Risk factors for strokes
- Diseases of the cardiovascular system: atrial fibrillation, heart failure, hypertension, arrhythmia, tendency to form blood clots, etc.
- Regular stress, chronic fatigue, overexertion.
- Age over 45 years for men and over 50 years for women.
- Migraine.
- Alcohol abuse, drug addiction, smoking.
- Metabolic disease.
- Diabetes.
- Excess body weight, sedentary lifestyle, unhealthy diet: eating fatty, spicy, fried, smoked foods.
- Long-term (more than 5 years) use of hormonal drugs.
- Heredity.
- Infectious and inflammatory processes (systemic lupus erythematosus, etc.).
- Gender: The risk of stroke is higher in men than in women.
These factors lead to a decrease in the elasticity of blood vessels, increased load on them, the formation of atherosclerotic plaques, and an increase in the amount of sugar and bad cholesterol in the blood.
Patients at risk should regularly check their health with a doctor, undergo a CT scan or MRI of the brain, conduct a study of the cerebral cortex, take a blood test for sugar and cholesterol levels, blood clotting, etc.
Types of stroke
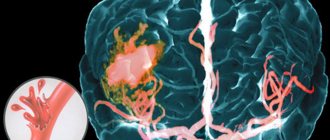
There are two main types of stroke: hemorrhagic, which occurs when blood vessels rupture (bleeding into the brain, under the membranes and ventricles of the brain), and ischemic, which occurs when blood vessels become blocked (thrombosis or embolization of blood vessels in the brain).
(more commonly known as cerebral hemorrhage) is a complication of hypertension. And this is the most acute type of stroke, which is an extreme manifestation of the diseases that cause it. Hemorrhagic stroke usually occurs in people with high blood pressure, usually against the background of a hypertensive crisis. It is also common for artery walls to rupture in places where they are too thin. This is due to aneurysms - congenital or acquired thinning and bulging of the walls of blood vessels. A blood vessel that cannot withstand the increased pressure on the wall ruptures. Hemorrhagic stroke most often occurs after a difficult, stressful day.
In the evening, your head literally bursts with pain, which leads to nausea, vomiting, and more and more headaches - these are terrible harbingers of a stroke. Symptoms of this stroke appear suddenly and get worse quickly. Movement, speech, sensitivity are impaired. The pulse becomes tense and rare, the temperature rises. There is slight numbness, and sudden loss of consciousness to coma is possible. Blood flows into the face, sweat appears on the forehead, the person feels a blow to the head, faints and falls - this is a hemorrhagic stroke. Blood from the ruptured vessel enters the brain tissue. After a few minutes, it can absorb and compress the brain matter, causing swelling and death.
Externally, a hemorrhagic stroke looks just as unattractive. In the blood vessels of the neck, the pulse quickens, screams, wheezing, loud breathing. Sometimes vomiting begins. Sometimes it is visible that the eyeballs begin to tilt towards the affected area. Paralysis of the upper and lower extremities may occur on the side opposite the affected area. Large bleeding begins to involuntarily move healthy limbs.
Primary prevention
About 80% of all strokes are primary. Basic preventive measures:
- Lifestyle changes. The patient must give up bad habits and a sedentary lifestyle, and start eating right. The diet should consist mainly of steamed, boiled and stewed dishes, low-fat dairy products, and fish. Be sure to drink about 8 glasses of water. Physical training should be age-appropriate; sometimes it is enough to add walking. Diet and moderate exercise will help normalize weight and improve health. It is equally important to eliminate or minimize stress, overexertion, and sleep 8 hours a day.
- Blood pressure control. Normal values are 120-140 mmHg. Art. for the upper and no more than 80-90 mm Hg. Art. for the bottom. The change must be made at the same time every day. If your readings increase, you should consult a doctor, he will select treatment and prescribe medications to stabilize your blood pressure.
- Controlling blood sugar and bad cholesterol levels.
- Taking medications , such as antithrombotic drugs.
