Conversion disorder - symptoms
Some of the symptoms of conversion disorder typically include:
- weakness
- paralysis of arms or legs
- loss of balance
- seizures, sometimes with limited consciousness
- episodes of unresponsiveness
- difficulty swallowing
- feeling of a lump in the throat
- shaking and tremor
- difficulty walking
- slurred speech or loss of ability to speak
- difficulty hearing or hearing loss
- double vision, blurred vision, or episodes of blindness
- numbness or loss of touch
Symptoms of conversion disorder vary from person to person and depend on the type of neurological disorder the person has.
Symptoms can be mild or severe, may stop or be continuous, and usually affect the body's ability to function properly.
Causes
Dissociative (conversion) disorders most often develop as a reaction to traumatic events that occurred in childhood or adulthood. These may include long-term domestic abuse, sexual or emotional abuse, military conflict, natural disaster, kidnapping, accident, or traumatic medical procedure. For victims, this “going beyond oneself” is a way to cope with the traumatic event, to observe it from the outside - as if the “bad thing” was happening to another person.
Dissociative disorders most often occur in childhood, during the formation of personality.
The International Classification of Diseases presents 10 types of dissociative (conversion) disorders: dissociative amnesia, dissociative fugue, dissociative stupor, trance and possession, dissociative movement disorders, dissociative convulsions, dissociative anesthesia (loss of sensory perception), mixed dissociative (conversion) disorders, other dissociative disorders.
Diagnostics
A doctor will diagnose conversion disorder using criteria that include:
- loss of movement control or sensory symptoms
- symptoms that occur after a traumatic or stressful event
- symptoms that have no underlying medical or physical cause
- symptoms that interrupt daily activities
Your doctor may suggest additional diagnostic tests to rule out other diseases.
Additional diagnostic methods:
- computed tomography (CT)
- radiography
- electroencephalograms (EEG), which record brain activity and can rule out neurological causes of seizures
- blood pressure measurement and reflex tests
Once diagnosed, there are many treatment options for conversion disorder.
Classification of neurotic disorders.
In the 9th revision of the International Classification of Diseases (ICD-9) of the World Health Organization, neuroses under diagnostic code 300 are classified as anxiety neurosis (ICD-9: 300.0), hysterical neurosis (ICD-9: 300.1), neurotic phobias (ICD-9: 300.2), obsessional neurosis (ICD-9: 300.3), neurotic depression (ICD-9: 300.4), neurasthenia (ICD-9: 300.5), neurotic depersonalization neurosis (ICD-9: 300.6) and hypochondriacal neurosis (ICD-9: 300.7). In ICD-10, neurotic disorders are given the entire number 4, under the letter F (F40-F48).
"Diagnostic and Statistical Manual of Mental Disorders".
(DSM III) of the American Psychiatric Association in its third edition (1980), although it retained the coding of neuroses specified in ICD-9, but introduced some significant points into the traditional division of neuroses. We are not talking so much about neuroses as about “neurotic disorders”, which are divided into five groups called “somatoform disorders”, “dissociative disorders”, “fear syndrome”, “affective disorders” and “psychosexual disorders”. This classification presents the possibility of further differentiation from the classical concept of hysteria of the so-called hysterical phenomena of somatoform or even dissociative disorders. On this basis, oriented towards DSM III, we propose our own definitions of neuroses, especially the concept of “somatoform disorders”, which has not previously been used in the German linguistic space.
Somatoform disorders.
A distinctive feature of this group is the somatic symptoms specified in the DSM III definition, which, despite the apparent damage to organs and systems of the body, do not have any known pathophysiological mechanisms, while the design of these disorders is supposed to be related to mental factors and conflicts. In addition to hypochondria, these disorders are clothed in somatic symptoms, which are covered by the diagnostic names “hysterical neurosis” or conversion neurosis. DSM III proposes a division of the concept of “hysterical” somatic symptoms into three parts, namely: conversion syndrome, psychogenic pain syndrome and somatization syndrome.
Conversion syndrome.
