04.01.18
Why do children with autism resort to stereotypic behavior (stimming) to self-soothe, and how to help them avoid harmful stereotypies
Author: Karen Wang / Karen Wang Source: Friendship Circle
Each of us has motor stereotypies. When I talk to my friend, I twirl my hair on my finger. Maybe you start biting your nails when you're nervous or bored. Maybe you have a habit of tapping your fingers or pen on the table when you are thinking. I had a friend who liked to chew cinnamon sticks, and I know someone who makes unusual eye movements.
There are people whom I recognize from afar by their characteristic movements. We all know people with annoying stereotypes, such as cracking their knuckles every 5 minutes, repeating the same phrase over and over again, or socially unacceptable stereotypes such as picking their nose or biting their hand.
What is stereotypy
Stereotyping is any purposeless, repetitive movement, sound or word. In autism they are present in the vast majority of cases. My son's neurologist calls them "autistic stereopathies." They are also called “self-stimulation” or, in colloquial language, “stimming”.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, includes stereotypy as one of the diagnostic criteria for autism spectrum disorder: “Stereotypical or repetitive motor movements, use of objects, or speech.” The guidelines also state that the diagnostic criteria are: “Symptoms that cause clinically significant difficulties in social functioning, employment, and other important areas of current functioning.”
This is the difference between autistic stereotypies and ordinary stereotypies. It is a symptom of autism only when stereotypies interfere with everyday tasks and learning.
Diagnostics
The diagnostic program includes the following activities:
- visual examination of the child;
- clarification of the current clinical picture, collection of personal and family history;
- studying the patient's medical history.
In addition, additional laboratory and instrumental research methods may be required:
- general and biochemical blood test;
- CT, MRI of the brain;
- psychiatric tests.
Carrying out a computed tomography scan for a child.
You may need to consult a neurologist, ophthalmologist, otolaryngologist, child psychologist, or speech therapist.
Wrong question
“How to stop stereotyping?” This is usually the first question parents ask when a young child discovers stimming. And this is the wrong question.
First, all people have self-stimulating behavior, so it is basically impossible to completely stop it. Secondly, even if you get rid of one stereotype, another will replace it - and there is a risk that the next stereotype will be much more problematic.
And most importantly, your attempts to stop stereotyping may make your child want to avoid you and communication with you, as a result, you will lose opportunities for social interaction.
Recommendations for raising a skin-sound child with autism
First of all, you need to remember the mechanism of autism formation. This happens through trauma in the development of the sound vector. Therefore, the first and main condition for raising any autistic child will be a “sound ecology” in the home.
Minimize the amount of household noise: from the operation of electrical appliances, loud music and the sound of a working TV. If your home is located above a road along which traffic flows, it is better to get soundproofing or even change your place of residence. Parents need to speak quietly, gently and calmly among themselves and with the child. No offensive meanings in speech should also be allowed.
As for the peculiarities of raising a skin-sound autistic person, first of all you should remember that it is absolutely forbidden to not only beat, but even lightly spank such children. The skin is a particularly sensitive area; even minimal stress can lead to disastrous results.
As a rule, parents who are not familiar with the “System-Vector Psychology” training by Yuri Burlan do exactly the opposite. Of course, it is difficult for them to perceive such a huge number of stereotypical movements in a child, and they try to stop them in the simplest way - to spank them on the arms, legs, back, or “whatever else he twists and turns.” Such upbringing leads to the fact that, even if by a miracle the child was able to stop making just such movements, they are replaced by ten new, even more elaborate ones.
Valid question
“Why is my child engaging in this behavior?” It is always better to start by looking for the cause and understanding the motivation behind the behavior. Here are some possible reasons and hypotheses to explain stereotypies:
Overstimulation: Stereotypes help block out unnecessary sensory information from the outside world and avoid overload.
Insufficient stimulation: Stereotypes can provide additional sensory stimulation when needed.
Reduce Pain: Repeatedly hitting the head or body can reduce the overall feeling of pain. It is hypothesized that stereotypies release beta-endorphins, which act as an anesthetic or induce pleasure.
Managing Emotions: Both negative and positive emotions can cause a “surge” of stereotypies. We've all seen reactions to joy or delight such as jumping or shaking our hands. Dissatisfaction or anger can increase stereotypies to the point where they become dangerous.
Self-regulation: Some stereotypies are a way to self-comfort or calm down. So many babies suck their fingers to relax.
Not long ago I read on one mother’s blog that she did not understand why her son covered his ears with his hands in his sleep. He began to cover his ears when things were too noisy, and this calmed him down. So he started covering his ears whenever he needed to calm down, including when he fell asleep.
How to reduce stereotypies
Here are some ideas on how you can reduce your time spent on stereotyping while developing your communication skills:
- Medical examination to rule out physical causes of stereotypies, for example, ear infections, chronic pain, migraines, retinal detachment.
