By etiology:
- Infectious;
- Infectious-allergic (for childhood exanthema infections: measles, rubella, etc.);
- Toxic;
- Allergic (vaccinal, serum, etc.);
- Dysmetabolic: with vitamin deficiency, with endocrine diseases (diabetes mellitus), etc.;
- Discirculatory: for rheumatic and other vasculitis;
- Idiopathic and hereditary (neural amyotrophy of Charcot-Marie, etc.);
- Compression-ischemic lesions of individual peripheral nerves;
- Vertebrogenic lesions (bone, disc, joint, muscle and tendon-ligament formations).
Diseases of the peripheral nervous system of various etiologies can be primary (Guillain-Barré polyneuritis, leprosy, syphilis, leptospirosis, etc.) and secondary (vertebrogenic, after childhood exanthemal infections, infectious mononucleosis, periarteritis nodosa, rheumatism, etc.).
Neuralgia is painful sensations in the area of innervation of certain nerves and the formation of trigger zones of the skin and mucous membranes, irritation of which, for example, touch causes another attack of pain. In the intervals between attacks, neither subjective nor objective symptoms of irritation or loss of function of the affected nerve are observed.
The most common symptoms of damage to the peripheral nervous system:
- viral (Guillain-Barré polyneuritis, viral diseases, influenza, sore throat, infectious mononucleosis, etc.);
- microbial (for scarlet fever, brucellosis, syphilis, leptospirosis, etc.);
- for chronic intoxication (alcoholism, manganese, lead, etc.);
- for toxic infections (botulism, diphtheria);
- blastomatous (for lung cancer, stomach cancer, etc.);
- sensory disturbances (pain, numbness, feeling of fullness, “crawling”, increased or decreased sensitivity of certain areas);
- movement disorders (weakness, impaired motor function of the limbs, facial muscles and eyes);
- vegetative disorders (dry or wet hands and soles, cold extremities).
Symptoms of polyneuropathy
The main clinical manifestation of polyneuropathy is the presence of motor disorders, as well as sensory and autonomic disorders. In most cases, polyneuropathy affects the longest nerve fibers. That is why the symptoms of the disease initially appear in the distal parts of the extremities. Due to the diffuse nature of damage to nerve fibers, a symmetrical manifestation of symptoms is noted.
During the development of polyneuropathy in a person, a violation of sensitivity occurs, with the manifestation of vegetative and motor symptoms. The most common motor dysfunction in a patient with polyneuropathy is paresis , accompanied by hypotension and muscle wasting. Paresis is most often observed in the extremities. In severe cases of the disease, the muscles of the trunk and skull are involved in the process. It is customary to distinguish between two types of symptoms in polyneuropathy: negative and positive symptoms. Negative symptoms are hypoesthesia, weakness and subsequent muscle weakness, sensitive ataxia (coordination of movements is impaired), weakened gastrointestinal motility, weak pulse, strong or weak sweating, impotence . Positive symptoms are tremor, neuromyotonia, fasciculations, paresthesia, pain and restless legs syndrome, high blood pressure, tachycardia , intestinal colic.
Sensory disturbances in polyneuropathy can be very diverse. Thus, sensitivity can either decrease or be completely absent. Paresthesia (tingling sensation and goosebumps), as well as pain of a different nature, are periodically observed. Thus, painful sensations can manifest themselves as a response to a non-painful stimulus. In addition, pain may be spontaneous.
Also a sign of polyneuropathy is neuralgia , manifested by pain at the site of innervation of the nerve. As a rule, it is usually a piercing or shooting pain. Causalgia also appears . This is a burning and persistent pain that develops at the site of innervation of the nerve due to its damage. In this case, various autonomic disorders often develop, and tissue nutrition is disrupted.
Another manifestation of polyneuropathy associated with the autonomic nervous system is erectile dysfunction in men, which is characterized by erectile dysfunction and the inability to perform normal sexual intercourse.
