If you want to get advice on treatment in Moscow. Fill out the form below:
We are often asked for advice with this question. Indeed, relatives and the patient himself are often left to their own devices. As such, there is no state rehabilitation program yet. Moreover, we also do not have a universal answer.
One thing we know for sure is that all patients and their relatives have the same goal: a speedy restoration of function and a return to normal life. The goal is one, but the paths to it are different, often long and, sadly, dead-end...
When treating a stroke, the situation very often develops as follows. A man is admitted to the hospital. The life of family and friends changes dramatically. Anxiety for a loved one, changes in work schedule, financial costs for medications, caregivers and consultations. And when you get discharged, it turns out that everything is just beginning: equipping an apartment, hiring caregivers, or temporarily stopping work for one of your relatives. And the prices for rehabilitation make you feel uneasy...
Yes, everyone’s financial capabilities are different! Yes, many people have to rely only on themselves! Yes, there are no clear and understandable government programs, for example, for a heart attack!
- Well, no, no trial!
Let's try to calculate everything ourselves and make the right decision.
Americans, for example, are a mercantile people and far from stupid. They once calculated that every dollar invested in treatment, without further rehabilitation, turns into 17 dollars spent in the future. Let's just count in money. It is important. Just numbers Average monthly drug treatment for stroke: from 2 to 7 thousand rubles.
Depending on the degree of dysfunction, complications and concomitant pathologies. Let's add to this a nurse or the financial losses of relatives if they are present and caring for the patient. Another 20-30 thousand monthly. All methods of motor and speech rehabilitation cannot be implemented on your own. Whatever one may say, at the first stages you will have to invite specialists. Preferably at least. There are a lot of subtleties, no matter what they write on the Internet. This is also money. Now all that remains is to add up all these numbers and multiply by the number of months. At 6 for example...or at 12...
The numbers may, of course, vary. There are different types of strokes. And if you don’t look at the numbers, but think about the time for effective rehabilitation, which we already have little of. In the end, we need to put our loved one back on his feet. Return to society, learn to drive a car again. And this is possible in modern conditions. So it turns out that the amounts are ultimately comparable, but the effects and results are radically different.
If you have read this far and haven’t given up on this idea without taking our word for it, let’s look for solutions and minimize costs.
If you or your loved ones need medical assistance, contact us. The site’s specialists will recommend a clinic where you can get effective treatment:
The first way. Rehabilitation center after stroke
Even before discharge from the hospital, select a rehabilitation center based on the functional equipment, capabilities of the center and the patient’s condition. Many centers do not accept bedridden patients. This is a fact that must be taken into account.
Also, you can count on rehabilitation according to the so-called quota . They don’t take seriously ill or bedridden patients, but if their condition allows it, it’s worth “fighting” for the quota. Naturally, commercial rehabilitation centers working according to European methods do not work according to quotas. But the approach, to put it mildly, varies. A distinctive feature of good centers is an individual approach, round-the-clock care and fast rehabilitation times with the maximum possible restoration of functions. There are also worthy centers among government institutions, but you won’t get away from the continuous approach.
Duration of non-drug treatment
Physiotherapy is applied in limited courses (from 10 to 30 days), which can be repeated (for example, in spring and autumn).
Psychotherapy is a long-term treatment method. For example, the average course of such a common type of psychotherapy as cognitive behavioral therapy takes several months. Although there are also one-time psychotherapeutic sessions and trainings designed for one or several sessions (the so-called short-term psychotherapy).
The second way. Combined approach
If you are denied a quota due to the patient's condition. In this case, you can combine the approach, and thereby, in fact, save the patient’s life. A short course of rehabilitation in a good paid center, and then rehabilitation under a quota. By the way! Even if you initially cannot pay for paid rehabilitation, be sure to visit good centers.
Show medical documentation, get advice from highly qualified specialists. At the very least, this will help you navigate the deadlines and outline a further rehabilitation plan. It is at least unreasonable to miss such an opportunity!
Duration of pharmacotherapy (medication)
Pharmacotherapy in the treatment of mental disorders and behavioral disorders is divided into:
- Active. It is usually carried out for a limited period of no more than 1-2 months to relieve the painful condition.