The leading symptom is a loss or change in somatic function, which, after careful examination, cannot be explained by an organic lesion (disorder). The symptom is not subject to volitional control. The onset or manifestation is associated in time with conflict-specific irritation from the external environment (in the language of psychoanalysis - “trigger conflict situation”). Often a symptom impresses with its expressiveness and/or manifests itself as a result of the action of secondary causes of the disease. “Classic” conversion symptoms were previously regarded as neurological diseases - for example, difficulty swallowing (feeling of a lump in the throat), loss of voice (aphonia), deafness, double vision, blurred vision (blurred vision), blindness, fainting or unconsciousness (loss of consciousness), seizures or convulsions, difficulty walking, paralysis or muscle weakness, problems urinating or defecating. More rare are conversion symptoms related to the gastrointestinal or endocrine systems (eg, psychogenic vomiting, imagined pregnancy). The diagnosis of conversion syndrome is made when the presenting symptom does not correspond to the actual physical disorder, for example, an indicator of good motor function in paralysis of the limbs, normal pupillary response to light in conversion blindness, or paresis that is clearly inconsistent with the anatomy of the nervous system.
Frequency of manifestation, course, differential diagnosis.
Conversion syndrome corresponds to the definition of “classical” conversion neurosis with dramatic expressive symptoms and conspicuous symbolic content. Such classic pictures of the disease are becoming increasingly rare nowadays. The course is characterized by a sudden onset under the influence of emotional stressful conditions and a short duration. The danger of chronicity (and iatrogenicity) lies in the pathogenic psychosocial structure. Differential diagnosis consists of excluding organic disorders. The danger of misdiagnosis is especially pronounced in relation to persons with conspicuous “hysterical” character traits.
Psychogenic pain syndrome.
Severe and prolonged pain is the dominant harmful factor in the mind, reducing performance. Complaints of pain after a thorough examination do not correspond to the anatomy of the nervous system or pathological changes in organs and cannot be explained by known pathophysiological mechanisms. even if somatic disorders are present, complaints of pain cannot be explained by them. The onset or manifestation of pain in conversion syndrome is temporally dependent on the conflict-specific influence of the external environment, which causes this symptom in the absence of conscious comprehension of the conflict. Exacerbation of pain syndrome often occurs due to the action of secondary causes of neuroses in the absence of achieving benefits through other mechanisms.
Course, differential diagnosis, complications.
The pain syndrome can disappear when the triggering intrapsychic or social factors are canceled and, accordingly, become aggravated or become chronic with prolonged exposure. Patients have their own opinion regarding the psychogenesis of their pain and therefore insist on somatic therapy. A severe complication of this pathology is iatrogenic dependence on tranquilizers and drugs, as well as unsuccessful repeated surgical interventions.
Somatization syndrome.
The main feature of this syndrome is a variety of long-term recurrent somatic ailments that require medical attention, but do not have obvious somatic disorders. The disorders begin at the age of about 30 years and are chronic, although fluctuating, in nature. The disease picture is often inadequate (dramatic, severe, excessive) and includes a complex medical history that contains many medical diagnoses. Often these patients simultaneously benefit from the treatment recommendations of many doctors. The disorders are associated with pseudoneurological symptoms, gastrointestinal disorders (eg, abdominal pain), disorders in the female reproductive system (eg, menstrual disorders), pain (primarily in the back), cardiopulmonary and psychosexual symptoms. According to DSM III criteria, somatization syndrome is described in 12 symptoms and can be attributed to patients who, in connection with their complaints, took medication or changed their lifestyle.
Course, differential diagnosis, complications.
Chronic but fluctuating course with rare spontaneous remissions. The main complications are depression, suicide attempts, (iatrogenic) dependence on psychotropic drugs and unnecessary diagnostic interventions. Differential diagnosis should concern differentiation from all somatic diseases (for example, multiple sclerosis). The initial appearance of numerous somatic symptoms in late life is almost always explained by a somatic disease.
Hypochondria.
The leading symptom is a detailed activity associated with the fear of illness due to an unrealistic interpretation of somatic signals and sensations. Unrealistic fear is not influenced by either medical reassurance or appropriate diagnostic measures. Frequent visits to doctors are typical, and doctors are easily accused of dishonesty. Hypochondria can be a severe mental disturbance and affect various areas of the patient's life. The course is usually chronic, with the addition of some symptoms and the cessation of others. The differential diagnosis consists of limiting it from actual organic diseases and psychoses with a corresponding disturbance of perception.
Psycho- and sociodynamics of somatoform disorders.
