You can familiarize yourself with other diseases starting with the letter “V”: Vegetative state, Ventricular, Vestibular ataxia, Vestibular neuronitis, Vibration disease, Viral meningitis, Viral encephalitis, Temporal lobe epilepsy, Intracerebral hematoma, Intracranial tumors of the cerebral hemispheres, Intracranial hypertension, Inflammatory myopathy, Inflammatory polyneuropathy, Congenital myopathy, Congenital paramyotonia, Secondary parkinsonism
Why is a vegetative state dangerous?
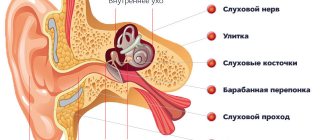
In vegetative states, the functions of the hypothalamus and brain stem are preserved, but the cerebral hemispheres suffer from severe dysfunction. This leads to impaired consciousness and the absence of the possibility of spontaneous mental activity. There are no signs of awareness, but the presence of unconditioned reflexes is noted. Vegetative states are characterized by periods of wakefulness accompanied by the opening and closing of the eyes. The disorder can be diagnosed clinically, but additional hardware diagnostic methods are prescribed, such as:
MRI;- Brain evoked potential study;
- Checking internal hemodynamics;
- EEG;
- PAT
As therapy, activities are carried out to stimulate the functioning of the hemispheres. In addition, the organization of high-quality patient care is required; nutrition, feeding, prevention of bedsores and possible complications.
General information about pathology
To vegetate means to live with the preservation of all biological functions, except intellectual and social. The term was introduced in 1972. In vegetative states, a personality disorder occurs, which results in disintegration of subcortical structures and the cerebral cortex. Special standardized scales have been developed that allow the degree of disorder to be determined using characteristic clinical signs. This is done by specialists such as resuscitators, rehabilitation specialists and neurologists. Accurate instruments to assess consciousness have not yet been developed. It has not even been established to what extent the impossibility of reacting to external stimuli reflects their perception or non-perception at the level of consciousness. It is not known whether a vegetative is able to understand the speech of others, their touch, and whether any internal processes occur in his consciousness.
Causes
Cerebral dysfunction begins due to factors damaging the brain, which are the causes of the syndrome. Etiological factors are classified according to their mechanism of action:
Metabolic, causing acute intoxication and hypoxia. These may include the use of drugs, an overdose of which causes toxic damage to brain cells. In addition, such damage to cerebral structures can provoke acute dysmetabolic conditions, which include hepatic coma, uremia, hypo- and hyperglycemia caused by diabetes, as well as poisoning with neurotropic poisons;- Severe TBI, diffuse axonal damage, and brain contusions are considered mechanical factors. In fifty percent of cases, they cause a coma that turns into a vegetative state;
- Intracranial hemorrhages, brain tumors, meningitis, encephalitis and other infectious lesions are organic causes caused by changes in cerebral tissue.
Etiology and causes of the condition
A vegetative state in a person develops due to damage to the cerebral hemispheres, which can develop due to injury, infection, or be toxic in nature, develop after ischemia.
If the root cause of the vegetative state is ischemia - cardiac arrest or stroke and oxygen does not reach the brain for more than 6 minutes, then the most irreversible changes take place, ultimately leading to a pathological condition.
According to medical statistics, in 30% of patients diagnosed with a vegetative state, it is caused precisely by ischemia, in 6 out of 10 such patients, doctors record a death, and only 4% of victims are able to return to normal life.
The root causes of the development of a vegetative state may be the following:
- head trauma suffered by the patient;
- acute form of cerebral blood flow disorder - stroke;
- severe form of intoxication, poisoning with chemical or organic compounds;
- anesthesia, during surgery and the use of general anesthesia;
- infections affecting the brain, such as encephalitis;
- brain damage due to disruption of blood flow and oxygen starvation.
Mechanism of development of the vegetative state
Under the influence of damaging factors, connections between the subcortical centers and the reticular formation are broken, which causes coma. When lost connections are restored, the functioning of the remaining synapses is strengthened, new interneuronal contacts are formed and neurotransmitters are reactivated, the coma is exited, which is characterized by an “awakening reaction,” that is, the patient opens his eyes. After this, a gradual restoration of consciousness begins. If recovery remains in the awakening phase, VS occurs. Experts suggest that it occurs during pathological processes of reintegration.