- Supportive. It is carried out after the condition has stabilized. Can last for months and years .
Groups of drugs such as tranquilizers and neurometabolic therapy are used in short courses, while antidepressants, mood stabilizers, and antipsychotics can be used for a long time (if necessary, throughout life).
The third way. Recovery after a stroke at home
If this is the case, study as much information as possible. Information that is objective and adequate. You should not do the exercises “in a hurry.” An arm, then a leg. This is where the biggest mistake lies. Rehabilitation measures are only successful when they are applied systematically and continuously. Buy a rehabilitation manual in video format. Consult with really smart rehabilitologists. And be patient.
Whenever possible, try to get qualified help .
We apologize if the material in this article seemed harsh and uncompromising to you. But if you look at it, the lives, health and well-being of both patients and their relatives are at stake.
Take care of yourself!
What to do if you have a stroke?
How to prevent a stroke, properly provide assistance and mitigate its consequences, said Inna Borisovna Tsyngeeva, head of the neurology department No. 2 of the Republican Vascular Center of the N.A. Semashko Republican Clinical Hospital.
Strokes happen only in old age.
Is it so? – Indeed, in most cases, people over 60 years of age are susceptible to stroke. However, our lifestyle, unhealthy diet, and physical inactivity lead to strokes becoming younger,” notes Inna Borisovna. – Unfortunately, we have an increased number of patients with strokes, whose age is 35-40 years. If a stroke occurs at a young age, it is worth understanding that the person has a chronic disease, blood disorder, or autoimmune disease. If you are over 60 years old, this is most likely due to vascular diseases: hypertension, atherosclerosis, a consequence of improper correction of risk factors.
Who is at risk and what are the risk factors?
– As with heart attacks, men are more vulnerable. Women before menopause have estrogen protection, explains the doctor. – But women who have reached menopause and older are also at risk. Modern women are workers, breadwinners of the family and at the same time mothers and housewives. And as a result, colossal emotional and physical stress equalizes the risk of stroke.
Speaking about risks, the doctor emphasized the importance of monitoring and timely correction of behavioral risk factors. These are low physical activity, smoking, lack of proper rest, reaction to stressful situations, consumption of large amounts of fatty meat and refined foods. A combination of several factors, which is not uncommon in modern people, further increases the risks of stroke and heart attack.
How is an ischemic stroke different from a hemorrhagic stroke?
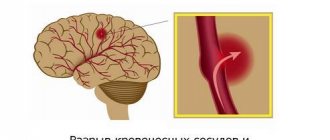
– Ischemic stroke occurs as a result of blockage of a vessel by a detached thrombus or as a result of the growth of an atherosclerotic plaque. There is only one result: blood does not flow, oxygen supply to the brain area is disrupted.
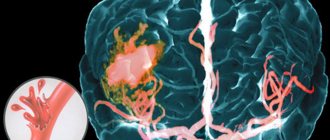
Hemorrhagic stroke is the most dangerous, often ending in death; against the background of high pressure, a vessel ruptures and blood flows into the brain tissue and cranial cavity.
According to statistics from the Republican Vascular Center, every 10-12th person dies, and 50% of patients become disabled after a stroke. Some are to a greater extent completely immobilized and need constant care, others are to a lesser extent, with a slight deficiency, after 3-4 months of rehabilitation they recover and return to normal life.
"Golden time"
“When you have a stroke, every minute is precious, and the patient’s life depends on how quickly the stroke is recognized and timely and correct assistance is provided,” the doctor emphasizes. – It is very important to inform people about risk factors and early signs of stroke, which will help, most importantly, to save life and minimize the patient’s disability. The “golden window” is 4.5 hours when, in the event of an ischemic stroke, a blood clot can be dissolved or, with the help of neurosurgeons, an operation can be performed to remove the blood clot from the lumen of the vessel. Thanks to the new thromboaspiration technique, the patient’s chances of recovery increase significantly. In the event of a hemorrhagic stroke, timely surgery will save life and cause less damage to brain tissue. It is also important to understand that the presence of chronic diseases, such as diabetes, arrhythmia, atherosclerosis, which were the cause of the attack, complicates the course of the stroke and the period of recovery of the body after.