Somatoform disorders are a manifestation of a subconscious conflict (or even a structural deficit) translated into body language (symbolized) or symptoms associated with fears about one’s own body and which are an adequate substitute for the actual mental conflict. With some functional somatic symptoms (for example, with conversion neurotic seizures or even psychogenic vomiting), symbolic expressiveness is in the foreground; other somatic symptoms (for example, chronic psychogenic pain) are less dramatic and have more relationships with neurotic conflict. The so-called substitution model often operates, in which the doctor, stating a complaint as a symptom (in this case, pain), actually regards it as a replacement, i.e. deviation from the response to the real situation (for example, someone who has suffered damage in interpersonal relationships, but denies the connection between the disease and this damage, while maintaining a passionate desire for support, recognition, reassurance, change, cheerfulness, etc.). These symptoms often stabilize and become compensated with the internal balance of the patient, as well as his partners and family members. The joint activity of all family members in helping this patient (Stierlin), the cessation of conflicts within the family prevents the exacerbation of the disease and stabilizes the condition even in conditions of unfavorable influence of the social environment. For clarity and precision in determining the sociodynamic aspect of somatoform disorders in somatization syndrome, which has been occurring for many years with a characteristic chaotic medical history, the doctor is of great importance. Modern forms of medical care (individual medical appointments, hospitals, medical clinics, etc.) serve the purpose of bringing out the intrapsychic conflict in the form of its stage embodiment, which is so important for the patient, when the patient dramatizes his secret mental suffering in a form previously unknown to him and in a way that “brings them to the surface.” Fundamentally, this manifests itself in the patient’s hope and understanding of his problems (understanding consists of asking the patient to verbalize what he previously asked the doctor about). The tragedy of this situation is that when a patient enters the medical scene, the entire apparatus of medical diagnostics is activated, which in each case is very painful and often unsuccessful. Sometimes it can be assumed that the patient’s somatic complaints and his visits to the doctor are caused by a masochistic desire to hurt himself and reveal a connection with the sadomasochistic complex. No one will suffer by choice, but one should always think about whether the condition is being reduced by something that might cause more suffering (eg fear, loneliness, deprivation of appropriate attention and reassurance, complete inhibition of expressing one's feelings , guilt). In a medical conversation, one should acknowledge the severity of the patient's suffering rather than deal with the aggravation of his symptoms. Once a symptom has been established, the question to ask is: what relief is the patient looking for in his suffering? What would happen to him without this symptom? Often, obtaining an answer to these questions is the basis for offering psychotherapeutic help (as well as refusing it). With hypochondria, it is always stated that it is less based on the description of a neurotic conflict, but rather, as it were, thematizes (denotes in an accessible topic) the general feeling of animal fear and, in accordance with this (as, probably, with somatization syndrome ), denotes in severe disorders of somatic well-being the existing preparedness in the form of a “mother-child” relationship. The patient's connection with his body, so to speak, symbolizes this early (broken, failed) connection with the mother: in his hypochondriacal fears and somatic focusing of attention, the patient finds a subconscious reflection of maternal care and care. Somatic functions do not have the corresponding labels such as “uncaring,” “unpredictable,” “unkempt,” “overly demanding,” or even “defective,” which the mother had previously found in the patient. Forced attention to one’s somatic functions (“care instead of love”) is a replacement for the maternal care for the child’s body that he felt in childhood. Hypochondriacal somatization disorders are almost always chronic, because in the narrow sense they are a conversion-neurotic manifestation of deeply rooted “early disorders” and cover up a massive “I”-structural deficit.
Therapy of somatoform disorders.
Maintenance therapy is indicated, in which the symptom is analyzed, first of all, in its subjective aspect (from the point of view of its place and meaning for a given subject). For some patients, long-term psychological (i.e., psychological and psychological-pedagogical, aimed at resocializing childhood psychotraumatization) support is necessary. The exception is conversion syndrome, in which targeted psychotherapy aimed at processing the conflict leads to the disappearance of the symptom in a short time. For conversion neurotic disorders, without prior announcement of the nature and orientation of psychotherapy, suggestive methods (for example, hypnosis) are most often recommended. Psychotherapy can be considered adequate for the treatment of somatoform disorders when the patient is willing to at least consider the psychogenesis of his somatic disorders. For all somatoform disorders, there is a danger of iatrogenic dependence on psychotropic drugs (as opposed to psychotherapy), as well as the futility of other unnecessary diagnostic and, especially (this should always be kept in mind!), surgical interventions.
Dissociative disorders.