— Improving the sensory and emotional environment so that the child is more comfortable and the need for self-comfort is reduced.
— Sports, exercise and other intense physical activity reduce stereotypies. This may be due to the fact that exercise releases beta-endorphins, as does stereotypy.
— Continue communication, even if stereotypes arise. James MacDonald suggests that people with autism perceive the world around them more through sensations and actions, while neurotypicals perceive the world more through thoughts and language. If you understand this difference, then stereotypes become more meaningful. MacDonald recommends doing different activities in turn, without trying to stop the child’s stereotypies, just involving him in the activity is enough. Gradually, joint activities will become more familiar and attractive for the child, and this will naturally reduce stereotypy.
— Creating a positive association between stereotypy and social interaction. One way to use stereotypy for learning is to allow stereotypy as a reinforcer or reward after a short period of playing or working together. Julia Moore believes that if you set aside a scheduled time for stimming after communication, this will allow the child to be himself, motivate him to communicate more often, and at the same time, the total time he spends on stereotypies will decrease.
— Join the stereotype! Some approaches ask adults to engage in self-stimulating behavior to initiate communication. For example, if your child is spinning plates, start spinning the plates too. If your child is rocking, start rocking next to him too. My son would “stimulate” by raising his hand and talking to her as if he were looking in a mirror. He was delighted when I started doing this with him!
You can then add new things to your interaction, such as gestures so your child can ask for what he wants. The basic principle is to offer the child experiences that will produce similar sensations to stereotypy, but that are more functional and will promote greater self-regulation.
In other words, to reduce stereotypy, offer a replacement that is more attractive!
Speech stereotypies and psychoneurological diseases
The causes of speech stereotypies often lie in the development of neurological and psychological diseases.
Causes of perseverations
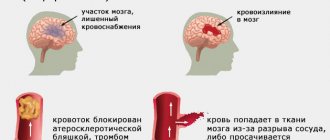
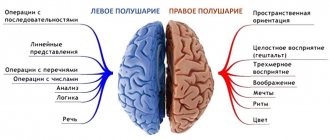
Experts believe that the cause of perseveration is damage to the lower parts of the premotor nuclei of the cortex of the left hemisphere in right-handers, and the right hemisphere in left-handers.
The most common cause of perseveration is considered to be neurological diseases resulting from physical damage to the brain. In this case, it becomes impossible to switch between different activities, changing the train of thought and the order of actions when performing various tasks.
With the neurological nature of the disease, the causes of perseveration are:
- Traumatic brain injuries , in which the lateral orbitofrontal areas of the cortex and its prefrontal convexities are affected.
- Aphasia is the appearance of disturbances in speech formed at a previous stage of life. These disorders arise due to physical damage to the speech centers, as a result of traumatic brain injury, encephalitis, and brain tumors.
- Pathologies related to the area of the frontal lobes of the cerebral cortex.
Psychiatry and psychology classify perseveration as a symptom of various phobias and anxiety syndromes. The course of this speech stereotypy in the psychological and psychiatric direction can be caused by:
- obsessiveness and selectivity of individual interests, which is most often found in people with autistic disorders;
- lack of attention with hyperactivity, while stereotypy arises as a defense mechanism to attract attention to oneself;
- a steady desire to learn and experience new things can lead to fixation on one conclusion or activity;
- Perseveration is often a symptom of obsessive-compulsive disorder.
Perseveration should not be confused with obsessive-compulsive disorder, human habits, and sclerotic changes in memory.
Perseverations are more often observed in patients with dementia (dementia), which is caused by vascular damage to the brain, as well as with age-related atrophic processes in the brain. The patient’s intellect is impaired, and he cannot understand the question being asked and, instead of a logical answer, repeats previously used phrases.
What provokes the development of verbigeration?
With verbigeration there is no connection with certain neuropsychic conditions. One of the features of verbigeration is that the patient pronounces words without showing emotion. As a rule, verbal repetitions are accompanied by active facial expressions and motor disturbances.
Most often, these verbal iterations occur in patients with dementia and catatonic schizophrenia.
Causes of standing revolutions, palilalia and echolalia
The appearance of standing phrases in speech signals a decrease in intelligence and empty thinking.
They often appear with a disease such as epileptic dementia. Also, one of the diseases characterized by standing movements is Pick's disease, as well as other atrophic diseases of the brain. Palilalia is a typical manifestation of Pick's disease. It is also often accompanied by diseases such as striatal pathology, striopallidal pathology (atrophic, inflammatory, vascular), postencephalic parkinsonism, pseudobulbar syndrome, catatonia, Tourette's syndrome, schizophrenia.
The occurrence of echolalia is often associated with damage to the frontal lobes of the brain. If the patient has symptoms such as hallucinations, lack of coordination, and forgetfulness, it is necessary to seek advice from a specialist. If brain damage is not diagnosed, then the causes of echolalia may be imbecility, schizophrenia, autism, Asperger's syndrome, Tourette's syndrome.