Diagnosis of diseases of the peripheral nervous system:
Methods for diagnosing diseases of the peripheral nervous system are aimed at identifying and correcting the underlying disease (for example, damage to peripheral nerves in diabetes mellitus requires correction of the underlying disease). An X-ray examination is carried out to identify the severity of degenerative-dystrophic changes in the spine, which are most often the causes of pain and discomfort in the back and limbs, to exclude pathological changes in bone tissue (including fractures).
For some pathologies, an MRI study may be indicated, which is aimed at identifying a pathological process that interferes with the normal functioning of the nerve fiber: for example, radiculopathy due to compression of the nerve root by an intervertebral hernia, neuromas, identifying congenital anomalies, etc.).
Classification
Assessing the course of the disease, experts distinguish between acute , subacute and chronic polyneuropathies. In the acute form of the disease, its symptoms become most pronounced several days or weeks after the onset of the disease. Subacute polyneuropathies are characterized by an increase in symptoms over several weeks. But at the same time they take place no more than two months. Chronic polyneuropathies can develop over several years.
There are also toxic polyneuropathies (another name for the disease is Guillain-Barre syndrome ), in which a monophasic course is observed. Consequently, the symptoms worsen once, after which the disease gradually regresses. Initially, the patient may show signs of an infectious gastrointestinal or respiratory disease.
There are also porphyritic polyneuropathy and inflammatory demyelinating polyneuropathy , which occur with periodic relapses and remissions. When the next exacerbation of the disease occurs, the neurological defect becomes more profound each time.
With axonal polyneuropathies, the disease develops gradually, and first of all, the distal parts of the legs are involved. With this type of polyneuropathy, trophic changes very quickly appear in the patient’s muscles, pain, and impaired autonomic functions are bothersome. The patient has sensory and motor impairment.
With demyelinating polyneuropathies, the patient exhibits early tendon reflexes. The sensitivity of muscles and joints is impaired. Both the proximal and distal parts of the limbs are involved in the process, with paresis more pronounced, but muscle atrophy manifests itself less.
Treatment of diseases of the peripheral nervous system:
Treatment of these diseases includes medication, non-drug and surgical treatment. Drug therapy is aimed at correcting the underlying disease:
- Non-steroidal anti-inflammatory drugs (NSAIDs) are used to relieve pain.
- To normalize vascular tone and improve blood circulation, suitable vascular therapy is selected
- A course of vitamin therapy is prescribed to improve nerve conduction
- Recommended medications to normalize muscle tone
- and other medications, the selection of which is based on a specific pathology
Non-drug therapy includes the use of physiotherapeutic treatment methods, the selection of which depends on the specific pathology, the severity of the process and concomitant pathology:
- reflexology
- massage
- hirudotherapy
- ozone therapy
- osteopathy and manual therapy
As for surgical treatment methods, they are used in case of long-term persistent neurological defect and ineffectiveness of conservative therapy, or in acute conditions and there are absolute indications for surgical treatment.
For the best result from treatment, it is necessary to contact a neurologist for a face-to-face consultation as early as possible from the onset of the disease; the doctor will develop an individual treatment and examination regimen.
Peripheral nerve injuries
According to the nature of the damage, peripheral nerve injury is classified as compression (compression), concussion, contusion (bruise) and anatomical break. The latter can be partial (incomplete), complete and intra-barrel. With a partial and intra-trunk break, the possibility of spontaneous regeneration of the nerve remains due to the ingrowth of the axons of the terminal sections of its central segment into the peripheral section. The rate of this process is 1 mm per day. Significant nerve damage leads to scar formation and conduction disturbances distal to the injury site. A complete anatomical break with divergence of the ends or the presence of an obstacle between the formed segments of the nerve in the form of a bone fragment, scar, or foreign body causes the development of neuroma. A neuroma can also result from a bruise of the nerve trunk or hemorrhage into it.
On the other hand, all nerve injuries are divided into open, which most often leads to an anatomical break of the nerve, and closed, in which concussion, compression or bruise of the nerve is possible. Open injuries include various wounds: stabs, lacerations, cuts, chopped, gunshots. In this case, there is a danger of direct infection of the wound tissue. Closed injury to the peripheral nerve is possible due to bruise, blow with a blunt object, compression of a limb, or excessive traction. Closed include damage to the nerve during dislocation and closed fracture, its compression by post-traumatic scars, hematoma, callus, etc.