What are the characteristic signs of a stroke that everyone should know?
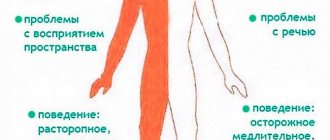
- So, let's remember. If you notice that something is wrong in the face: if a person cannot smile symmetrically, half of the face is distorted, one eye may not close, the corner of the mouth is drooping. Speech is impaired, as if there is “porridge in the mouth”; the person cannot raise an arm or leg. Sound the alarm, call an ambulance. Remember, your attentiveness will help save the life of a person, perhaps a dad, mom, grandma, grandpa, or even a stranger.
Be attentive to your loved ones,” Inna Borisovna urges. – It happens that a spouse took alcohol, took a steam bath, and he became ill, had a stroke, those around him do not notice, they blame everything on alcohol, and time passes. Don’t be indifferent, don’t pass by on the street, when you see that a person is feeling unwell, come up and ask, maybe it’s a stroke. Then you need to urgently call an ambulance by phone. 03, 103.
How can I help before the doctors arrive?
– Before the ambulance arrives, it is necessary to lay the patient down with his head elevated. If you feel nauseous, turn your head to the side, provide rest and access to fresh air. Take off tight clothes, unfasten your tight belt and tie. Under no circumstances should you give anything to drink or eat, as pharyngeal functions may be impaired and the person may choke. Also, the patient should not get up and walk. Until the ambulance arrives, you need to stay with the patient, then convey to the doctors all the information you know.
How can you prevent a stroke?
– According to experts, most strokes occur due to the growth of atherosclerotic plaques in the vessels. If you have high cholesterol, that is, it is above 5 millimoles per liter, you need to sound the alarm. It is necessary to regularly monitor blood pressure and take a cholesterol test twice a year. If it is elevated, it is necessary to follow a diet, limit fatty meats, and take statins as indicated. And these rules are not discussed, it’s like brushing your teeth,” says the neurologist. – At any age, you need to monitor your weight, the body mass index (BMI) should be less than 25. To do this, you need to consume less refined fats and carbohydrates, give up alcohol and smoking, and walk more. It's advisable if you exercise, but consult your doctor before engaging in strenuous exercise. If the vessels are already changed, then excessive load can lead to rupture - hemorrhagic stroke. Follow your doctor's recommendations and take prescribed medications correctly. Rest, get enough sleep and think positively!
Distribution of “risk factors” for the development of cerebrovascular insufficiency
( G. J. Hankey ,
J. M. Wardlaw , 2002 ) _ _ _
| The most important “Risk Factors” | Frequency of occurrence of the factor in patients with signs of cerebrovascular accident |
| Tendency to increase blood pressure | 50 – 75% |
| Heart diseases | 35 – 40% |
| Lipid disorders | 40 – 45% |
| Abuse of alcohol, smoking | 10 – 20% |
| Increased salt intake | 25 – 30% |
| Excess body weight | <15% |
| Unfavorable heredity | 5-10 % |
| Frequent stressors | 5% |
| Physical inactivity | 8% |
Stroke is divided into hemorrhagic and ischemic (cerebral infarction). Ischemic stroke accounts for about 80%, although recently published data in the journal Stroke (Shiber JR, Fontane E, Adewale A. Stroke registry: hemorrhagic vs ischemic strokes. Am J Emerg Med. Mar 2010;28(3):331-333), based on a retrospective review of data obtained from stroke centers increased the proportion of hemorrhagic stroke to 40.9%. The authors attribute this increase to improved diagnostics due to the use of SCT and the increased use of antiplatelet agents and warfarin.
According to the nature of the course, a small stroke is also distinguished, in which the impaired functions are completely restored during the first 3 weeks of the disease. However, such relatively mild cases occur in only 10-15% of stroke patients.
Transient cerebrovascular accidents (TCI)
are characterized by the sudden onset of focal neurological symptoms that develop in a patient with vascular disease (arterial hypertension, ischemic heart disease, rheumatism, etc.) and last several minutes, less often – hours, but no more than a day and end with complete restoration of impaired functions.
Transient neurological disorders with focal symptoms that develop as a result of short-term local cerebral ischemia are also referred to as transient ischemic attacks (TIA).
