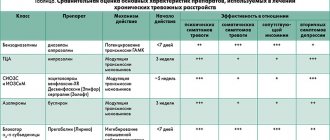
Parkinson's disease is the name of a slowly developing pathology of the central nervous system. The main symptoms of the disease include movement disorders, muscle rigidity (increased tone), tremors at rest.
Carriers of the pathology experience not only vegetative, but also affective disorders. Neurologists diagnose patients with true parkinsonism - Parkinson's disease - and parkinsonism syndrome. The latter becomes a complication of other neurological diseases: malignant brain tumors, strokes, encephalitis, etc.
Classification of pathology
The most widespread approach in neurology is based on the patient’s age at the time the first symptoms of Parkinson’s disease were detected. Based on this data, the following are distinguished:
- juvenile parkinsonism;
- pathology with early onset;
- disease with late onset.
An alternative approach to the classification of Parkinson's disease is based on the pattern of changes in the kinematics of movements of the upper and lower extremities of patients. In this case, parkinsonism syndromes are divided into tremulous, tremulous-rigid, rigid-tremor, akinetic-rigid and mixed.
Both classifications given are conditional. Neurologists still have not developed a unified approach to the types and forms of Parkinson's disease.
Causes
Accurate data on the causes of true parkinsonism have not been identified to date. The leading role in the development of the pathological process is given to genetic predisposition. They also note the importance of the impact of negative environmental factors (the effects of toxic substances, heavy metals and other causes), and also assign a significant role to the natural aging of the body.
In 15% of cases of this disease, a family predisposition can be traced. Genetic factors play a leading role in the case of early onset. In young people diagnosed with true parkinsonism and a family history of the disease, the following genes are found: PINK1, SNCA, LRRK2 PARK2. Their presence is obviously associated with the development of forms of the disease with an early onset.
Symptoms of pathology
Destructive processes in the central nervous system provoke the development of the main symptoms:
- tremor;
- rigidity;
- hypokinesia (limited mobility);
- violations of translational regulation.
True parkinsonism is characterized by recurrent or constant episodes of tremors. The pathology is characterized by a looped movement of the patient’s limbs at rest.
In the early stages of the syndrome, muscle rigidity remains relatively unnoticed. As other symptoms develop, constant muscle tone causes more and more discomfort to the patient. Asymmetry in muscle tension remains one of the main diagnostic markers in the early stages of Parkinson's disease.
Neurologists distinguish several stages in the development of pathology. In the educational literature for medical universities, the classification of Hoehn and Yahr is often given. Its basic provisions are presented in the table.
| Stage | Description |
| Zero | There are no motor symptoms of parkinsonism |
| First | Pathology manifests itself unilaterally |
| Second | A complex of bilateral symptoms is formed |
| Third | Noticeable translational instability develops, but the patient retains the ability to care for himself independently |
| Fourth | Rapid degradation of motor activity, the patient can only stand and move short distances without assistance |
| Fifth | The patient cannot leave the chair or bed without the help of doctors or relatives |
Symptoms and signs of Parkinson's disease are the same in women and men. Gender and age differences in the diagnosis of pathology turn out to be insignificant.
Are you experiencing symptoms of Parkinson's disease?
Only a doctor can accurately diagnose the disease. Don't delay your consultation - call
Physiotherapy
Physical education classes are conducted under the supervision of a rehabilitation specialist.
A set of exercises is formed taking into account the patient’s condition, the stage of Parkinson’s disease, and rehabilitation potential. All movements should be simple, without overexertion. Be sure to include a block of exercises that ensure muscle relaxation: without them, the tremors will intensify, movements will begin to slow down and become constrained, and the pain will increase. Doctors recommend doing physical therapy daily, gradually increasing the load, working all muscle groups. The exercises are performed in a free rhythm, supplemented with breathing exercises, and the state of health is monitored: it is important that after training a person feels pleasantly tired, but not exhausted. You have questions?
We will call you back within 30 seconds
or call the number
Clicking the "Submit"
, you automatically consent to the processing of your personal data and accept the terms of the User Agreement.