Dissociative disorders, as well as somatoform disorders, belong to the hysterical circle (the most commonly used designations are “hysterical neurosis”, “dissociative type”). The leading symptom of dissociative disorders is a sudden, time-limited change in integrative mental functions - memory (psychogenic amnesia), self-identification (not one, but many personalities) or motor behavior - psychogenic escape (fugue). Differential diagnosis with neurological disorders (temporal lobe epilepsy), as well as with psychoses. Depersonalization syndrome in the DSM III taxonomy also refers to dissociative disorders. The leading symptom is a violation of self-perception and experience of one’s “I”, as a result of which the perception of one’s own existence is either lost or changed (alienation of one’s own feelings, a change in the perception of one’s own body, a feeling of oneself as mechanical, devoid of naturalness, as if “in a dream”). Mild depersonalization experiences occur in 30-70% of young people. The more pronounced this symptom is, the more severe the mental disorder in which it manifests itself (fear syndrome, depression, schizophrenia), which requires differential diagnosis!
Psycho- and sociodynamics, psychotherapy.
All described phenomena are protective mechanisms of dissociation and in traditional diagnostics were classified as hysteria. They are also found in borderline disorders (border areas between schizophrenic psychoses, personality disorders and mental health) and in schizoid or schizotypal personality disorders that go beyond hysterical disorders. A thorough structural or personality diagnosis is necessary to determine the location and significance of dissociative symptoms. The conclusions from this structural diagnosis also determine the starting points of psychotherapy. Diagnosed disorders often (but not always) express a self-structural deficit that in many cases limits the scope of psychotherapy. With appropriate strength of the “I” and motivation (in this case, even less often), integration of dissociated content or participation of the individual in achieving common therapeutic goals is possible.
Neurotically caused fear syndrome.
Fear syndrome includes disorders in which fear is the dominant symptom, occurring either when encountering a triggering, fear-causing object or situation (phobias), or when trying to overcome obsessive thoughts or obsessive actions (obsessive neurosis). The affect of fear can occur in the form of panic or generalized fear. The classification of obsessional neurosis as a fear syndrome and the distinction between a fear syndrome combined with panic attacks and a fear syndrome uncomplicated by panic attacks is specific to DSM III and has not yet been applied in the German language space.
Phobic disorders.
The leading symptom is a prolonged, unusually strong fear of certain objects or situations that normally do not cause such feelings, associated with repressed desires and accompanied by avoidance of fear-inducing stimuli. Fear and avoidance behavior limit social radius and create subjectivity and vulnerability. In simple phobias, restrictions are associated with phobic fears relating to single objects or situations (for example, fear of animals or fear of heights). Social phobias are characterized by a persistent, irrational fear of a situation in which others might see, test, shame, or humiliate. Severe social restrictions are often caused by agoraphobia.
Agoraphobia. The leading symptom of this severe form of phobia is a pronounced fear of being alone or of being in an open space from which evacuation is difficult or in which it is difficult to provide assistance in case of sudden weakness, such as fainting. Most often, the following avoidance situations arise: being in a crowd (busy street, store), in a tunnel, elevator (lift), on a bridge, in public transport. Patients can often leave the house only with an accompanying person. The disorder often begins with a single or several repeated attack of fear. Next, the fear of waiting for the attack itself develops, the so-called “fear of fear.” Often this means the onset of chronification with the inherent limitation of the disease's normal range of activity; Fear and avoidance behavior define the life of someone suffering from this disorder. As with other phobias, the severity of this disorder can increase or decrease depending on changes in the phobic stimuli. Complete remissions are also possible.
States of fear or “fear neurosis.”
Here the affect of fear is in the foreground. It may occur as generalized fear or panic. Generalized fear syndrome refers to a general, persistent (persistent) state of fear, which is a leading symptom and not only accompanies the clinical picture of other disorders. In addition to large individual differences in manifest symptoms, constant features are motor tension, autonomic hyperactivity, anxiety of anticipation, hypervigilance and constant checking of the environment. A panic attack manifests itself as a sudden onset of intense apprehension. Fear or fright is often accompanied by a feeling of impending catastrophe (misfortune). The most commonly recurring symptoms during a panic attack are: dyspnea, palpitations, chest pain, choking or tightness, dizziness, paresthesia, sweating, weakness, trembling or chills, fear of death, madness, or loss of self-control during the attack. Complications - especially with chronic fear syndrome (including agoraphobia) - almost always manifest themselves in the abuse of alcohol, barbiturates and anxiolytics (often in accordance with medical prescriptions). The course can be undulating, with spontaneous remissions, but more often with a pronounced tendency to chronicity. Generalized fear and panic attacks are associated with the mechanism of fear suppression through a tendency towards phobic processing with a corresponding change in symptoms, namely the removal of the affect of fear through avoidance behavior.
