General information
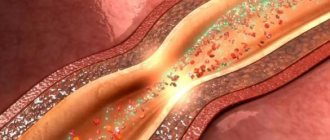
Vascular spasm (syn. angiospasm) is a pathological transient narrowing of the lumen of large/small arteries and capillaries due to prolonged intense/excessive contraction of the muscles of the vascular wall, causing disturbances in blood circulation/tissue metabolism.
Angiospasm can be considered as a variant of vascular crisis (acute vascular dystonia). Normally, due to their elasticity, blood vessels ensure uninterrupted and adequate blood flow to various organs, which ensures their functioning. With vascular spasm of varying degrees/localization, the parameters of local/systemic hemodynamics are correspondingly disrupted.
Maintaining vascular tone is carried out due to the tension of the vascular muscle layer, and the contractile activity of the muscle layer is directly regulated by nerve impulses from the brain arriving through sympathetic nerve fibers. It is the myogenic reactions of blood vessels that support circulatory homeostasis . In addition to muscle regulation of tone, its maintenance is carried out due to metabolic, humoral-hormonal and neurogenic mechanisms of vascular regulation.
Developing arterial insufficiency due to spasm of the arterial network leads to tissue ischemia in the area of the spasmodic artery and the development of hypoxia of various organs and tissues, which is manifested by disturbances in their functions. Previously, vasospasm was classified as a disease of “old age,” but currently there is a clear trend towards rejuvenation of vascular disorders. The reason is the high pace of life with frequent stress and unfavorable environmental conditions. The consequence of vasospasm is ischemia .
Angiospasms can occur in different vascular regions, mainly in diseases characterized by damage to the arteries/nervous apparatus ( aneurysms , atherosclerosis , vasculitis , etc.) or disorders of the neurohumoral regulation of vascular tone ( neuroses , hypertension , pathological menopause , hypothalamic syndrome , etc. .). Angiospasm often shapes the dynamics of clinical symptoms in organic vascular diseases, such as thrombosis , atherosclerosis , embolism, etc.), significantly complicating their course. Prolonged chronic or acute arterial insufficiency in the heart (coronary vasospasm), brain (cerebral vasospasm), and in the retina (retinal vasospasm) can cause the development of acute vascular insufficiency. As a rule, acute arterial obstruction is the cause of such serious conditions as myocardial infarction , stroke , and visual impairment.
Vascular stenosis develops in most cases with atherosclerotic damage to the arteries, which is caused by the deposition of cholesterol plaques on the walls. Chronic arterial insufficiency of the lower extremities is also widespread. What are the types of vascular diseases in the legs? In the lower extremities, so-called “occlusive vascular diseases” are quite common, provoked by narrowing/clogging of the iliac arteries/abdominal aorta as a result of the deposition of atherosclerotic plaques on their walls, which significantly impairs the blood flow of the lower extremities. These are obliterating diseases of the peripheral arteries of the legs ( atherosclerosis obliterans , thromboangiitis obliterans , endarteritis obliterans , diabetic angiopathy ), characterized by a steadily progressive course with the transition of increasing intermittent claudication to a constant pain syndrome. Critical leg ischemia leading to gangrene is an extremely severe outcome of long-term arterial insufficiency.
Pathogenesis
The pathogenesis of vasospasm has not yet been fully studied, which is largely due to its non-identity for arteries of different vascular regions. It is generally accepted that a common factor in the mechanism of development of vasospasm includes functional disorders of the membranes of smooth muscle cells of the vessel, the essence of which is a violation of the exchange of potassium, calcium, and sodium ions through the membranes, which disrupts the alternation of muscle contraction/relaxation phases. Enhanced/accelerated depolarization of membranes, as well as an increased influx of free calcium ions into cells, contribute to intense muscle contraction, and a delay in membrane repolarization (preceding muscle relaxation) contributes to prolonged contraction of the arterial wall.
Disturbances of this kind may be caused by disturbances in the innervation of vascular walls, an imbalance in the production/destruction of humoral regulators of tone, increased sensitivity of vascular wall receptors to the effects of vasoconstrictors, and a disorder of humoral regulators of vascular tone. Often, stenosis can develop against the background of local changes in the vessel wall in areas of thrombus , vascular inflammation, scars (for example, near the area of coronary artery thrombosis/location of an aneurysm or atherosclerotic plaque).