A special form of PNMK is acute hypertensive encephalopathy (AHE).
More often, acute hypertensive encephalopathy develops in patients with malignant arterial hypertension and is clinically manifested by severe headache, nausea, vomiting, impaired consciousness, convulsive syndrome, and in some cases is accompanied by focal neurological symptoms.
The appearance of a TIA or minor stroke indicates a high risk of repeated and, as a rule, more severe stroke (since the pathogenetic mechanisms of these conditions are largely similar) and requires their prevention. Recent population-based and hospital-based epidemiological studies have demonstrated a high risk of stroke immediately after TIA. Studies have shown that prompt evaluation of patients with TIA in the clinic and immediate initiation of treatment reduces the risk of stroke after TIA. This emphasizes the need for emergency hospitalization of patients with TIA for evaluation and immediate treatment.
When can relatives not be allowed into intensive care?
Relatives are not allowed in if there is a threat to the health of an intensive care patient, that is, with signs of an infectious disease, including a runny nose. The ICU patient is weak and it is extremely difficult for his body to resist infection.
Children are not allowed and there are enough reasons for that. Firstly, a child with an infection does not realize that he is not healthy, especially since his activity decreases little even at high temperatures, so parents may not notice the onset of the disease. Secondly, he may touch tubes and medical devices with his hands, run or move awkwardly, disrupting the operation of equipment and disturbing personnel. Thirdly, children take death lightly, but the shock of what they see in the hospital will disrupt the child’s psychological comfort for a long time.
When performing medical manipulations and procedures, relatives are also not needed, it is unpleasant for them to see it, and the staff feels psychological pressure.
The presence of several relatives in the intensive care unit is excessive; one or two close people for a short time is quite enough to maintain the spirit of a cancer patient; do not forget that it is hard for him, he gets tired very quickly. Sitting all night long is not good for anyone, healthy people are exhausted, and the patient is simply not aware of round-the-clock vigil at the bedside.
How should a relative behave in intensive care?
- You must be in clean clothes, a medical gown, clean hands, shoe covers on your feet, and a mask on your face.
- Perfume odors are irritating, since in a serious condition the sense of smell changes; you should not perfume yourself on this day.
- Phone beeps must be turned off, or better yet, all gadgets must be turned off. Maintaining silence is mandatory; loud sounds disturb staff and cause stress in patients.
- Without the permission of the staff, you cannot perform any actions with the patient: turn over, sit up, put on your feet, take you to the toilet, change clothes, and so on.
- You cannot feed - the patient receives a specific and, as a rule, very strict diet or is generally on intravenous nutrition.
- You should not give medications, homemade decoctions, pharmacy tinctures, dietary supplements and nutritional supplements previously prescribed for chronic diseases. Biological supplements may not be compatible with the medications the patient is receiving. Everything must be agreed with the attending physician.
A sick person and a patient in the intensive care unit are two very different things; some cannot recognize their loved one, his appearance changes so much. Not only because of the tubes and wires, but the tissues swell, the eyes become sunken, and the unconscious state changes facial features. Many are shocked by what they see; one must be prepared for an unpleasant experience or not enter the intensive care unit.
In the Euroonko intensive care unit they always help patients and support the spirit of relatives. We know what needs to be done and when, you can be confident in us. We do not guarantee immortality, but we help to live without suffering.
Book a consultation 24 hours a day
+7+7+78
Bibliography
- Clinical recommendations. Anesthesiology and resuscitation / ed. Zabolotskikh I.B., Shifmana E.M. - M.: GEOTAR-Media, 2016.
- Moroz V.V., Bobrinskaya I.G., Vasiliev V.Yu. and others/Cardiopulmonary resuscitation// M.: FNKTs RR, MGMSU, NIIOR, 2017.
- Order of the Ministry of Health of the Russian Federation dated November 15, 2012 N 915n “On approval of the Procedure for providing medical care to the population in the field of oncology”
- Order of the Ministry of Health of the Russian Federation dated July 4, 2017 No. 379n “On amendments to the Procedure for providing medical care to the population in the field of oncology, approved by order of the Ministry of Health of the Russian Federation dated November 15, 2012 No. 915n”