- Types of massage and their benefits
- Types of physiotherapy and its benefits
- Hardware physiotherapy
- Physiotherapy in rehabilitation, treatment and prevention
- Physiotherapy in anti-relapse treatment
- Physiotherapy in the treatment of addictions
- Benefits of Physical Therapy for Elderly Patients
- Physiotherapy for Parkinson's disease
Diagnostic measures
The diagnosis is made by a neurologist. It may take the doctor a significant amount of time to differentiate the diagnosis and conduct various functional tests.
Early-onset parkinsonism is characterized by severe limitation in movement with regular attacks of tremor (the frequency of oscillations of the limbs of patients is 4-6 Hz). The clinical picture is complemented by postural instability, which is not associated with cerebellar disorders or injuries received by the patient.
Diagnostic procedures include:
- EEG;
- rheoencephalography;
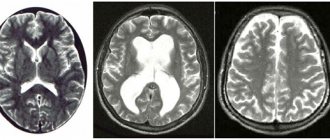
- computer and magnetic resonance imaging of the brain.
Mechanism of occurrence
The above list of pharmacological products in any case causes an inhibitory effect on the dopaminergic region of the brain. The main place is occupied by mechanisms that provoke blocking of the D2 receptor in the striatum and disruptions in the production of the hormone from the presynaptic zone. As a result, it turns out that acetylcholine processes begin to predominate in the human body, which activate the caudate nucleus in large quantities. The last point slows down the motor environment, which is noticeable in the form of a decrease in the number, speed and amplitude of an active lifestyle. According to the analyzes carried out, scientists found that the clinical picture of the presented pathological process begins when more than 75% of the receptors are blocked.
Also, do not forget about the hereditary predisposition to hidden hormone deficiency, which manifests itself during the additional effects of dopamine blockers from the medication used.
Treatment of pathology
Treatment strategies for Parkinson's disease depend on the stage at which the patient begins receiving the necessary therapy. For this reason, neurologists prefer to separate therapeutic approaches aimed at relieving early and late symptoms.
Treatment in the early stages involves the use of medications that stimulate the synthesis of dopamine in the brain. The therapeutic effect is achieved by stimulating dopamine releases and blocking reuptake. Thanks to this, it is possible to reduce the rate of neuronal death. Basic drugs can be used as part of complex treatment or as monotherapy. The combination of necessary substances is selected by a neurologist based on the clinical picture of parkinsonism and the individual characteristics of the patients.
Treatment of Parkinson's disease in the later stages remains an inevitable stage, since drug therapy can only slow down destructive processes. Progressive pathology is complemented by new symptoms that are difficult to relieve. At a certain point, the usual effectiveness of medications decreases. The patient experiences hypersensitivity of dopamine receptors and a kind of withdrawal syndrome due to the body's resistance to substances taken for a long time.
Against this background, doctors are forced to prescribe constantly increasing doses of medications to patients by reducing the intervals between doses. An alternative solution is to switch to a combination treatment regimen, which uses drugs from several groups. In some cases, surgery may be possible to implant an electrode into the patient that provides deep brain stimulation. This method allows you to stop resting tremor and restore motor activity in people suffering from Parkinson's disease.