Correction of diabetes manifestations
Among patients with IS, the frequency of detection of diabetes, according to various authors, ranges from 15 to 33%. Diabetes is an undoubted risk factor for stroke, but there is not much data on the role of diabetes as a risk factor for recurrent stroke.
Constant and adequate control of hypertension in patients with diabetes leads to a significant reduction in the incidence of strokes. Thus, the UKPDS (United Kingdom Prospective Diabetes Study) study showed a reduction in the risk of recurrent stroke by 44% among patients with diabetes with controlled hypertension compared with patients with a low level of control [43]. A number of other studies have also correlated a reduction in the risk of stroke and/or other cardiovascular events with blood pressure control in patients with diabetes. It is believed that among all antihypertensive drugs, ACE inhibitors have the best effect on the outcome of stroke and other cardiovascular events for this category of patients [23, 39]. According to the recommendation of the American Diabetes Association, the treatment regimen for patients with diabetes and hypertension should include either ACE inhibitors or angiotensin receptor antagonists [9].
Timely and optimal glycemic control, leading to a reduction in the incidence of microangiopathies (nephropathies, retinopathy, peripheral neuropathy), is also extremely important for the primary and secondary prevention of stroke and other CVDs. The results of three randomized clinical trials (ACCORD, ADVANCE, Veterans Affairs Diabetes Trial) have been published, which assessed the effectiveness of intensive hypoglycemic therapy in patients with type 2 diabetes who had coronary artery disease, stroke, and other vascular risk factors in their history. In these studies, a reduction in the risk of cardiovascular events and death during intensive glucose-lowering therapy was not demonstrated.
The prospective, double-blind, randomized PROactive trial included 5238 patients with type 2 diabetes and a history of macrovascular events who received pioglitazone or placebo. After stroke, among patients (486 in the pioglitazone group, 498 in the placebo group), there was a trend towards a decrease in the combined rate of death and vascular events (p = 0.067) in the pioglitazone group. A secondary analysis found that pioglitazone reduced the incidence of fatal or nonfatal stroke (p = 0.0085) and death from cardiovascular events, as well as nonfatal myocardial infarction or nonfatal stroke (p = 0.0467) [45].
Thus, the basis of secondary prevention of IS in patients with diabetes is adequate control of hypertension and glycemia [29].
Secondary prevention
The main task of secondary prevention is to reduce the likelihood of developing a recurrent stroke to a minimum. Basic measures:
- Regular monitoring of blood pressure and reducing it to normal levels if necessary.
- Changing your diet: it is important to reduce the amount of salt consumed, eat more vegetables and fruits, low-fat dairy products, eliminate fatty, fried and smoked foods, and alcohol.
- Normalize weight, exercise for at least half an hour every two days.
- Drug therapy especially for patients with signs of atherosclerosis and patients who have experienced ischemic stroke or transient ischemic attacks. Medicines help lower cholesterol and blood pressure, cope with inflammatory diseases and exacerbations of chronic diseases.
- Regular visits to a neurologist. The doctor can monitor changes in the patient’s condition, adjust therapy, prescribe medications or procedures, and give recommendations regarding hospitalization.
In the future, this disease causes persistent disorders in the form of paresis, paralysis, speech disorders and vestibular disorders, which are the causes of disability and disruption of social adaptation of patients after strokes.
Symptoms that may indicate a stroke.
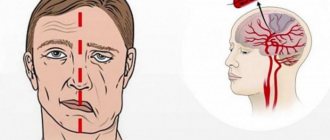
Facial distortion. You need to ask the person to smile, puff out his cheeks, and bare his teeth. A possible sign of a stroke is asymmetry of the nasolabial folds, the cheek “sails,” and the smile becomes “crooked.” Speech disorders. A sign of a stroke is when a person cannot pronounce words, or when it seems that the person does not understand what he is saying, “confuses” words. Weakness in an arm and/or leg. You can ask to squeeze your hands with both hands, or simply stretch both hands forward - the weak hand will begin to fall. Important: if a person complains of sudden clumsiness in his hand, the inability to write something clearly by hand is also a sign of weakness.
Why is it important to act quickly?