In some cases, combined injuries occur, in which open injury to the nerve is combined with its closed damage. A special group consists of iatrogenic injuries of peripheral nerve trunks that occur as a complication of a number of surgical operations or various medical procedures.
Periods of injury
Acute period
takes 3 weeks from the moment of nerve injury. During this period, the spread of degenerative changes that occur in the nerve trunk after its injury occurs. Due to certain neurophysiological laws of this process, it is not possible to accurately assess the degree of dysfunction of the injured nerve in the acute period. During this period, surgical treatment is performed for open injuries with visualization of the anatomical break of the nerve while maintaining the integrity of the resulting segments. In such cases, it is possible to perform a primary suture of the nerve during PSO of the wound in the early stages after injury or to apply a primary delayed suture 2-4 days later.
Early period
lasts from 3 weeks to 3 months after damage and is characterized by the highest regenerative activity of damaged nerve tissue. In the early period, the degree, type, level and extent of damage can be accurately determined; together with a neurosurgeon, resolve the issue of treatment tactics (conservative or surgical) and determine the optimal extent of the operation.
Subacute or intermediate period
- 3-6 months from injury. There is a significant decrease in the rate of regenerative processes and an increase in the degree of divergence (diastasis) of the ends formed as a result of the anatomical break of the nerve. Surgical treatment is possible, but requires the use of complex reconstructive techniques and brings less results.
Late period
- from 6 months to 3-5 years after the nerve injury occurred. Due to a significant decrease in the ability to repair and an increase in degenerative changes in the injured nerve trunk, surgical treatment during this period leads to significantly less functional recovery.
Residual or long-term period
- 3-5 years after damage. Functional restoration of the nerve is not possible. To improve the function of the affected limb, orthopedic musculotendinous surgery may be performed.
Decrement test
Examination and analysis of the condition of most large nerves of the extremities usually does not cause difficulties. Assessing the condition of the plexuses and nerve roots is more complex, because, as discussed above, they are formed from many peripheral nerves, and it becomes necessary to examine almost each of them.
To diagnose diseases of the neuromuscular synapse, the method of rhythmic stimulation or “ decrement test ” is used. When performing a decrement test, the nerve is stimulated several times (usually five) at a high frequency of stimuli (about 1 per second), the muscle is forced to contract five times in a row in five seconds. If the synapse functions normally, then all five times the impulse from the nerve causes the muscle to contract with the same force. If the synapse is damaged, the muscle contracts weaker each time. Of course, this is a very simplified explanation of the essence of rhythmic stimulation ( decrement test ).
1.What is peripheral neuropathy and its types
Peripheral neuropathy is a condition that damages the nerves that carry signals to the brain and spinal cord from the rest of the body.
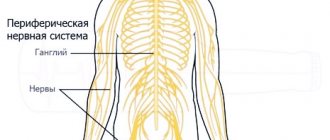
Peripheral nerves form a complex network that connects the brain and spinal cord to muscles, skin and internal organs. Peripheral nerves emerge from the spinal cord and are located along conventional lines in the body called dermatomes
. Typically, nerve damage affects one or more dermatomes and, as a result, specific areas of the body. Nerve damage and disruption of communication between the brain and other parts of the body impair muscle movement, interfere with normal sensation in the arms and legs, and cause pain. Peripheral neuropathies most often appear in people over 55 years of age.
Types of peripheral neuropathy
There are several types of peripheral neuropathy that appear for different reasons
.
The condition can range from carpal tunnel syndrome
(a traumatic injury due to constant use of the hands and wrists, such as while working on a computer) to nerve damage due to diabetes.
Neuropathies are generally classified according to the problem they cause (such as facial neuropathy) or what causes the disease.
A must read! Help with treatment and hospitalization!
Polyneuropathy (PNP)
Polyneuropathy (PN) (patient information) Polyneuropathy is one of the most common diseases of the peripheral nervous system.