Psychiatry Psychiatry and psychopharmacotherapy named after. P.B. Gannushkina No. 01 2006
Extrapyramidal syndromes are a group of movement disorders resulting from damage to the basal ganglia and subcortical-thalamic connections [1]. Neuroleptics can cause almost the entire spectrum of extrapyramidal disorders: parkinsonism, dystonia, tremor, chorea, akathisia, tics, myoclonus, stereotypies. Parkinsonism is a syndrome caused by damage to the basal ganglia and disruption of their functional connections; it is manifested by akinesia and rigidity, sometimes by resting tremor and postural disorders. According to statistics, from 4 to 15% of all cases of parkinsonism are associated with taking medications [2–4], most often antipsychotics. Its prevalence is especially high among patients in psychiatric clinics. Often, such patients are mistakenly diagnosed with Parkinson's disease and prescribed dopaminergic drugs, which does not give the desired effect and sometimes leads to an exacerbation of mental manifestations. At the same time, timely and adequate therapeutic opportunities are unused, which affects the quality of life of such patients, impairs their daily activity, affects the emotional sphere, and in some cases leads to loss of ability to work. Neuroleptic parkinsonism occurs on average in 10–15% of patients taking antipsychotics. The likelihood of developing parkinsonism when taking an antipsychotic is directly proportional to its ability to block M-cholinergic receptors and serotonin 5-HT2 receptors. Parkinsonism develops especially often when using potent D2 receptor blockers with weak anticholinergic activity and low affinity for serotonin receptors (haloperidol, fluorophenazine, triftazine). When using atypical antipsychotics (clozapine, olanzapine, quetiapine, etc.), due to their weak interaction with D2 receptors in the striatum (the activity of this group of drugs is due to the blockade of D4 receptors and serotonin receptors), the likelihood of developing parkinsonism is minimized. Parkinsonism can also develop when taking “mild” neuroleptics (prochlorperazine) [5]. The likelihood of developing parkinsonism is higher when using high doses of antipsychotics, especially the piperazine series; in the presence of background organic brain damage, a history of traumatic brain injury, or a hereditary predisposition to this complication [6]. In addition, risk factors include age, gender, and smoking. In older people, the antidopaminergic effect of antipsychotics is more pronounced, which has been confirmed by several studies [7]. Neuroleptic parkinsonism in most cases occurs in people over 40 years of age; in women – 2 times more often than in men [2]. Other possible risk factors include a family history of Parkinson's disease, previous motor disorders, early age of onset of schizophrenia in psychiatric patients, the presence of cognitive impairment, and diabetes mellitus [2]. The pathogenetic factors in the development of neuroleptic parkinsonism are not entirely clear. Neuroleptics block dopamine D2 receptors in the nigrostriatal system of the brain, which leads to inhibition of dopaminergic transmission and changes in the sensitivity of dopamine receptors. Neurochemical imbalance is manifested by increased activity of the cholinergic, serotonergic systems, as well as increased activity of glutamatergic subthalamic neurons, which leads to increased release of glutamate and activation of oxidative stress, which is one of the main factors contributing to damage to basal ganglia neurons. Due to their lipophilicity, antipsychotics have the ability to integrate into cell membranes and disrupt the energy metabolism of neurons. However, the often delayed neuroleptic side effect indicates that it is not solely due to immediate blockade of D2 receptors. As experimental studies show, with the blockade of postsynaptic D2 receptors, dopaminergic neurons of the substantia nigra (as well as neurons of the ventral tegmentum of the midbrain) gradually (over several weeks) stop discharging due to a depolarization block, which coincides in time with the development of parkinsonism [5]. The diagnosis of neuroleptic parkinsonism is established in accordance with the American classification DSM-IV (1994): A. The presence of one or more symptoms that appear during neuroleptic therapy:
- tremor (extremities, head, tongue);
- muscle rigidity with a plastic increase in muscle tone and the “cogwheel” symptom;
- akinesia.
B. Symptoms of group A appear within the first few weeks after the start of antipsychotic therapy or an increase in the dose of previously taken antipsychotics and decrease after the appointment of antiparkinsonian correctors.