In an ischemic stroke, during which an artery is blocked by a blood clot, an area of the brain does not receive nutrition and brain cells die. In the absence of timely specialized medical care for a person with a stroke, the death of cells in the area of the brain that has lost its blood supply is inevitable. There is a technology for restoring blood supply to the brain, when a medicine that can dissolve blood clots is administered intravenously. This treatment method is called systemic thrombolytic therapy. It is possible to use systemic thrombolytic therapy only in the first 4.5 hours from the onset of a stroke. After 4.5 hours, brain tissue and cerebral vessels in the area of the infarction acquire irreversible changes and the risk of hemorrhage in the area of cerebral infarction increases many times over. There are two main types of strokes: 1. Ischemic (associated with blockage or spasms of arterial cerebral vessels and causing insufficient blood supply to the brain and death of nerve cells in the area of necrosis and the development of cerebral infarction); 2. Hemorrhagic (hemorrhage associated with rupture of a cerebral vessel (artery or vein) with blood leaking into the brain substance or under its membranes, compressing the surrounding nervous tissue, causing the death of neurons and stimulating the development and progression of cerebral edema).
Today, preventing the development of this pathology – primary and secondary prevention of stroke – is of great importance.
Risk factors for strokes
All areas of preventive work to prevent the development of strokes involve monitoring risk factors and their correction. All risk factors are divided into several categories: 1. Predisposing; 2. Behavioral; 3. "Metabolic". Predisposing factors include aspects that cannot be corrected: 1. age (the frequency of strokes increases after 50 years and grows every year); 2. gender (men over 40 years of age have a higher risk of developing strokes than women); 3. family history and hereditary predisposition. Behavioral factors that contribute to the development of strokes are: • smoking (doubles the risk of strokes); • psychological factors (stress, depression, fatigue); • taking alcohol, drugs and medications (oral contraceptives); • overweight and obesity; • atherogenic diet; • physical activity (physical inactivity increases the risk of ischemic strokes). “Metabolic” risk factors – arterial hypertension, dyslipidemia, metabolic syndrome, endocrinopathies (diabetes mellitus), coagulopathy. Individual drug correction of “metabolic” factors and elimination of behavioral aspects underlie the prevention of ischemic and hemorrhagic strokes.
Main directions of stroke prevention
The main etiological causes of the development of acute cerebrovascular accidents are considered to be atherosclerosis of cerebral vessels and hypertension in ischemic strokes, and malignant hypertension against the background of cerebral vascular pathology (aneurysms, arteriovenous malformations, diabetic angiopathy and other vasopathies) in hemorrhagic strokes. In this regard, the main directions of primary and secondary prevention of strokes are: • active identification and adequate treatment of patients with primary arterial hypertension or essential hypertension; • prevention of ischemic strokes (cerebral infarction) in patients with pathology of the heart and blood vessels (rhythm disturbances, heart defects, myocardial infarction and endocarditis) and timely treatment of these diseases; • prevention of repeated acute disorders of cerebral circulation in patients with transient ischemic attacks or “minor” strokes, including surgical treatment methods; • drug therapy for lipid metabolism disorders in persons with atherosclerotic lesions of cerebral vessels, carotid arteries and in patients with coronary artery disease.
Primary prevention of strokes
Primary prevention of stroke is a set of measures aimed at preventing the development of acute cerebral circulatory disorders - hemorrhagic stroke or cerebral infarction (ischemic stroke) - maintaining a healthy lifestyle, balanced nutrition, maintaining adequate body weight, abstinence from smoking and adequate drug treatment of heart and vascular diseases , diabetes and other diseases.
Drug correction for the prevention of cerebral infarction
Ischemic stroke occurs much more often - from 75 to 80% of all cases of acute cerebrovascular accidents. The occurrence of cerebral infarction occurs, as a rule, against the background of atherosclerotic changes in the walls of cerebral vessels in combination with high blood pressure, damage to the heart valves (congenital or acquired defects) and/or cardiac arrhythmia (atrial fibrillation). Prevention of strokes includes timely treatment with medications: • lipid-lowering therapy (use of statins); • antihypertensive therapy; • effective treatment of somatic diseases and infectious and inflammatory processes that contribute to the development of strokes (collagenosis, chlamydia, HIV coagulopathies, diabetes mellitus); • the use of herbal preparations and folk remedies to normalize lipid metabolism and lower blood pressure (together with drug therapy).