Vascular headache
It is important to understand that the term “vascular headache” is not an official designation for any disease. However, patients often hear from their doctors about “vascular” pain.
In our country, “vascular pain” refers to vegetative dystonia, migraine, headache due to high blood pressure and impaired venous outflow. At the same time, “vegetative dystonia” in itself is also not a correct diagnosis, but in practice this diagnosis is made and various neurological problems are blamed on it.
The bad thing is that, using such a general term, the doctor himself often does not delve into the details. As a result, an inaccurate diagnosis leads to the choice of incorrect treatment.
Primary and secondary pain
Although the diagnosis “vascular headaches” is not entirely correct, no one disputes that blood vessels are often involved in the development of headaches. However, a violation of vascular tone or damage is NEVER the only cause of a headache, but only one of the stages in the development of a painful episode! The appearance of pain is always the result of a complex cascade of reactions from all body systems (cardiovascular, endocrine, nervous and others).
Causes
The causes of vascular spasms have not been sufficiently studied, however, a number of diseases can be identified that are accompanied by vasospasm in different vascular regions:
- Atherosclerosis at the stage of pronounced atherosclerotic changes in the vascular bed.
- Osteochondrosis of the spine in the cervical region.
- Hormonal disorders in diseases of the endocrine system ( diabetes mellitus ).
- Diseases of the cardiovascular system ( hypertension , atrial fibrillation ).
- Dysfunction of the autonomic nervous system.
- Traumatic brain injuries.
- Frostbite.
- Stress and overwork.
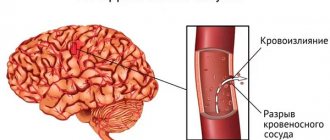
- Brain hemorrhages.
- Vasculitis is inflammation of the artery (vascular walls).
- Brain tumors.
- Chronic intoxication (poisoning with lead/carbon disulfide compounds).
The most common/significant risk factors for the development of vasospasm are: arterial hypertension , smoking, alcohol abuse, male gender, old age, dyslipidemia , physical inactivity and excess body weight. Among them, the greatest importance is given to disorders of fat metabolism and arterial hypertension.
Obviously, the causes of vasospasm in different vascular regions differ, that is, the causes of spasms of cerebral vessels and the causes of vasospasm of the retina or lower extremities are different.
Clinical manifestations of vasospasm
It must be remembered that cerebral vasospasm is a kind of circulatory disorder, and since the brain is associated with the regulation of neuropsychological processes, the main clinical manifestations are associated with a violation of neurological and psychological functions. To describe the symptoms of cerebral vasospasms, it is convenient to identify two groups: neurological and psychological lesions.
I. Neurological lesions in cerebral vasospasms.
- Headache, migraine. One of the early symptoms of vasospasm.
- Dizziness. As a rule, they arise spontaneously. They can occur together with loss of orientation in space.
- Feeling sick or suddenly vomiting.
- Visual, auditory, taste or olfactory disturbances, including hallucinations.
- Sometimes patients experience pain in various parts of the body (although the connection with cerebral vasospasm has not been established).
- Decreased performance.
- Increased fatigue.
II. Psychological disorders:
- The main and most alarming signs are memory impairment and amnestic syndrome.
- Various types of preservation (multiple repetitions of words or actions).
- Violations of psychological orientation. Patients are not able to talk about themselves, their profession, etc. This state is sometimes accompanied by apathy and indifference to the environment.
Symptoms
Symptoms of vascular spasm are determined by its localization and are manifested by manifestations of dysfunction of ischemic tissue of various organs. Let's look at just a few of them:
Symptoms of vascular disease in the legs (using the example of obliterating atherosclerosis ). Depending on the severity of insufficiency of arterial blood supply to the limb, several stages of clinical manifestations of the disease are distinguished:
- Stage of functional compensation . At this stage, cramps, chilliness and paresthesia of the lower extremities are characteristic, and less often - burning/tingling in the fingertips, leg fatigue, and increased fatigue. As the skin cools, it becomes pale and cold to the touch. As a rule, when walking on level ground after 1000 meters or more, intermittent claudication appears due to insufficient blood supply to the muscles, accumulation of under-oxidized metabolic products in tissues and disruption of the process of oxygen utilization.