Characteristic signs of a vegetative state are extensive damage to the subcortical substance and diffuse necrotic changes in the thalamus and cortex. Atrophy of demyelination of subcortical structures also occurs, but much less frequently. According to some experts, the leading role in the mechanism of development of VS belongs to the activation of the process of removal of defective cells by the body.
Autonomic dysfunction syndrome in children: myths and reality
Autonomic dysfunction syndrome (AVS) and its manifestations in children still raise a large number of questions, to which there are just as many answers, and not always unambiguous. Suffice it to say that in Internet search engines alone there are 214,000 Russian-language sites dedicated to SVD, and 10,600,000 English-language sites covering issues of disorders of the autonomic nervous system. Let us add that if for 1951–1960. There were only 68 publications, then in 2001–2008 one can find 10,623 publications on autonomic dysfunction (Fig. 1).
The abundance of information on this topic does not exclude the existence of certain myths both among patients and among medical practitioners. In this publication, the authors attempted to determine the essence of SVD in children and dispel the most common myths regarding this problem.
Myth one: SVD is not an independent nosological entity. However, according to the International Classification of Diseases (10th revision) in the class “Diseases of the nervous system”, in the block “Other disorders of the nervous system” under code G90.8 there is a definition of “Other disorders of the autonomic (autonomic) nervous system,” which means SVD.
Myth two: SVD is an acquisition of the 20th century. In fact, the study of functional pathology, manifested by cardiac disorders, dates back to the 19th century, when in 1871 Da Costa Jacob Mendez (1833–1900), an American physician, described the “excitable heart” of young soldiers participating in the Civil War in USA, called Da Costa syndrome. In our country, the foundations for the study of the physiology and clinic of the autonomic nervous system were laid by such outstanding scientists as S. P. Botkin, I. M. Sechenov, I. P. Pavlov, L. A. Orbeli, A. P. Speransky, K. M. Bykov. At the beginning of the twentieth century (1916), the Russian scientist V.F. Zelensky in “Clinical Lectures” described the symptoms of cardiac neurosis. Modern ideas about the organization of the autonomic nervous system, as well as clinical vegetology, we, indeed, largely owe to scientists who worked in the twentieth century. The attending physician of the 21st century, having encountered the problems of autonomic dysfunctions, cannot do without the works of A. M. Vein and N. A. Belokon, in which one can find explanations for almost all clinical cases.
Myth three: the basis of autonomic dysfunction is the increased activity of one department due to the suppression of another. This idea - the “principle of scales” - reflects the rule of double innervation, in which the sympathetic and parasympathetic systems have opposite effects on the working organ (dilation and constriction of blood vessels, increased and slowed heart rate, changes in the lumen of the bronchi, peristalsis and secretion by the organs of the gastrointestinal tract) . However, under physiological conditions, an increase in the effects of one of the departments of the autonomic nervous system leads to compensatory tension in the regulatory mechanisms of another, which transfers the system to a new level of functioning, restoring the corresponding homeostatic parameters. The most important role in these processes is played by both suprasegmental formations and segmental autonomic reflexes. In a state of overstrain, failure of adaptation, the regulatory function is disrupted and, accordingly, increased activity of one department does not lead to corresponding changes in the other, which is clinically manifested by symptoms of autonomic dysfunction.
Myth four: stress plays a leading role in the etiology of autonomic dysfunctions. In fact, SVD is polyetiological, and among the many causes, both congenital and acquired features can be distinguished:
- hereditary and constitutional features of the activity of the autonomic nervous system (autosomal dominant type of inheritance);
- unfavorable course of pregnancy and childbirth, contributing to impaired maturation of cellular structures of the suprasegmental apparatus, natal injuries of the central nervous system and cervical spine (hypertensive-hydrocephalic syndrome, vertebrobasilar insufficiency);
- psycho-emotional characteristics of the child’s personality: increased personal anxiety, depressive disorders, hypochondriacal fixation on the state of one’s own health;
- psycho-emotional stress (pathological intra-family relationships, incorrect educational tactics, including overprotection, conflict situations in the school environment, staying in deviant informal groups);
- postnatal damage to the central nervous system (skull injuries, tumors, infections);
- mental and physical fatigue (classes in specialized schools, sports clubs with participation in competitions);
- hypokinesia (a sedentary lifestyle leading to a sharp decrease in tolerance to dynamic loads);
- hormonal imbalance (pre- and puberty, congenital and acquired diseases of the endocrine glands);
- acute and chronic infectious and somatic diseases, foci of infection (tonsillitis, dental caries, sinusitis);
- pathological influence of tobacco combustion products, beer alcoholization, toxic and drug addiction, leading to destabilization of the autonomic nervous system due to toxic and psychoneurotic effects;
- other reasons for the development of autonomic dysfunctions: cervical osteochondrosis, surgical interventions and anesthesia, unfavorable meteorological conditions, excess body weight, passion for watching TV shows, computer games.