Psycho- and sociodynamics of neuroses of fear and phobias.
Neurotic fear syndromes are not conflict specific. Often the formalization of getting rid of fear symptoms or avoidance behavior involves protection from neurotic conflict. At the same time, conscious avoidance is often diametrically opposed to the subconscious instinctive impulse: agoraphobia, for example, is a defense against constant expansive desires (escape from the constant desire for violence, hatred and urges to kill, sexual desires, fantasies associated with prostitution, etc.) . These desires are based on biographical life experience (often on the prohibition of the child’s autonomous behavior in early childhood), suppressed by fear and subconscious, and therefore rationalized and protected avoidance behavior (avoidance of temptation). In all phobic situations, a basic protective process operates, according to which the escape from threatening internal stimuli is transferred to the external situation, as a result of which a corresponding avoidance and reduction of fear occurs. Repeated experience of fear reduction leads to stabilization of the avoidance response in accordance with the principles of learning theory. In fear neurosis, the expressive experience of a panic attack often corresponds to a psychodynamic origin: an attack of fear can be the equivalent of an attack of rage, an ersatz of the sexual act (with a typical increase and end of sexual arousal); often, however, this is an expression of the elementary fear of rejection, corresponding to the fear of death when a mother leaves a helpless child. We often find patients with fear neurosis among the children of those overly anxious mothers who convey to their children their diffuse fear of life instead of a realistic assessment of the risks and dangers threatening the child. Koenig calls this "loss of control of the object" as one of the vital internal structures. In such cases, a formed person remains dependent on an outsider who plays the role of vital protection. Increased sensitivity to rejection, an emphasized desire for avoidance and passive anticipation of errors in therapy characterize relationships with patients suffering from fear neurosis. During psychotherapy, a departure from the achieved improvement is possible due to the activation of a deeply rooted fear of autonomy. Conversely, fear is often eliminated by the proximity of a protective figure (doctor) or protective situation (hospital).
Therapy.
Behavioral therapy for tolerable phobic symptoms or even massive social impairment, focused on protecting the patient; soft, caring, analytical psychotherapy aimed at identifying causes (the prognosis is unfavorable if the disease is expressed exclusively in symptoms, simultaneously supported by a high degree of secondary causation). Often the treatment of choice is long-term, leisurely therapy in which the therapist acts as the missing protective figure (symbolized often through a prescription, written behavior statement, telephone number, or medication that the patient must carry with him). Regular use of anxiolytics is contraindicated both due to the risk of addiction and secondary fear of drug withdrawal.
Obsession syndrome or obsessional neurosis.
The leading symptom is recurrent obsessive thoughts and/or obsessive actions. Obsessive thoughts invade consciousness and are perceived by the sufferer as alien, disturbing and meaningless (in contrast to delusional ideas, which are experienced as syntonic to the “I”), which is why an attempt is made to ignore or overcome them. Obsessive actions are also accompanied by a feeling of subjective violence, i.e. the patient does not have a clear ability to choose between conscious and uncontrolled action. The course of action is regulated by certain rules or rituals, which, while not meaningless in themselves, are designed to cause or prevent certain events and situations. Suppressing compulsive actions causes massive fear. Intrusive thoughts may take the form of violent thoughts (“I want to kill my baby”), fears of contamination (“I could become infected myself or infect others through touch”), or doubts about everything (for example, wondering for a long time about whether an accident will occur). on transport). The most common types of obsessive actions include hand washing, counting, constantly double-checking one's actions, and the desire to touch. Often the immediate social environment is involved in a ritual of obsessions (checking cleanliness, being involved in a situation of elimination and control, etc.). The course and complications are the same as with other fear syndromes. Obsession syndrome can become the main content of life. If obsessions lead to serious social restrictions, then they are called not a neurosis, but a “disease of obsessions.”
Psycho- and sociodynamics of obsessional neurosis.