C. Symptoms of group A should not be caused by a mental illness (catatonia, negative symptoms of schizophrenia, motor retardation during a major depressive episode, etc.). D. Symptoms of group A should not be caused by taking another drug, or by a neurological or somatic disease (Parkinson's disease, Wilson's disease, etc.). Currently, a number of works by foreign authors widely discuss the issue of the therapeutic effectiveness of amantadine and anticholinergic drugs (trihexyphenidyl, biperiden) in relieving extrapyramidal neuroleptic syndromes. A number of studies report equivalent effectiveness of biperiden and amantadine [8], others indicate greater effectiveness of amantadine in the correction of neuroleptic complications [9]. In a double-blind, placebo-controlled study conducted by W. Fann and C. Lake (1976), it was found that in the treatment of neuroleptic parkinsonism, amantadine at a dose of 200 mg/day is therapeutically equivalent to 8 mg/day of trihexyphenidyl. Amantadine caused significantly fewer and less severe side effects than trihexyphenidyl, although this difference did not reach the level of statistical significance [10]. At the same time, a number of advantages of amantadines over anticholinergics have been reported. Anticholinergics in standard clinical doses can worsen the cognitive functions of patients [11, 12]. Compared with anticholinergic drugs, cognitive functions in healthy [8, 13] and patients with schizophrenia [14] are preserved longer when treated with amantadine. In addition, anticholinergic drugs may reduce the antipsychotic effect of antipsychotics and lead to their abuse due to their anxiolytic properties and ability to induce euphoria [15]. Finally, they can produce changes in cardiac repolarization [16]. According to some researchers, anticholinergic drugs provoke the development of tardive dyskinesia [12, 15, 17]. One report from the American Psychiatric Association indicates that amantadine is effective in the treatment of tardive dyskinesia (1992). Improvement was observed in all 6 patients receiving amantadine and antipsychotics, and improvement was achieved with the abolition of anticholinergic drugs. At present, the factors that increase the risk of developing neuroleptic extrapyramidal disorders and the features of the clinical picture of neuroleptic parkinsonism have not been studied in detail. The subject of special attention and discussion are methods for correcting this complication. The purpose of the work was to study the characteristics of the clinical manifestations and course of neuroleptic parkinsonism, as well as to determine approaches to its correction. Material and methods
The study included 90 patients diagnosed with paranoid schizophrenia (in accordance with ICD-10 criteria), who developed parkinsonism syndrome while taking antipsychotics. Clinical assessment of the patients' condition included a study of neurological and somatic status with objectification of existing neurological disorders using the Hoehn & Yahr scale as modified by Lindvall (1988), Tetrud and Langston (1989); UPDRS scales, version 3 (S. Fahn et al., 1987). Clinical assessment was carried out before the start of correction of the complication, during therapy, and after 1 month of therapy. The duration of subsequent corrective therapy was determined by the rate of regression of the neuroleptic complication. Amantadine sulfate and trihexyphenidyl were used as correctors. Amantadine sulfate is an antagonist of NMDA receptors for glutamate, which is an excitatory neurotransmitter. When treated with amantadine sulfate, the predominance of the glutamatergic system and the level of acetylcholine in the striatum decrease, the synthesis of dopamine in presynaptic terminals and its release into the synaptic cleft increases. The average daily dose of amantadine sulfate was 300 mg/day. The mechanism of action of the anticholinergic trihexyphenidyl is to reduce the functional activity of cholinergic systems and restore neurotransmitter imbalance. The average daily dose of trihexyphenidyl was 7.5 mg/day. The research results were processed using the statistical program Statistica 6.0 using the Student's t test, c2 goodness-of-fit test, U test, non-parametric sign test, rank correlation analysis (according to Spearman). All data below are presented in the form M±d.
Results and discussion
90 patients (34 men, 56 women) with neuroleptic parkinsonism were examined.
The average age of the patients was 45.7±15.5 years. The average duration of treatment with antipsychotics was 143.3±121.9 months (from 1 month to 35 years). The severity of parkinsonism on the Hoehn–Yahr scale was 2.5±0.5 points. All examined patients took antipsychotic drugs in average therapeutic daily doses for their underlying mental illness. Of the typical antipsychotics, the most frequently used were aliphatic phenothiazine derivatives (n=37), piperazine phenothiazine derivatives (n=44), pipedine phenothiazine derivatives (n=16), butyrophenone derivatives (n=49), thioxanthene derivatives (n=36), substituted benzamides (n=6). Each patient received combinations of these drugs with each other and with atypical neuroleptics, of which benzisocoxazole derivatives (n=17), dibenzodiazepine derivatives (n=25), and long-acting forms of neuroleptics (n=35) were used. Some patients received antipsychotics in combination with tricyclic antidepressants (n=21), tranquilizers (n=16), and lithium preparations (n=3). Neuroleptic parkinsonism was noted significantly more often (p<0.05) in women than in men (1.6 times). A positive correlation was found between the age of patients (R=0.3; p=0.002), the duration of neuroleptic therapy (R=0.4; p=0.0006) and the timing of the onset of parkinsonism. The clinical picture of neuroleptic parkinsonism was in many ways similar to the manifestations of Parkinson's disease and was characterized by the same basic symptoms (hypokinesia, rigidity, tremor, postural instability). Hypokinesia and muscle rigidity were detected in all patients, rest tremor was noted in 26 (34.4%) patients, and postural instability – in 46 (44.6%). Hypokinesia
in patients with neuroleptic parkinsonism was the earliest manifestation of parkinsonian syndrome, predominant in the distal parts of the extremities, dominated over rigidity, and was characterized by a moderate or significant degree of severity.