Myth five: clinically, SVD manifests itself primarily as damage to the cardiovascular system. Indeed, cardiovascular manifestations (“dystonia”) are present in various types of autonomic dysfunction. However, in the diagnosis one should remember and take into account other numerous clinical manifestations of this pathology: the condition of the skin, violations of thermoregulation, cephalalgia, changes in the respiratory system up to the hyperventilation phenomenon (pseudo-asthmatic attack), symptoms of dysfunction of the gastrointestinal tract, both dyspeptic and painful in nature , urinary disorders.
For a practicing physician, clinical manifestations such as vegetative paroxysms (“panic attacks”, “vegetative crisis”) are quite difficult in terms of diagnosis, the criteria of which are: paroxysmalness, multisystem vegetative symptoms, emotional-affective disorders. In childhood, there is a predominance in the structure of an attack of vegetative-somatic manifestations over actual panic, emotional experiences, while as the child grows up, the vagal direction of reactions decreases, the sympathetic component in paroxysms increases, reflecting the general intensification of the humoral link of regulation. An insufficiently studied problem in pediatric vegetology, with particular significance and high prevalence (from 15 to 50% of children and adolescents, according to I.V. Leontyeva, had a history of at least one fainting spell), remains syncope: vasovagal, situational, stress and orthostatic, the pathological mechanisms of which include vegetative components.
Myth six: clinical manifestations of autonomic dysfunction are characteristic exclusively of adolescence. Autonomic dysfunction is one of the most common diseases among adolescents; its frequency in the population of boys, according to various authors, ranges from 54.6% to 72.6%, and among girls from 62.4% to 78.2%. The state of morbidity can be indirectly judged by the number of publications on this problem among children of different ages: the number of articles on manifestations of VDS in adolescence is more than 7 times higher than the number of publications on the clinical features of the syndrome in newborns (Fig. 2).
This may be due to the difficulties of objective diagnosis of autonomic dysfunction in neonatology. However, an attentive clinician can already identify symptoms of autonomic disorders during the newborn period: “marbling” of the skin, cyanosis of the nasolabial triangle or limbs, disturbances in thermoregulation, regurgitation, vomiting, “intestinal colic,” disturbances in heart rhythm or repolarization processes on the ECG.
Autonomic changes worsen by the age of 4–7 years, and, as a rule, the parasympathetic direction predominates, accompanied by fearfulness, indecisive behavior, and increased body weight. Finally, at puberty, the manifestations of autonomic dysfunction are accompanied by violent emotional manifestations and personality disorders, which leads to more frequent requests for medical help and, accordingly, to more frequent registration of the disease.
Myth seven: it is impossible for a practitioner to objectively assess the state of the autonomic nervous system. Indeed, the diagnosis of SVD is largely subjective and depends on the clinical worldview and experience of the doctor, since it is mainly based on clinical symptoms (assessment of vegetative status using tables and questionnaires by A. M. Vein, modified for children by N. A. Belokon, 1987). Currently, in pediatrics, to characterize autonomic tone, mathematical models for assessing autonomic indicators are used: the Kerdo index, analysis of heart rate variability with the calculation of statistical indicators (tension index according to R. M. Baevsky). According to the standards developed at a joint meeting of the European and North American Heart Associations in 1996, for clinical studies, heart rate variability is recommended to be assessed using four main indicators:
- SDNN (standard deviation of the NN interval) - standard deviation of the duration of normal RRs in a 24-hour ECG recording;
- SDANN (standard deviation of the average NN interval) is an indicator of the stability of heart rate variability;
- HRV-index—triangular heart rate variability index;
- RMSSD (the square root of the mean squared differences of successive NN intervals) - is calculated as the square root of the sum of squared differences of successive pairs of RR intervals, including anomalous ones.