- Subcompensation stage . There is an increase in the intensity of intermittent claudication, which already occurs after traveling a distance of about 200 m. The skin of the legs/feet becomes dry, loses elasticity and flakes, and hyperkeratosis . Characterized by a slowdown in hair growth (patches of baldness appear) and nails, which become dull, brittle, thickened and acquire a matte color. Initial signs of atrophy of the foot muscles and subcutaneous fat are noted.
- Stage of decompensation . Against the background of ongoing spasm of the vessels of the legs of the affected limb, pain appears at rest, and walking is possible at a distance not exceeding 25 meters. Progressive atrophy of the leg/foot muscles is noted, the color of the skin of the legs changes, and the skin turns pale when the limb is raised and redness appears when it is lowered. The skin becomes easily vulnerable and various types of minor injuries (abrasions/ bruises ) lead to the formation of non-healing chronic wounds , cracks , and painful superficial ulcers . The patient has limited ability to work. With severe pain syndrome, disturbances in night sleep are observed, patients take a forced position - the “doll” pose.
- Stage of destructive changes . At this stage, vasospasm of the lower extremities causes the development of necrobiotic processes. And the rate of their increase is determined by the level of the gap between the amount of blood flow to the tissues and their need for oxygen. The pain in the fingers and feet is extremely intense. The resulting ulcers are located mainly in the distal parts of the legs (usually on the fingers). The bottom/edges of the ulcers are covered with a gray-dirty coating without granulation, and there is inflammatory infiltration around them. Swelling of the foot/leg develops. Characteristic is the development of wet gangrene of the fingers and feet. The ability to work at this stage is completely lost.
Symptoms of cerebral vascular spasms
Angiospasm of cerebral vessels, contributing to the development of chronic circulatory failure of brain structures (dyscirculatory encephalopathy) can develop with damage to the main arteries (stenosis of the vertebral/carotid arteries), narrowing/thickening of intracerebral arteries against the background of arterial hypertension and due to narrowing of the lumen due to thickening of the walls of small arteries.
There are several stages of development of dyscirculatory encephalopathy. The initial symptoms of the disease may be latent for some time. At this stage, the disease manifests itself with complaints of noise in the head, headaches , dizziness , and decreased non-professional memory and performance. Patients may be tearful, distracted, irritable, and depressed. They experience difficulty transitioning from one type of activity to another.
At the next stage, non-professional/professional memory impairments progress, a narrowing of the range of interests, a decrease in intelligence, and fixation on a specific problem are noted. The patients are quarrelsome, and personality changes are increasing. Such patients sleep poorly at night and are drowsy during the day. Neurological symptoms increase, spasms in the head are noted, movements slow down and their coordination is impaired, staggering when walking/mild speech impairment is characteristic, and performance is significantly reduced.
Subsequently, against the background of ischemia, gross changes in the tissue of certain brain structures occur, which intensifies the manifestations of neurological symptoms, and mental disorders develop. Patients stop recognizing loved ones, can get lost while walking, perform inappropriate actions and almost completely lose their ability to work.
Angiospasm of the retina
Bilateral retinal vasospasm is typical, less often a unilateral process is noted. Patients complain of the appearance of “fog” before the eyes and the flickering of “floaters”. With a short-term spasm, blurred vision is possible, but it is transient. Distortion of visual perception in the form of meta/photomorphopsia is possible. In some cases, a feeling of discomfort appears in the orbital area; patients may feel pulsation in the temples, headache and dizziness . After the attack is over, the patient’s condition returns to normal and visual function is restored. In severe cases (acute obstruction of the central retinal artery) can lead to a pronounced/irreversible decrease in visual acuity.
Alcoholic epilepsy
This type of epilepsy develops in patients who abuse alcohol. Seizures occur due to irreversible pathological processes in the cerebral cortex. Epilepsy attacks caused by alcohol intoxication most often occur in patients suffering from the following concomitant diseases:
- Atherosclerosis;
- Consequences of traumatic brain injury;
- Brain tumors;
- Residual effects of previously suffered infectious and inflammatory diseases of the brain.
The cause of the disease may be aggravated heredity. The symptoms of alcoholic epilepsy have some peculiarities. The disease does not necessarily begin with a convulsive syndrome. Initially, the following pathological signs appear:
- Increased salivation;
- Marked weakness throughout the body;
- Paleness of the skin;
- Blueness of lips;
- Dizziness;
- Strong headache;
- Loss of consciousness;
- Nausea, vomiting;
- Uncontrolled urination;
- A spasm of the vocal cords that causes a person to emit a high-pitched scream.