Use of lipid-lowering drugs
Atherosclerosis occurs as a result of lipid metabolism disorders and the development of hypercholesterolemia. Cholesterol is deposited on the inner lining of blood vessels, forming atherosclerotic plaques that impede the flow of blood through the vessels - the heart, brain and other organs. Their ulceration with separation of part of the plaques leads to obliteration of the cerebral artery - disruption of the nutrition and respiration of nerve cells, leading to necrosis of neurons with the formation of cerebral infarction. A long-term increase in blood cholesterol levels by 10% leads to an increase in the risk of cerebral infarction to 25-30%. Statins are drugs that reduce plasma lipid levels and the increased formation and deposition of cholesterol in the form of cholesterol plaques and reduce the risk of ischemic stroke and myocardial infarction.
Antihypertensive therapy prescriptions
Increased blood pressure is a major and highly treatable risk factor for the development of both hemorrhagic and ischemic strokes. A frequent complication of hypertension or primary arterial hypertension is repeated cerebral hypertensive crises with an acute increase in blood pressure, which are accompanied by the death of myocytes of the vascular wall, which leads to the formation of multiple aneurysms with the development of cerebral hemorrhage. Or to swelling of the walls of cerebral arteries and arterioles, their narrowing or closure of the lumens with the development of small deep cerebral infarctions. Prevention of cerebral strokes consists of monitoring blood pressure followed by the prescription of antihypertensive drugs - ACE inhibitors, calcium channel blockers, diuretics or angiotensin II receptor blockers with individual selection of the drug in each specific case. Antihypertensive drugs are taken for a long time until the optimal blood pressure level is stabilized, with mandatory correction of therapy by the attending physician (cardiologist or therapist).
Features of primary prevention of ischemic stroke in women
Today, ischemic strokes between the ages of 18 and 40 often develop in women due to long-term use of oral contraceptives, during pathological pregnancy and dyshormonal disorders (due to increased estrogen levels, leading to increased blood clotting and blood clots) . And also with frequent and prolonged migraine attacks, which are accompanied by prolonged spasm of cerebral vessels, in combination with smoking, which causes prolonged vascular spasm and intoxication of the body, contributes to the progression of degenerative processes in cerebral vessels. The basis for preventing the development of acute ischemic cerebrovascular accident in women is: • giving up smoking and other bad habits; • monitoring blood pressure and taking antihypertensive drugs; • rational nutrition and maintaining a healthy lifestyle with physical activity; • adequate intake of oral contraceptives with monitoring of hormone levels and consultation with a gynecologist-endocrinologist; • treatment of hormonal imbalances and diseases that provoke its changes (mastopathy, endometriosis, polycystic ovary syndrome).
Secondary prevention of ischemic and hemorrhagic strokes
Secondary stroke prevention is a comprehensive program to prevent the development of recurrent stroke, which includes non-drug and drug methods. Non-drug methods include: • quitting smoking and other bad habits (alcohol, drug addiction); • hypocholesterol diet; • gradual increase in physical activity (physical therapy, massage, walking); • reduction of excess weight.
Therapeutic measures to prevent recurrent stroke:
• antithrombotic drugs (antiplatelet agents and indirect anticoagulants); • treatment with antihypertensive drugs; • prevention of stroke with folk remedies; • surgical treatment (carotid endatherectomy).
Modern antithrombotic therapy
The use of antithrombotic drugs today is an important element in the prevention of recurrent strokes. For this purpose, acetylsalicylic acid (aspirin), ticlopidine, clopidogrel and dipyridamole are mainly used. Preventive antithrombotic therapy is carried out long-term and continuously (for several years) under the control of platelet aggregation examination before prescription and a few days after the start of antiplatelet therapy. An increase in platelet aggregation activity in patients at risk of developing ischemic stroke and effective drug correction of this pathology are one of the criteria for the need to prescribe antiplatelet agents.