In recent years, the possibilities of mathematical assessment of heart rate variability have expanded through the use of spectral analysis with the identification of certain components: very low frequency (Very Low Frequency - VLF), reflecting the degree of activation of cerebral ergotropic systems, low frequency (Low Frequency), characteristic of sympathetic influences, and high frequency (High Frequency), with the help of which vagal influences are described.
Significantly expands the possibilities for an objective assessment of autonomic dysfunction by the use of stress tests, which make it possible to characterize autonomic reactivity and autonomic support of activity (physical - when using a test with dosed physical activity, position tests - orthostatic test, mental and emotional). To record vegetative changes, parameters of the cardiovascular and respiratory systems are used: heart rate, heart rate variability, blood pressure (BP), respiratory rate. The studied indicators are recorded at rest (vegetative tone) and during activity (vegetative support, which can be normal, excessive or insufficient and reflects the state of the ergotropic apparatus). The introduction of 24-hour blood pressure monitoring into pediatric practice and the assessment of the circadian rhythm of blood pressure made it possible to open a new page in the objectification of the assessment of the autonomic regulation of vascular tone.
Thus, the use of an integrated clinical and experimental approach using a functional-dynamic study of vegetative status, tone, autonomic reactivity and autonomic support of activity will allow the attending physician to identify changes in the homeostatic parameters of the body and assess the state of its adaptation mechanisms during autonomic dysfunction.
Myth eight: therapy for children and adolescents with VDS is ineffective. The success of treatment for children largely depends on the timeliness and adequacy of the therapy; it must be comprehensive, long-term, taking into account the age and clinical manifestations of the disease, with the active participation of the patient himself and his environment. Preference should be given to non-drug correction methods in combination with general regimen and psychotherapeutic measures, while drug treatment should include a minimum number of individually selected drugs.
Non-drug methods:
- normalization of work and rest regimes, with mandatory physical activity, physical education, limiting the time spent watching TV shows and spending time at the computer, it is possible to engage in certain sports (playing, dynamic, tourism), but without participating in competitions, reducing the negative impact of psycho-emotional stress, normalizing sleep ;
- adherence to certain dietary measures depending on the clinical manifestations of dysfunction;
- therapeutic massage of the spine, cervical-collar area, for hypotension: massage of the lower extremities, abdomen with a course of at least 15–20 procedures;
- reflexology;
- physiotherapeutic methods including electrosleep procedures in the complex (10–15 procedures per course of treatment daily or every other day);
- hydrotherapy (baths, showers, rubbing, dousing);
- psychotherapy.
Drug therapy:
- sedatives, primarily of plant origin (Persen);
- plant adaptogens (tinctures of Schisandra, Eleutherococcus, Leuzea, Aralia);
- vitamin therapy, microelements (magnesium);
- metabolic, nootropic drugs that allow not only to stop the pronounced clinical manifestations of SVD, but also to improve the long-term prognosis by optimizing metabolic processes in suprasegmental structures: Pantogam (hopantenic acid) 0.25 g 2-3 times a day - course 1 month, Nootropil ( piracetam) 0.4 g 2-3 times a day - course 1 month, Phenibut (gamma-amino-beta-phenylbutyric acid hydrochloride) 0.25 g 2-3 times a day - course 1 month;
- agents that improve microcirculation: Stugeron (cinnarizine) 25 mg 3 times a day - course 1 month, Cavinton (vinpocetine) 2.5-5 mg 3 times a day - course 1 month, Trental (pentoxifylline) 5-10 mg/kg per day - course 1 month;
- tranquilizers, antidepressants and antipsychotics in children are used taking into account age, in minimal doses and only if there is no effect from other treatment methods.