An attack of alcoholic epilepsy can result in respiratory arrest and death.
Tests and diagnostics
The diagnosis of “angiospasm” is based on the presence of characteristic symptoms of vasospasm and their dynamics, characteristic of the development of transient ischemia in the area of the spasmodic artery. To establish a diagnosis, the following is carried out:
- Ultrasound of leg vessels (Doppler/duplex scanning).
- CT angiography (with contrast agent) of cerebral vessels, which allows you to clearly determine the diameter of the lumen of the vessels and visualize the places of narrowing.
- Dopplerography of cerebral vessels (to assess the speed of blood flow in the intracranial arteries in various areas).
- MRI of the brain/cervical spine.
- Doppler ultrasound of the brachiocephalic arteries.
- Fundus ophthalmoscopy.
- Functional tests (Goldflam/thermometric, etc.).
Laboratory methods include biochemical blood tests, determination of blood cholesterol levels, and coagulogram. In the presence of cognitive impairment - neuropsychological testing.
Diagnosis of cerebral vasospasm
The diagnosis is made by a specialist based on symptoms, as well as instrumental and hardware research methods. When diagnosing cerebral vascular spasm, the most informative methods are:
- MRI (magnetic resonance imaging) of the head and neck;
- Contrast magnetic resonance imaging of blood vessels (angiography). This method uses the introduction of special contrast agents into the bloodstream.
Can also be used:
- magnetic resonance imaging
- Doppler examination using ultrasound (less informative research method).
Prevention
Prevention of vascular diseases, including vasospasm, consists of maintaining a healthy lifestyle, including:
- Balanced diet.
- Active lifestyle.
- Stop smoking.
- Body weight control.
- Monitoring blood pressure , cholesterol /sugar levels.
- Periodic medical examinations.
The basis for the prevention of thrombosis and vascular diseases is the strengthening of blood vessels, which is achieved by regular practice of procedures such as contrast showers/douches, contrast foot baths, bath procedures, lymphatic drainage massage, pine/turpentine baths.
Angiospasm of leg vessels
Angiospasm can be observed in all kinds of vascular regions and is accompanied by damage to blood vessels and the nervous system. People who are addicted to smoking are most often susceptible to vasospasm in the legs. The disease also occurs as a result of frostbite and hypothermia. The disease is diagnosed based on the dynamics of symptoms, including changes in skin color and a decrease in its temperature.
Consequences and complications
The consequences of vasospasm are determined by the duration/severity of ischemia in the area of the spasmodic artery, the sensitivity of tissues/organs to oxygen deficiency, as well as the development of collateral circulation in the affected organ. The brain and heart muscle, kidneys, and spleen are especially sensitive to hypoxia. Accordingly, ischemia of these organs is accompanied by a high risk of developing ischemic stroke and myocardial infarction . Prolonged vasospasm of the arteries of the lower extremities can cause the development of obliterating diseases ( atherosclerosis obliterans , thromboangiitis obliterans , endarteritis obliterans , diabetic angiopathy ), retinal vasospasm - visual disorders, and so on.
List of sources
- Krylov V.V., Gusev S.A., Titova G.P., Gusev A.C. Vascular spasm in subarachnoid hemorrhage. M.: Medicine; 2000.
- Avksentyeva M.V., Krysanov I.S., Chupin A.V. Pharmacoeconomic aspects of the treatment of obliterating diseases of the peripheral arteries of the lower extremities // Angiology and Vascular Surgery. 2012. T. 18, No. 4. P. 16-21.
- Drozhzhin E.V., Darwin V.V. The role of rheological disorders in the pathogenesis of the obliterating process in the arterial system // Collection of scientific papers of Surgut State University. Vol. 12. Natural sciences. Surgut: Surgut State University Publishing House, 2003. pp. 67-69.
- Zudin A.M., Zasorina M.A., Orlova M.A. Epidemiological aspects of chronic critical ischemia of the lower extremities // Surgery. 2014. No. 10. P. 78-82.
- Savelyev V.S., Koshkin V.M. Critical ischemia of the lower extremities. M.: Medicine, 1997. - 160 p.