Rigidity
developed later than hypokinesia, was manifested by a plastic increase in muscle tone in the muscles of the limbs, axial muscles, and regressed more quickly against the background of antiparkinsonian therapy.
Tremor
in neuroleptic parkinsonism was somewhat different from tremor in Parkinson's disease.
It was characterized by symmetry and more often had a postural-kinetic character; Resting tremor was observed somewhat less frequently. In 1 patient, a tremor was detected that covered only the perioral area and resembled the chewing movements of a rabbit - “rabbit syndrome”. In the structure of parkinsonism syndrome, tremor was the most rare symptom and was of an unstable nature. Postural instability
was manifested by impaired ability to maintain balance, as well as falls and walking disorders. Postural instability was observed in 76 patients; in 63% of patients – retropulsion. Falls were noted in 19% of patients, and 2% of patients even required outside assistance. Thus, in almost half of the cases there were violations of postural stability, however, as a rule, they were of a minor nature and were not dominant in the structure of neuroleptic parkinsonism. Walking was also less affected; a hunched posture and a mincing, shuffling gait were not characteristic of such patients (Table 1).
Frequency of occurrence of extrapyramidal neuroleptic syndromes.
Table 1. Severity and frequency of the main symptoms of neuroleptic parkinsonism (n=90)
| Main symptoms of parkinsonism | Degree of severity, points (M±s) | Frequency of occurrence, % |
| Hypokinesia | 16,3±8,2 | 100 |
| Rigidity | 9,6±4,4 | 100 |
| Rest tremor | 6,7±4,1 | 31 |
| Postural-kinetic tremor | 3,9±1,9 | 35 |
| Postural instability | 1,3±0,6 | 84 |
Table 2. The severity of clinical manifestations of parkinsonism syndrome in patients with neuroleptic parkinsonism with varying degrees of severity (Hoehn–Yahr UPDRS scale, part III)
| Severity of parkinsonism according to the Hoehn–Yahr scale, points | Clinical manifestations of parkinsonism syndrome according to the UPDRS scale (Part III) | |||
| hypokinesia | rigidity | tremor | total score | |
| 2,0–2,5 | 8,1±3,3 | 13,1±5,8 | 4,9±3,6 | 29,5±10,1 |
| 3,0–3,5 | 14,2±2,9 | 26,2±5,2 | 6,5±5,3 | 48,4±11,4 |
| 4,0 | 19,3±1,2 | 33,7±3,2 | 8,0±6,4 | 68,0±2,0 |
Table 3. Evaluation of the effectiveness of amantadine sulfate (PC-Merz) in relieving the manifestations of neuroleptic parkinsonism (n=30)
| Symptoms of parkinsonism (UPDRS scale, part III) | Points (M±d) | Improvement, % | |
| before treatment | after treatment | ||
| Hypokinesia | 19,2±9,2 | 9,4±6,6** | 53 |
| Rigidity | 9,6±5,5 | 3,5±3,3** | 64 |
| Tremor | 5,4±2,8 | 2,5±1,8* | 54 |
| Postural instability | 1,8±0,9 | 0,9±0,5* | 50 |
| Total score | 37,6±15,7 | 15,5±10,6** | 58,8 |
| Note. Here and in the table. 4: * – p<0.05; ** – p<0.01. | |||
Table 4. Evaluation of the effectiveness of trihexyphenidyl (cyclodol) in relieving the manifestations of neuroleptic parkinsonism (n=70)
| Symptoms of parkinsonism (UPDRS scale, part III) | Points (M±d) | Improvement, % | |
| before treatment | after treatment | ||
| Hypokinesia | 15,2±7,6 | 11,6±6,7** | 23,7 |
| Rigidity | 9,6±3,9 | 6,2±3,6** | 35,4 |
| Tremor | 7,0±6,4 | 5,2±4,8** | 25,7 |
| Postural instability | 1,2±0,4 | 1,1±0,3 | 8,3 |
| Total score | 33,1±13,2 | 23,4±13,3** | 29,3 |
Table 5. Frequency (in%) of side effects of trihexyphenidyl and amantadine sulfate during the correction of neuroleptic parkinsonism (n=90)
| By-effect | Trihexyphenidyl | Amantadine sulfate |
| Dry mouth | 92 | – |
| Constipation | 80 | – |
| Urinary retention | 20 | – |
| Visual impairment | 5 | – |
| Livedo reticularis | – | 4 |
| Anxiety | – | 12 |