Myth number nine: ADD is easier to prevent than to treat. In fact, preventive measures to prevent autonomic dysfunction should be carried out before the birth of the child both by the pregnant woman herself (normalization of the daily routine, avoidance of overwork, weight control with nutritional correction if necessary, optimization of the psycho-emotional environment), and by medical personnel providing patronage and management of pregnant women. childbirth
Important conditions for the prevention of SVD in children and adolescents are age-appropriate education and ensuring harmonious mental and physical development. Both overloading a child, especially with sedentary activities, such as music, and overprotection with encouragement of inactivity are unacceptable. For people of any age, one of the most significant ways to prevent SVD is physical education, in contrast to sports, which should not be allowed for all children, even those over 14 years of age. In all age groups, sports should be provided with high-quality and informal medical supervision. It is important to promote a healthy lifestyle, excluding, in particular, smoking and other bad habits. In general, the problem of preventing SVD goes beyond just medical measures; its solution is associated with the possibility of major social and environmental transformations, increasing well-being and improving living conditions of the population. The authors do not claim to be the “ultimate truth”, since as long as humanity exists, the problem of SVD will worry us and approaches to diagnosis and treatment will change.
For questions regarding literature, please contact the editor.
M. Ya. Ledyaev , Doctor of Medical Sciences, Professor O. V. Stepanova , Candidate of Medical Sciences, Associate Professor N. V. Shakhova * Volgograd State Medical University, * Children's Clinical Hospital No. 8 , Volgograd
Symptomatic picture
In a vegetative state the following is observed:
Preservation of vital functions: breathing, cardiovascular activity, digestion, chewing and swallowing reflex of tear production;- The ability to involuntarily move the eyes, blink, exhibit unfocused motor activity, grind teeth, grasp objects located near the hand, and respond to pain impulses is preserved;
- There are no signs of awareness of what is happening, no contact with the outside world;
- There are periods of wakefulness when a person lies with his eyes open. He is able to move his eyeballs slowly, but this is not a conscious gaze. When there are flashes of light and loud sounds, the patient reacts;
- In the absence of speech, the ability to produce isolated guttural sounds and deep sighs is retained, which can give untrained people the erroneous impression that they are emerging from a vegetative state. But that's not true. The first signs of exiting the VS are gaze tracking, gaze fixation, a state of small consciousness in which the patient can fulfill simple requests: clench his fingers, show his tongue.
The duration of a vegetative state can range from several months to 10 years. Persistent VS is diagnosed when symptoms persist for more than a month. Permanent is characterized by the persistence of symptoms for more than a year in a post-traumatic vegetative state and more than three months in a non-traumatic genesis.
Clinical picture
It is worth noting that in a vegetative state one can observe its own characteristics. Based on the characteristic signs, it will be possible to recognize the pathology and understand what exactly is happening to the patient’s body. For information, people should consider the clinical picture of the condition.
A vegetative state has the following symptoms:
- The person is completely unconscious. He doesn't understand who he is. He also does not recognize anyone from his surroundings.
- The biorhythms of wakefulness and sleep are preserved. There is a biological distinction between these conditions. The eyes have the ability to open on their own, and this can also be a reaction to an irritant.
- There are no voluntary and conscious movements. Only reflex actions remain, as well as physical and motor movements. For example, twitching of the arms or legs, head, or uncontrolled movement of the lips may be observed.
- In humans, cardiorespiratory function is observed.
- The patient cannot control natural processes. That is, there is urinary and fecal incontinence.
- A person has no reaction to stimulants, both visual, auditory and tactile. That is, he cannot respond to a request, as well as to a command. The patient does not have the ability to connect words and pronounce them clearly.
The duration of the vegetative state can be several months or ten years. In this case, two forms of pathology can be distinguished. There may be a persistent vegetative state that lasts less than 1 month. In such a situation, one can hope that consciousness will be partially or completely restored.
A permanent condition may also occur. It continues for more than a month. In such a situation, there is an extremely small chance that the body will at least partially recover.
Doctors believe that the persistent condition will become permanent 3 months after brain damage associated with acute disruption of blood flow, as well as poisoning. In case of traumatic brain injury, the transition between forms occurs within 12 months.
In any case, the patient will be monitored by a doctor, because it is important to carefully monitor the person’s well-being. It is definitely difficult to make a forecast immediately after the occurrence of such a condition. That is why you will have to wait a certain period, during which there is a high chance of recovery.