What is polyneuropathy? Polyneuropathies are a group of diseases characterized by multiple and diffuse damage to roots, plexuses and peripheral nerves.
What symptoms bother a patient with polyneuropathy? Depending on which nerve fibers are more involved in the pathological process, the following complaints arise:
- sensitive symptoms: the patient is bothered by numbness, tingling, burning, “crawling” in the hands and/or feet; unsteadiness when walking, aggravated in the dark and when closing the eyes;
- motor symptoms: clumsiness, weakness in the hands and/or feet develops; weight loss in the muscles of the arms and legs; impaired fine motor skills (difficulty fastening buttons and zippers, tying shoelaces, etc.); difficulty walking (“spanking” feet, difficulty getting up and down stairs, etc.);
- vegetative symptoms: fluctuations in blood pressure, “interruptions” in the heart, constipation or diarrhea, dry skin or increased sweating, decreased libido, erectile dysfunction.
With polyneuropathy, either an isolated lesion of a certain type of nerve fiber or a combination of them can occur, which leads to the appearance of a varied clinical picture.
How does polyneuropathy develop? According to the speed of development, they are distinguished:
- acute polyneuropathies (development < 4 weeks): the most common cause is Guillain-Barré syndrome;
- subacute polyneuropathy (development within 4-8 weeks);
- chronic polyneuropathies (development over > 8 weeks): common causes are diabetes mellitus, alcohol abuse, lack of B vitamins, chronic inflammatory demyelinating polyneuropathy, hereditary causes, etc.
What are the causes of the development of polyneuropathy? The most common causes of polyneuropathy in developed countries are diabetes and alcohol abuse. Other possible reasons may be:
- dieting, poor nutrition, vegetarianism, leading to the development of vitamin B12 deficiency;
- chemotherapy, the use of neurotoxic drugs, less often - intoxication with heavy metals, etc.;
- autoimmune damage to peripheral nerves with the development of dysimmune neuropathies (Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy, paraproteinemic polyneuropathy, multifocal motor neuropathy, etc.);
- chronic somatic diseases: systemic autoimmune connective tissue diseases (systemic lupus erythematosus, rheumatoid arthritis, Sjogren's disease, etc.), chronic renal or liver failure, thyroid pathology, etc.;
- infectious diseases (Lyme borreliosis, HIV infection, neurosyphilis);
- oncological diseases with the development of paraneoplastic process;
- hereditary neuropathies (hereditary motor-sensory neuropathies, hereditary neuropathy with a tendency to paralysis from compression, transthyretin familial amyloid polyneuropathy, porphyritic polyneuropathy, etc.).
It is important to clarify the cause of polyneuropathy as early as possible, because The prognosis and treatment tactics depend on this!!!
What diagnostic methods can be used to detect polyneuropathy? An examination of a patient with polyneuropathy begins with a consultation with a neurologist, during which the doctor analyzes complaints and anamnestic information and assesses the neurological status. If there are subjective and objective symptoms indicating the presence of polyneuropathy, the doctor prescribes an examination:
- Electroneuromyography (ENMG) is the main instrumental method for diagnosing diseases of peripheral nerves, which not only confirms the fact of nerve damage, but also determines the nature of their damage (demyelinating, axonal, with conduction blocks).
In complex diagnostic cases, the doctor may recommend ultrasound of peripheral nerves, MRI of the plexuses with contrast, diagnostic lumbar puncture, morphological examination of the nerve (biopsy).
What diagnostic methods can be used to clarify the cause of polyneuropathy? To clarify the reasons that caused widespread damage to peripheral nerves, a thorough examination is necessary:
- comprehensive laboratory blood test: minimum volume - detailed general and biochemical blood test, RW, anti-HIV, HBsAg and anti-HCV, level of vitamins B1, B6, B9, B12, homocysteine (if necessary, in each case individually, spectrum of laboratory examination is expanding)
- if hereditary neuropathy is suspected - molecular genetic analysis (search for mutations in the PMP22 gene, neuromuscular disease panel or full genomic sequencing), etc.;
- electrophoresis of serum and urine proteins with immunofixation + freelite;
- lumbar puncture with general analysis of cerebrospinal fluid;
- instrumental general somatic examination, including cancer screening (CT of the lungs, ultrasound of the mammary glands, mammography, ultrasound of the prostate and scrotum, endoscopy, colonoscopy, ultrasound of the abdominal and pelvic organs, PET-CT, etc.).