Preventing strokes in high-risk groups
Stroke prevention is carried out jointly by therapists and neurologists. Antiplatelet agents and indirect anticoagulants, lipid-lowering and antihypertensive drugs are used to prevent ischemic and hemorrhagic cerebral strokes, as well as myocardial infarction. The success of surgical interventions on the great vessels of the brain in most cases depends on the state of the patient’s cardiovascular system, and to perform coronary artery bypass surgery, a comprehensive assessment of the cerebrovascular reserve and the state of the cerebral vascular system as a whole is necessary. To achieve a significant reduction in the incidence of strokes, a combination of primary prevention in high-risk groups and a general national strategy for the prevention of cerebrovascular pathology is necessary.
Prevention of ischemic stroke
Measures to prevent ischemic stroke, in addition to those listed above, include drug therapy. All medications must be prescribed by a doctor. Typically these medications are:
- preventing the formation of blood clots;
- lowering cholesterol levels;
- increasing the tone of blood vessels and strengthening their walls;
- activating metabolism in the brain;
- having a calming effect.
If you or your family have experienced a stroke, take care of your health and contact. Rehabilitation after a stroke will allow you to recover and reduce the risk of developing a recurrent vascular accident.
Antiplatelet therapy
The effectiveness of the use of antiplatelet agents to prevent recurrent IS has been confirmed by many researchers. Four antiplatelet drugs have been shown to reduce the risk of recurrent IS after stroke or TIA.
The results of a meta-analysis of data from 287 studies, including 212 thousand patients with a high risk of occlusive vascular events, showed that against the background of antiplatelet therapy, the number of cases of non-fatal stroke decreased by an average of 25%, and vascular mortality - by 23%. Moreover, according to a meta-analysis of 21 randomized trials that compared antiplatelet therapy with placebo in 18,270 patients who had a stroke or TIA, antiplatelet therapy leads to a 28% relative risk reduction in nonfatal stroke and a 16% relative risk reduction in fatal stroke [ 10].
Acetylsalicylic acid
The clinical effectiveness of ASA for the secondary prevention of IS was first shown in 1977. Subsequently, numerous international placebo-controlled studies demonstrated that ASA at a dose of 50–1300 mg/day is effective in the prevention of recurrent IS or TIA [10, 15].
The first experience in world clinical practice of using small doses of ASA (1 mg/kg/day) in patients with cerebrovascular pathology due to hypertension, carried out at the Research Institute of Neurology of the Russian Academy of Medical Sciences, showed a rapid and persistent elimination of platelet hyperaggregability due to an almost 3-fold decrease in the initial concentration of thromboxane A2 in the blood regardless of the gender of patients and the type of ischemic cerebrovascular accident. The study included patients with TIA and post-IS [5].
Two large international controlled studies compared the effectiveness of different doses of ASA for patients with TIA or IS (1200 vs. 300 mg/day and 283 vs. 30 mg/day) [25, 40]. In both studies, high- and low-dose ASA was effective in preventing IS, but higher doses of ASA were associated with a higher risk of gastrointestinal bleeding [10].
When choosing the optimal daily dosage of ASA for the prevention and treatment of IS, its side effects play an important role. Like other non-steroidal anti-inflammatory drugs, ASA can have both local (due to irritation of the mucous membrane) and systemic (by reducing the synthesis of prostaglandins) damaging effects on the mucous membrane of the gastrointestinal tract (GIT) when taken orally, including. including the occurrence of erosions and ulcers, as well as the development of gastrointestinal bleeding. The frequency of this complication directly depends on the daily dose. Thus, the side effect of ASA on the gastrointestinal mucosa decreased when taking 300 mg/day compared with the use of higher (1200 mg/day) doses of ASA and amounted to 31 and 41%, respectively, for discomfort in the abdominal area, 3.1 and 4. 8% for gastrointestinal bleeding (UK-TIA Study Group, 1991) [25]. At the same time, the ESPS 2 (European Stroke Prevention Study 2) study showed that low doses of ASA do not completely eliminate its ability to induce bleeding [19].