Diagnostic methods
The diagnosis is made by a neurologist based on characteristic signs: lack of awareness, preservation of unconditioned reflexes, sleep-wake phases. To assess the metabolism of bioelectrical activity of the central nervous system and cerebral hemodynamics, hardware diagnostic methods are required:
The study of evoked potentials can demonstrate anatomical interruption of cerebral tracts. It is worth considering that the resulting picture will be heterogeneous;- Electroencephalography is capable of recording paroxysmal bursts, delta and theta rhythms, and occasionally an alpha rhythm close to normal may appear;
- Ultrasound scanning of intracranial vessels helps to clarify the state of vascular blood flow. With VS, there is difficulty in perfusion and impaired venous outflow;
- Magnetic resonance imaging shows nonspecific changes in soft tissues: an increase in the volume of the ventricles and subarachnoid space, signs of atrophy. With a high degree of probability, the degree of atrophy makes it possible to make an expected prognosis about exit from the VS;
- PET allows you to detect the degree of decrease in metabolic processes in the cortex. In persistent vegetative states it decreases by 50%, and in permanent ones by 30-40 percent. During activation of the multifunctional area of the associative cortex, the exit from the VS begins.
To differentiate VS from coma, it is necessary to check the integrity of unconditioned reflexes, the change in sleep-wake phases and the presence of eye opening under light and sound influences. In coma, these signs are absent.
Therapy
Recent research has refuted the assertion that adult nerve cells are not capable of self-healing. To achieve this, the body has a mechanism for transforming stem cells and cerebral progenitor cells into neurons. The processes of surviving nerve cells grow and reserve areas of the brain are used. Treatment of vegetative-vascular conditions includes activation of the listed compensatory processes. It must be accompanied by the prevention of complications and quality care. Therapy includes:
Artificial nutrition that can fully provide the body with the necessary amount of microelements, vitamins, calories and proteins. Since tube feeding causes complications in the form of mucosal ulcers, gastroesophageal reflux, and aspiration, preference should be given to nutrition using a gastrostomy tube;- Pharmacological therapy and regular sensory stimulation designed to stimulate the restoration of consciousness. For this purpose, auditory, visual, painful, tactile, and olfactory stimuli are used with a gradual increase in intensity and time of exposure. This allows you to eliminate sensory hunger that prevents you from leaving the sun. In addition, recently a positive effect has been recorded from taking amphetamines. The search for a successful method of activating cerebral reintegration continues; in Japan and France, targeted electrical stimulation of the brain stem is now being tested;
- High-quality care, including maintaining adequate skin moisture, posture control, teeth brushing, and regular linen changes.
In addition, it is very important to carry out prevention and treatment of complications, which includes:
- Correct installation of catheters;
- Timely change of diapers;
- Massage;
- Changing the patient's posture;
- Planting with the help of orthopedic systems, designed to prevent secondary infections;
- Correction of muscle tone with medications;
- Passive movements to combat contractures;
- Treatment of contractures using tenotomy.
With permanent VS, it is necessary first of all to prevent complications. In case of persistence, brain stimulation is indicated.
Prognosis for vegetative states
It is possible to make any predictions only based on the cause of occurrence, the duration of the coma and the period of VS, the age and general condition of the patient. If the condition was caused by non-traumatic etiological factors, then recovery will take about 3 months, and at least a year if the factors that caused the vegetative state were traumatic. Cases of improvement were noted at a later date. In younger patients, motor activity returns more quickly. In most of the reported cases, restoration of brain function to the previous level does not occur. The consequence of VS is severe disability. If a vegetative is in this state for more than six months, then with good care and medical supervision, the survival rate is ¼ of all cases.
Prognosis and prevention
The outcome of VS depends on the cause, the age of the patient, the duration of the previous coma and the period of vegetative consciousness. Recovery occurs within the first 3 months. non-traumatic VS, for a year from the date of diagnosis of post-traumatic VS. The literature indicates cases of improvement in a later period. Motor activity is better restored in young patients. The functioning of the cortex does not return to its previous level; in most cases, severe disability is observed. If the duration of VS is > 6 months. Five-year survival rate is observed in a quarter of vegetatives. As a rule, these are cases of well-organized care and supervision. Prevention of VS includes the prevention of head injury, vascular accidents, exogenous intoxications, neuroinfections, and timely correction of metabolic disorders.
LiveJournal