The examination plan is drawn up individually! It is important to remember that in every third case, after a thorough examination, it is not possible to clarify the cause of polyneuropathy - in this case, idiopathic polyneuropathy is diagnosed!!!
What treatment methods have been developed for polyneuropathy? From the standpoint of evidence-based medicine, pathogenetic treatment has not been developed for all polyneuropathies. Thus, with diabetic polyneuropathy, first of all, careful monitoring of blood glucose levels and compliance with all recommendations of the treating endocrinologist is necessary. For toxic polyneuropathy, such as alcoholic polyneuropathy, treatment begins with complete cessation of the bad habit. If deficiency polyneuropathy is detected, vitamin therapy is carried out, and the causes causing the development of the disease are eliminated.
Pathogenetic therapy (i.e. therapy aimed at correcting the mechanisms of disease development) is the main one in the treatment of dysimmune polyneuropathy (Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy, paraproteinemic polyneuropathy, multifocal motor neuropathy, etc.). Depending on the type of dysimmune neuropathy, the optimal treatment method or their combination is selected individually, taking into account all the nuances of the disease. The following methods of pathogenetic therapy for dysimmune neuropathies have been developed: hormone therapy (use of high doses of glucocorticosteroid drugs), high-volume plasmapheresis, high-dose intravenous immunotherapy, as well as the use of cytostatics and monoclonal antibody preparations.
Currently, pathogenetic therapy has been developed for some hereditary polyneuropathies:
- Transthyretin familial amyloid polyneuropathy (TTR-FAP) – liver transplantation, stabilization of the transthyretin molecule;
- Fabry disease – enzyme replacement therapy;
- Porphyritic polyneuropathy - heme arginate.
- Refsum's disease - diet therapy, plasmapheresis.
Symptomatic therapy is used to eliminate unpleasant sensory sensations (numbness, burning, burning pain) in polyneuropathy. Local anesthetics, anticonvulsants, antidepressants, opioid analgesics, and psychotherapy are recommended.
Restorative and rehabilitation methods of treatment (transcutaneous electrical neurostimulation, acupuncture, biofeedback, interventional methods, massage, physiotherapy, balance therapy, robotic therapy) occupy an important place in the correction of neurological disorders in polyneuropathy.
If you have symptoms of polyneuropathy or have been diagnosed with polyneuropathy, you can undergo a comprehensive examination at the Center for Diseases of the Peripheral Nervous System of the Federal State Budgetary Institution National Center of Neurology, where they will help you clarify the diagnosis, identify the causes of damage to the peripheral nerves and prescribe therapy based on evidence-based medicine.
This area has long been one of the priorities for the Federal State Budgetary Institution Scientific Center for Science and Technology. Here, the country's first neuroreanimation department was created, which was famous for its unique methodology of caring for patients with severe forms of polyneuropathy requiring long-term artificial ventilation. Several decades ago, unique work was carried out on the diagnosis and treatment of certain forms of neuropathies: hereditary, diphtheria, dysimmune, etc. Here, for the first time in the USSR, plasmapheresis was introduced as a method of treating autoimmune diseases of the nervous system. We have accumulated unique domestic experience in the treatment and rehabilitation of patients with Guillain-Barre syndrome, severe forms of CIDP and neuropathies of other origins. The center for diseases of the peripheral nervous system includes 13 specialists, including 10 neurologists and 3 endocrinologists. All neurologists are proficient in ENMG research techniques.
Employees of the Center for Peripheral Nervous System Diseases provide consultations to patients on an outpatient basis within the framework of compulsory medical insurance and on a commercial basis.
MAKE AN APPOINTMENT AND ENMG/iEMG BY MULTI-CHANNEL PHONE +7 +7