Obsessive thoughts and actions have a function associated with fear. They make safe threatening instinctive impulses (urges) of a predominantly aggressive or sexual nature, which can lead to pronounced antisocial tendencies. Intrusive symptoms are often relatively explicit about their defensive content; In addition, this defense is also associated with the fact that obsessive symptoms are alienated from the patient’s personality. The obsessive syndrome is often combined with magical thinking and magical behavior, with the help of which instinctive danger is suppressed. When the syndrome of obsessions (but not violence) is combined with a corresponding obsessive or “passive-aggressive” character, the patient’s behavior in a therapeutic relationship also bears the corresponding characterological features (intransigence, inability to empathize, intractability, sublimated tendency to obstruction, resistance, passive aggression), which the psychotherapist defines as sadomasochistic reactions of resistance. In therapeutic practice, these destructive relationships often need to be clarified before psychotherapeutic cooperation begins.
Therapy.
Behavioral therapy (especially for delineated, formalized symptoms of obsession, as well as for massive social restrictions caused by obsessive symptoms); systemic therapeutic method (for example, the patient’s description of his symptoms, their intended assessment and the method of behavior change proposed for communication therapy); for persons capable of introspection - disclosure-oriented analytical psychotherapy. Destructuring and psychotherapeutic interventions requiring regression often lead to the emergence of fear, and therefore psychoanalysis should be carried out only after a thorough examination and when indicated. Obsessive symptoms often occur as precursors to psychosis. In this case, analytical psychotherapeutic intervention is strictly contraindicated (differential diagnosis). The basic rule for the treatment of psychosis is therapeutic measures.
Neurotic depression.
(synonym - “depressive neurosis”; according to DSM III nomenclature - “dysthymic disorders”)
Clinical symptoms. The leading symptom is a prolonged depressive mood (sadness, despondency, depression) or a lack of joy and interest in usual activities and pastimes. This is accompanied by individual manifestations of depressive syndrome (decreased appetite, weight change, sleep disturbances, psychomotor inhibition or agitation, decreased activity, general decreased performance, social decline, feelings of inferiority or guilt, impaired concentration, slowness of thoughts and speech, painful indecision , hypochondriacal fears, thoughts of death and suicide, often suicidal plans and attempts).
Differential diagnosis . Neurotic depression should be distinguished from exhaustion depressions, reactive depressions and so-called endogenous depressions. From the so-called conflict of reactions or violation of adaptation. Neurotic depression is characterized by duration and recurrent course. The mourning response can develop into deep depression, but it is a normal response to rejection from a loved one. When depression lasts more than two years without remission and manifests itself in excessive depression, motor retardation, a pronounced decrease in performance, a feeling of worthlessness and guilt, we should talk about a complicated mourning reaction and its depressive-neurotic processing. The diagnosis of endogenous depression, as a rule, indicates the severity of the disease and suggests organic causes, and also indicates the absence of a causal relationship with external stressful preconditions. Often, a clear distinction between endogenous and neurotic depressions is controversial. The differential diagnostic distinction also includes the definition of “psychotic depression” within the framework of manic-depressive psychosis.
Psycho- and sociodynamics of neurotic depressions.
Neurotic depression, as their name implies, is the result of neurotic processing of conflict. This is, as a rule, a conflict associated with aggression, a subjective refusal to say goodbye to a loved object, a subjective denial of the existing one, an internalized ideal solution that has not been processed narcissistically, and in extreme cases, a general violation of narcissistic integrativeness, which often leads to suicidal actions. Depression corresponds to the concept of “a reversal of aggression against one’s own person,” despite the fact that aggression against a loved one, an object that is existentially connected with the patient, alienated from him by an enemy or by one’s own hatred, passes. The turn of aggression against one’s own person is equivalent to an attempt to hold on to a (long-lost) object: the picture of the death of a loved one can remain and be held in one’s own internal space, while initially death acts as a reproach, and therefore abandonment manifests itself with complaints about one’s own torment. Often depression is a subconscious attempt to at least replace a lost object with held suffering or (literally) bring that object closer with suffering. In other cases related to the narcissistic sphere, depression means a collapse of the narcissistic equilibrium due to resentment (a return to narcissistic claims to the environment) or even a return to following internal ideal ideas (about beauty, success, love appeal). Sometimes suicide represents a last attempt to restore one’s lost narcissistic unity (“one’s own face”). In practice, all depressive reactions are actualized more or less intensely, just like the feeling of helplessness and impotence in childhood - with the impossibility of establishing a connection with an existential object that serves as a source of love and protection. This makes depression extremely vulnerable to real, even minimal experiences of rejection, as a result of which even interruption of communication with a psychotherapist and a break in psychotherapeutic sessions due to the doctor's vacation can lead to an increased risk of suicidal reactions. The seemingly unreasonable fixation on suffering, the emphasized attention to the aspects of life that cause suffering and the immanent provocation of a return to the past through the sooner or later demand for help gives depression the devaluing label of masochism. One must try to avoid increasing suffering (feelings of guilt, mortal fear of rejection, absolute, unbearable self-deprecation) through supervision and restraint. Reproaches from others or even favorable encouragement, as well as a simple call to put an end to the past, can in this situation increase depressive self-reproaches (self-blame).