| Dizziness | – | 20 |
| Exacerbation of psychotic symptoms | 8 | – |
Table 6. Comparison of the effectiveness of amantadine sulfate and trihexyphenidyl in the treatment of neuroleptic parkinsonism
| Amantadine | Trihexyphenidyl |
| More effective in correcting movement disorders | Less effective in correcting movement disorders in |
| for parkinsonism | parkinsonism |
| Does not reduce the antipsychotic effect of neuroleptics | Reduces the antipsychotic effect of neuroleptics |
| Does not cause cognitive impairment | Causes cognitive impairment |
| Rarely causes side effects | Often causes side effects |
| According to experimental studies, it may have a neuroprotective effect | Has no neuroprotective effect |
Table 7. Effect of therapy with amantadine sulfate and trihexyphenidyl on indicators of quality of life and daily activity in patients with neuroleptic parkinsonism (n=90)
| Scale | Improvement, % | |
| trihexyphenidyl | amantadine sulfate | |
| UPDRS (Part II) | 50,4 | 63,0 |
| PDQ-39 | 20,1 | 30,2 |
| EUROQoL (Part II) | 29,6 | 30,2 |
In most patients, the severity of parkinsonism on the Hoehn-Yahr scale was 2–2.5 points (Table 2). The following clinical forms of neuroleptic parkinsonism were identified in the examined patients: 79% – akinetic-rigid, 20% – rigid-tremor, 11% – akinetic-rigid-tremor (mixed). As the duration of neuroleptic therapy increased, the incidence of tremulous forms of parkinsonism increased. The majority of patients (88%) had symmetrical parkinsonism, only in 12% of cases there was a predominance of motor symptoms on one side. In all patients, symptoms of parkinsonism developed quickly: in 17% of patients - acutely (symptoms appeared within 1-2 days); in 83% of patients - subacutely (increasing movement disorders were observed over a period of weeks). In 53 (59%) patients, a combination of parkinsonism syndrome with other neuroleptic extrapyramidal disorders was observed (see figure). The frequency of occurrence of syndromes exceeded 100%, since many patients simultaneously had a combination of them. In this study, follow-up observation of patients for 2 years allowed us to identify the following types of course of neuroleptic parkinsonism: – rapidly regressive
, in which within 1 month of treatment, while reducing the dose of a typical and/or prescribing an atypical antipsychotic in combination with a corrector (anticholinergic, amantadine), symptoms regressed by more than 50%;
– slowly regressing
, in which within 1–6 months of treatment, while reducing the dose of a typical and/or prescribing an atypical antipsychotic in combination with a corrector (anticholinergic, amantadine), symptoms regressed from 20–50%;
– inpatient
, in which, against the background of a reduction in the dose of a typical and/or prescription of an atypical antipsychotic in combination with a corrector (anticholinergic, amantadine), there was no or slight regression of symptoms up to 20% within 6 months of treatment. A slowly regressive type of parkinsonism was noted in 40% of cases, a rapidly regressive type of course was identified in 36% of cases, and a stationary course of parkinsonism was identified in 24% of cases. The higher the age of patients with neuroleptic parkinsonism, the longer the duration of neuroleptic therapy, the more often the stationary type of this syndrome occurred in patients (R<0.4; p<0.01). Significantly more often (p<0.05) the rapidly regressing type of parkinsonism occurred in patients with the akinetic-rigid form (40%) than in patients with the mixed form (15%). Regression of parkinsonism symptoms caused by taking atypical neuroleptics was more pronounced and occurred earlier after reducing the dose of drugs or stopping them.