To eliminate the adverse effect of ASA on the gastrointestinal mucosa, various dosage forms with an enteric coating have been proposed, for example thrombo ASA. Absorbed from the upper part of the small intestine, this drug causes local ulcerogenic effects to a much lesser extent.
Ticlopidine
The effectiveness of ticlopidine (thienopyridine) was assessed in three randomized trials in patients with cerebrovascular disease. The CATS (Canadian-American Ticlopidine Studi) trial compared the effectiveness of ticlopidine 250 mg/day with placebo in the prevention of stroke, MI, or death due to vascular pathology in 1053 patients with IS. Ticlopidine has been shown to lead to a 23% reduction in the relative risk of meeting the combined endpoint of the study [27]. The TASS (Ticlopidine Aspirin Stroke Study), which compared the effectiveness of ticlopidine (250 mg twice daily) and ASA (650 mg twice daily) in 3069 patients with a recent minor stroke or TIA [30], demonstrated a reduction in the relative risk of stroke. by 21% over a 3-year follow-up, as well as a slight (9%) reduction in the risk of end events (stroke, MI, death due to vascular pathology) when using ticlopidine.
The most common side effects of ticlopidine: diarrhea (approximately 12%), gastrointestinal symptoms, rash, hemorrhagic complications, are identical to those that occur when taking ASA. Neutropenia was observed in approximately 2% of patients receiving ticlopidine in the CATS and TASS studies. However, the incidence of particularly severe complications was less than 1%; in almost all cases they were reversible and disappeared when the drug was discontinued. In addition, thrombocytopenic purpura has been described.
Clopidogrel
The effectiveness of clopidogrel was assessed in comparison with ASA in the CAPRIE study (Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events, [14]). More than 19 thousand patients with stroke, MI or peripheral vascular disease were randomized to receive ASA at a dose of 325 mg/day or clopidogrel at a dose of 75 mg/day. The primary end event - IS, MI, death due to vascular pathology - occurred with a frequency of 8.7% lower in patients receiving clopidogrel compared to the ASA group.
Two studies [12, 36] indicated a relatively greater effectiveness of clopidogrel (compared to ASA) for patients with diabetes and patients who have already had an ischemic stroke or myocardial infarction. In general, clopidogrel is safer when taken compared to ASA and especially ticlopidine. Clopidogrel, like ticlopidine, was less likely to cause gastrointestinal symptoms and hemorrhage compared to ASA. Neutropenia was not noted at all; there were isolated reports of the occurrence of thrombocytopenic purpura [11].
Thus, clopidogrel is slightly more effective than ASA in preventing vascular events. Clopidogrel may be more effective in patients with high vascular risk (history of stroke, peripheral arterial atherosclerosis, symptomatic coronary artery disease, or diabetes) [28].
Dipyridamole sustained release
Dipyridamole is close to ASA in its effectiveness in reducing the risk of recurrent strokes [19].
Combined antiplatelet therapy
Taking into account the different points of application and mechanisms of action of drugs with an antiplatelet effect, as well as the variability of the platelet response, their combined use to achieve an additive effect of aggregation inhibition seems theoretically justified.
Combination of clopidogrel and ASA
The MATCH (Management of Atherosclerosis with Clopidogrel in High-Risk Patients with Recent Transient Ischemic Attack or Ischemic Stroke, [18]) study, involving 7599 patients who had suffered an IS or TIA and had additional risk factors, assessed the effectiveness and safety of combination therapy, which included clopidogrel 75 mg and ASA 75 mg/day in relation to clopidogrel monotherapy at a dosage of 75 mg. The primary outcome event was a composite of stroke, myocardial infarction, death due to vascular pathology, or rehospitalization associated with ischemic episodes. There was no significant benefit of combination therapy over clopidogrel monotherapy in reducing the incidence of primary endpoints or recurrent ischemic events.