Therapeutic strategy.
The main thing in the therapeutic strategy is to establish the fact of depression and the ability to alleviate the patient’s suffering. In further therapeutic plans, and especially in chronic depressive disorders, the possibility of alcohol abuse and psychotropic drugs as possible complicating factors should be taken into account, as well as the possibility of increasing suicidal risk with premature stress aimed at revealing the internal mechanisms of depression, or the insufficiency of prescribed psychopharmacological therapy.
Psychodynamics of neuroses and personality disorders. – previous | next – Personality Disorders Clinic.
PSYCHIATRY. PSYCHOSOMATICS. PSYCHOTHERAPY. Table of contents.
Conversion disorder - treatment
If you experience symptoms of conversion disorder, you should seek immediate medical attention as the symptoms may be caused by an underlying medical condition.
The first line of treatment is to determine the underlying cause. Once the patient figures out what the cause is, they can work on solutions to relieve as much stress and emotional trauma as possible. Relieving triggers should in turn reduce physical symptoms.
Suggested treatments for conversion disorder may include:
- treatment of any underlying mental disorders such as depression
- cognitive behavioral therapy (CBT)
- psychotherapy
- relaxation techniques such as meditation or yoga
- physiotherapy
- maintaining a healthy work-life balance
- support from friends and family
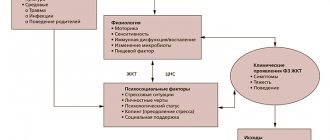
Clinical manifestations
The main manifestations of neurosis and hysteria are:
- Motor disorders - can be expressed in partial or complete paralysis of the limbs, hyperkinesis, tremor.
- Sensory disorders - manifested in anesthesia, hypoesthesia or hyperesthesia. Often there is pain in different parts of the body, narrowing of visual fields.
- Autonomic disorders - include gastrointestinal disorders, fainting, rapid heartbeat.
- Actually, mental manifestations include sharp emotional reactions, mood swings with fears, tearfulness, resentment, and conflict.
Origins of the disease
The specific causes of the development of hysterical personality disorder have not been established. Psychiatrists believe that the occurrence of the disease is associated with three factors: genetic characteristics, the family upbringing system and organic brain damage in childhood.
Inherited character traits are different, but with hysterical psychopathy, transmission from parents of increased impressionability, emotionality and inability to notice small details is often detected. Damage to brain structures may be associated with pregnancy, childbirth, or early childhood.
In psychoanalysis, it is believed that a hysterical personality is often formed when parents transmit to their children attitudes that people initially have different power depending on their gender. status, social position. This occurs in a child’s childhood, including when adults refuse to accept his emerging sexuality. Not all psychiatrists agree with the opinion of psychoanalysts.
Complications
These symptoms often lead to a person developing a tendency toward self-deception, which can reach an exaggerated degree. As a result, the patient always considers himself to be right, even if he commits antisocial acts or crimes. Hysterical personality disorder is typical for thieves, swindlers, rapists and other criminals.
Without treatment, hysterical psychopathy in women can lead to frigidity. At the same time, the patient arranges sexual provocations, flirts and shows sympathy for men. However, lasting relationships between them are not formed. Against the background of hysterical disorder, autonomic disorders are possible. These include nausea, increased body temperature, asthma attacks, movement disorders and other signs.
The main reason for their appearance is psychosomatics, which occurs as a reaction of the nervous system to severe psychological disorders. People with a hysterical personality are prone to a promiscuous sex life and abuse of alcohol and drugs. They are at increased risk of developing psychosis and depression, as well as other mood disorders.