Approaches to the correction of neuroleptic parkinsonism
Correction of parkinsonism syndrome was carried out in accordance with the general principles of treatment of neuroleptic complications: if possible, discontinuation of the drug that caused the complication (n=10), or reduction of its dose (n=36), or prescription of an atypical neuroleptic (n=86), or replacement of one atypical antipsychotic to another (n=5). The same patient was often simultaneously reduced in dose of a typical antipsychotic and prescribed an atypical antipsychotic. The majority of patients (n=70) received infusion therapy, which included intravenous drip administration of 5% glucose, B vitamins, ascorbic acid, piracetam 20% - 10 ml, Riboxin - 10 ml; some patients were administered aminophylline 2.4% - 10 ml. In addition to this therapy, patients were prescribed an anticholinergic and/or amantadine.
Comparative assessment of the effectiveness of amantadine sulfate (PC-Merz) and the anticholinergic trihexyphenidyl (cyclodol) in the correction of neuroleptic parkinsonism
Amantadine sulfate and trihexyphenidyl were used to correct neuroleptic parkinsonism in this study.
Neuroleptics block dopamine D2 receptors in the nigrostriatal system of the brain, which is accompanied by inhibition of dopaminergic transmission and changes in the sensitivity of dopamine receptors. A neurochemical imbalance develops, which is manifested by an increase in the activity of the cholinergic and serotonergic systems, as well as an increase in the activity of glutamatergic subthalamic neurons. This results in increased release of glutamate, which is an excitatory neurotransmitter. At the same time, the influx of calcium ions into neurons increases, the level of acetylcholine in neurons of the striatum increases, cholinergic systems are activated and tremor, rigidity, and hypokinesia appear. Increased calcium concentrations in nigrostriatal neurons contribute to the degeneration of these neurons and the activation of oxidative stress, which is one of the main factors contributing to damage to basal ganglia neurons. The excitatory effect of glutamate is mediated through N-methyl-D-aspartate receptors (NMDA receptors). Due to their lipophilicity, antipsychotics have the ability to integrate into cell membranes and disrupt the energy metabolism of neurons. Amantadine sulfate
is an antagonist of NMDA glutamate receptors, through which the excitatory effect of the latter is carried out;
reduces the predominance of the glutamatergic system, the level of acetylcholine in the striatum; increases the synthesis of dopamine in presynaptic terminals and its release into the synaptic cleft, inhibits the reuptake of dopamine into the presynaptic terminal, stimulates DA receptors; indirectly reduces the concentration of calcium ions in nigrostriatal neurons, as a result of which it may have a neuroprotective effect [9, 18]. The mechanism of action of anticholinergics is to reduce the functional activity of cholinergic systems and restore the balance of the dopaminergic and cholinergic systems in the basal ganglia that is disturbed due to dopamine deficiency, blocking the reuptake of dopamine from the synaptic cleft (Table 3, 4) [1]. Analysis of the results showed a significant advantage of amantadine sulfate over trihexyphenidyl in the treatment of major movement disorders caused by neuroleptic parkinsonism. Unlike trihexyphenidyl, amantadine sulfate reduced the severity of postural and gait disorders. In order to assess the safety of treatment, the frequency of side effects of pharmacotherapy was analyzed (Table 5). Thus, amantadine sulfate, when relieving neuroleptic parkinsonism, caused fewer side effects than trihexyphenidyl. In general, a number of advantages of amantadine sulfate over trihexyphenidyl in the correction of neuroleptic parkinsonism can be noted (Table 6). Amantadine sulfate significantly improved indicators of daily activity (UPDRS scale, part II) and quality of life (PDQ-39 scale and EUROQoL scale, part II) compared with trihexyphenidyl (Table 7). Thus, this study identified a number of features that distinguish neuroleptic parkinsonism from Parkinson’s disease. Neuroleptic parkinsonism develops subacutely, less often acutely, usually within 1–2 weeks after starting antipsychotic therapy or increasing its dose. Its development is more frequent in women, mainly after 40 years. The clinical picture is dominated by symmetry of manifestations. Hypokinesia may be its earliest and sometimes only manifestation. Classic resting tremor is less common than postural-kinetic tremor, which in turn is characterized by symmetry. Neuroleptic parkinsonism is not characterized by severe postural disturbances; gait disturbances and falls are rare. A characteristic feature of neuroleptic parkinsonism is its combination with a variety of dyskinesias and dystonias. When the antipsychotic is discontinued or its dose is reduced, the manifestations of parkinsonism usually regress within a few weeks. However, some patients experience a slower decrease in movement disorders or their stationary course, which is usually observed in patients with a history of organic pathology and treatment with long-acting forms of neuroleptics. Risk factors for the development of neuroleptic parkinsonism are the elderly age of patients and long duration of neuroleptic therapy. Treatment of neuroleptic parkinsonism with amantadine sulfate leads to a more significant and earlier regression of the main symptoms of neuroleptic parkinsonism, does not affect the cognitive functions of patients and does not reduce the antipsychotic effect of neuroleptics. In addition, amantadine sulfate causes side effects significantly less often and statistically significantly improves the quality of life and daily activity of patients.