The effectiveness of combination therapy with clopidogrel (75 mg/day) and ASA (325 mg/day) compared with ASA monotherapy (325 mg/day) was assessed in the CHARISMA (Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization Management and Avoidance) study. After 30 months of observation of patients, the incidence of the combined endpoint, which included IS, MI, death from a vascular cause in patients receiving combination antiplatelet therapy, was 6.8% and was less than in the group of patients receiving ASA monotherapy, where this indicator was 7.3% (p = 0.22). Thus, the study did not demonstrate the advantages of combination therapy with clopidogrel and ASA compared with ASA monotherapy for this category of patients [28, 29].
Combination of dipyridamole and ASA
In the ESPS-2 study (European Stroke Prevention Study, [19]), 6602 patients with a history of stroke or TIA were randomized, taking into account the main risk factors for the development of ischemic brain injury, into groups of different regimens of extended-release dipyridamole and ASK. A significant reduction in the risk of stroke was achieved with ASA alone by 18%, dipyridamole alone by 16%, and the combination of both by 37%. No reduction in the risk of death was observed with any of the dosage regimens used. The effectiveness of combination therapy compared with ASA monotherapy was observed in reducing the risk of recurrent stroke (by 23%) and was 25% higher than the effectiveness of dipyridamole monotherapy.
Similar results were obtained in the international randomized, non-blinded study ESPRIT (European/Australian Stroke Prevention in Reversible Ischaemia). The purpose of one of the directions of this study was a comparative analysis of the effectiveness and safety of the combination of ASA (30–325 mg/day) with slow-release dipyridamole (400 mg/day) and ASA monotherapy (30–325 mg/day) in patients who had suffered a TIA or IS ( with a neurological deficit assessed as no more than 3 points on the modified Rankin scale) within 6 months before inclusion in the study. It is important to note that the study included only patients who had suffered atherothrombotic cerebrovascular accidents: 1363 received combination therapy, 1376 received monotherapy. The primary endpoint (vascular death, non-fatal IS, MI, symptomatic hemorrhagic complications) was achieved by 16% of patients receiving ASA monotherapy and 13% of patients receiving combined antiplatelet treatment (hazard ratio [HR] = 0.8; 95% confidence interval [CI] – 0.66–0.98), which allowed the authors to conclude that the combination of ASA and dipyridamole is more effective than ASA in the secondary prevention of vascular complications of IS of atherothrombotic origin. Following the publication of the ESPRIT results, a meta-analysis of studies on the combined use of dipyridamole and ASA, which included all the studies described above, confirmed the reliability of the conclusions of the ESPRIT study [7].
The results of the ESPS-2 and ESPRIT studies formed the basis of the ESO (2008) recommendations for secondary stroke prevention, in which the combination of ASA and slow-release dipyridamole is a first-line drug (along with clopidogrel) as an effective antiplatelet therapy (Class I, level of evidence A ). It should also be noted that for those in whom secondary prophylaxis with oral anticoagulants is indicated but is contraindicated, the ESO also recommends a combination of slow-release dipyridamole and ASA (although the level of evidence for this recommendation is low - class IV, GCP - Good Clinical Practice).
Thus, the range of drugs - antiplatelet agents - with proven efficacy and safety in multicenter studies is quite wide, and therefore the question of choosing an oral antiplatelet agent is logical. When choosing antiplatelet drugs after stroke or TIA, the influence of several factors should be taken into account. Concomitant somatic pathology, side effects, and the cost of the drug may influence the choice of therapy: monotherapy with ASA, clopidogrel or a combination of ASA and dipyridamole. The low cost of ASA promotes its long-term use. However, if you look at it differently, even a small reduction in the frequency of vascular episodes observed with the use of dipyridamole or clopidogrel suggests a certain adequacy of the cost-effectiveness ratio of the drugs, which is comparatively more noticeable than with ASA. In patients who cannot tolerate ASA due to allergies or gastrointestinal side effects, clopidogrel or dipyridamole should also be recommended. The combined use of ASA and clopidogrel may be acceptable for patients who have recently suffered an acute coronary attack or stenting surgery [46].