Questions and answers
Can true parkinsonism be cured?
Modern pharmacology and medicine do not have the means to completely cure Parkinson's disease. The treatment regimens used are aimed at slowing down destructive changes, relieving the main symptoms and improving the quality of life of people suffering from parkinsonism. Treatment methods for Parkinson's disease and the causes of this pathology are still being closely studied by the world's leading scientists. It is possible that in the foreseeable future there will be a breakthrough in medicine.
How to predict the life expectancy of a patient with Parkinson's disease?
The prognosis is formed by the attending physician based on the clinical picture, chronic pathologies of the patient and the results of diagnostic procedures. Assessing the prospects for treatment is a difficult task, since neurologists cannot predict in advance the human body's response to drug therapy.
Is it possible to eliminate the possible causes of Parkinson's disease in youth and avoid the development of pathology in adulthood?
Neurologists believe that parkinsonism is a genetically determined pathology. For this reason, the development of an effective set of preventive measures is not possible. Note that the symptoms and signs of Parkinson's disease in the early stages remain insufficiently pronounced to take emergency measures.
Diagnosis of parkinsonism at the Yauza Clinical Hospital
The Department of Neurology of the Yauza Clinical Hospital carries out a comprehensive diagnosis of parkinsonism.
Despite the fact that this disease has a number of characteristic external manifestations, in order for the doctor to have comprehensive information about the patient’s condition, laboratory diagnostics are necessary: general and clinical blood tests; determination of blood glucose, cholesterol, bilirubin, creatinine, beta-lipoproteins, triglycerides.
Also, to examine patients with suspected parkinsonism, instrumental diagnostics are used: electromyography, which allows you to determine the cause of tremor and exclude muscle diseases, and electroencephalography to diagnose disorders of brain activity. Plus, to diagnose parkinsonism, specialists from the neurology department of the Yauza Clinical Hospital refer patients to MSCT of the brain, neck vessels and cerebral vessels with contrast; MRI of the brain; MR angiography of intracranial arteries and vessels of the neck.
The examination is carried out in a complex manner, so the patient is also referred for consultation to specialists (ophthalmologist, physiotherapist and others).
Prognosis and prevention of Parkinson's disease
Today, this disease remains incurable. Today doctors cannot offer drugs that can restore the structure of the brain. The prognosis of development is related to the age of the patient and the presence of concomitant diagnoses.
The severity of symptoms makes it possible to reduce timely diagnosis and prescribe effective therapy. The development forecast depends on:
- age of first manifestations, the younger, the more strength the body has to resist rapid development with frequent attacks leading to the death of neurons;
- prospects for the use of modern drugs, including Levodopa. Today in the Russian Federation this drug is included in the list of medications prescribed to federal beneficiaries under SNILS;
- the possibility of using innovative surgical methods, most often offered to young and middle-aged patients who are able to withstand surgery.
Due to the lack of accurate data on the causes of the onset of Parkinson's disease, exact methods of prevention are also unknown. But to reduce risks, it is recommended to lead a healthy lifestyle and stop taking drugs and alcohol. Regular medical examinations become an important prevention option.