08 October 2021
Alzheimer's disease is the most common type of dementia, a condition in which the brain no longer functions properly.
Alzheimer's disease is the most common type of dementia, a condition in which the brain no longer functions properly. The disease was first described in 1907 by the German psychiatrist Alois Alzheimer. Typically, it is found in people over 65, but there is also early-onset Alzheimer's disease, a rare form of the disease. Due to the disease, memory and mental abilities gradually deteriorate, and the ability to cope with daily activities decreases.
Some sources report that the number of people around the world suffering from Alzheimer's disease is estimated at about 30 million people; in others - over 50 million. It has been reliably established that women get sick more often, the frequency of occurrence is constantly growing: over the next decades, the number of sick people should increase by 3-5 times.
There are many forms of dementia. Alzheimer's disease is the most common form, accounting for 60-70% of all cases. Other common forms include vascular dementia, dementia with Lewy bodies (abnormal protein inclusions that form inside nerve cells), and a group of diseases that contribute to the development of frontotemporal dementia (degeneration of the frontal lobe of the brain). There are no clear boundaries between different forms of dementia, and mixed forms of dementia often coexist.
Predementia
The first stage of the disease, which is characterized by primary cognitive disorders. Typically, the patient’s most pronounced symptom is a deterioration in memory, namely short-term memory (it becomes increasingly difficult to remember information that was only recently memorized). This stage occurs 8-10 years before diagnosis. These symptoms are often confused with stress or the aging process.
- Services Prices
- Consultation with a psychiatrist-gerontologist 5000 rubles
- Calling a psychiatrist to your home for an elderly person 12,000 - 15,000 rubles
- Certificate of incapacity of an elderly person 5,000 rubles
- Initial consultation with a psychiatrist 5000 rubles
- Appointment with a psychiatrist, candidate of medical sciences, with 30 years of experience (50-60 min) 6,000 rubles
- Urgent call of a psychiatrist to your home (within the Moscow Ring Road) 12,000 - 15,000 rubles
- Psychiatric examination before the transaction (in the center) 5,000 rubles
- On-site psychiatric examination (60 min) 12,000 - 15,000 rubles
- Certificate of legal capacity when selling an apartment 5,000 rubles
- Conclusion on mental health 5000 rubles
Request a call back Make an appointment
Early dementia
This stage of diagnosis, as there is a further deterioration in the general condition of the patient: the symptoms are becoming more pronounced. In addition to short-term memory impairment, speech impairment, motor impairment, and the first symptoms of long-term memory impairment appear. Disorders of long-term memory manifest themselves individually in everyone, ranging from the inability to remember information that the patient memorized several years ago, ending with memories of the correct use of cutlery. There is a violation of the speech apparatus, however, it is hardly noticeable.
Moderate dementia
Memory problems only get worse, to the point of being unable to recognize your relatives. Manifestations of speech impairment become noticeably more noticeable - as the disease progresses, a decrease in vocabulary occurs; Often the patient begins to select the wrong words to replace the forgotten ones. Loss of motor coordination occurs, and it becomes increasingly difficult to perform everyday tasks. There is a loss of reading and writing skills, disturbances in the patient’s psycho-emotional state, outbursts of aggression and spontaneous crying.
Symptoms of dementia in Alzheimer's disease
Depending on the severity of symptoms, there are 4 stages of Alzheimer's disease.
- At the first stage, short-term memory impairments begin to appear. This is reflected in periodic loss of things and difficulties in remembering new information. Some people may have trouble finding words when speaking. But in general, these changes are typical for older people, so no one pays attention to them.
- At the stage of early dementia, the state of memory begins to deteriorate, and these changes can no longer be attributed to senile forgetfulness or absent-mindedness. It becomes more difficult for the patient to cope with daily activities, he may forget to pay bills or turn off the gas. Other symptoms also appear. In particular, coordination of movements, especially fine motor skills, is impaired. There may be disturbances in gait, and patients may get caught on a carpet or threshold and fall. Mental changes occur. Grouchiness and quarrelsomeness appear, the person gets irritated by every little thing.
In addition, delusions may occur, such as delusions of damage or harm. They may claim that relatives, neighbors or social workers are trying to rob, poison, or kill them in order to take possession of property or real estate. Other manifestations may also occur - a tendency to wander, overeating or, conversely, refusal to eat. Meaningless repetitive actions are also typical, for example, constantly moving objects from place to place, meaningless walking around the room. Speech also continues to be impaired. It becomes impoverished, phrases are primitive, and some words can be replaced with inappropriate ones. At this stage, many things can be done independently, but periodic supervision and assistance from others are required.
- At the third stage, the patient's condition worsens even more. Memory is impaired to such an extent that patients do not recognize relatives and loved ones. False memories arise. Patients have very poor spatial orientation and can become confused in their own apartment. Motor functions are greatly impaired, which makes it difficult for such people to carry out everyday activities, for example, dressing, washing, and preparing food. At the same time, they seem to forget how to correctly perform this or that action. For example, when they try to sit on a chair, they freeze over it because they don’t know what to do next. At this stage, patients need round-the-clock care.
- At the terminal stage, a pronounced disintegration of personality occurs. Speech is almost completely lost, only individual words or sounds remain. Verbal contact is almost impossible. Movement disorders are very pronounced, to the point that patients cannot move around the house independently and become bedridden. Eating skills such as chewing and swallowing may be lost. In this condition, patients need round-the-clock specialized care.
Causes
The exact causes of the disease are not known. Previously, it was thought that the main cause was a disruption in the production or massive destruction of the neurotransmitter acetylcholine. However, drugs based on it did not cure the patient. The following possible reasons are currently identified:
- Genetic predisposition;
- Heavy metal poisoning;
- Head injuries;
- Hypothyroidism;
- Malignant and benign neoplasms;
- Concomitant genetic diseases (Down syndrome);
- Age.
Causes
There are many theories about the occurrence of Alzheimer's disease, but the exact cause has not been established.
The exact cause is still not determined.
Lack of acetylcholine. It was thought that the disease might be related to a deficiency of this neurotransmitter. But it turned out that the administration of this substance does not improve the condition of patients.
Amyloid theory. Amyloid protein is deposited in brain tissue and is detected on CT/MRI in the form of plaques. First, the transmission of nerve impulses is disrupted, then the brain cells die. It can take 10-15 years from the appearance of the first plaques to mild forgetfulness3.
Tau theory. Structural abnormalities occur in the structure of tau protein, which is contained in nerve cells. This disrupts the transmission of nerve impulses, and ultimately leads to the death of the neuron. These disorders are usually detected after the onset of amyloid plaques.
Genetic predisposition becomes the cause in only 10% of cases1.
Risk group
Patients who have certain diseases are automatically included in the risk group. These diseases can be grouped together according to one very important symptom - lack of oxygen in brain cells:
It is also worth mentioning separately about the disturbance of protein metabolism, or more precisely about the production of a pathological protein - amyloid. It can be deposited in the brain in the form of plaques and leads to neuronal degeneration and impaired blood supply. A distinctive feature of this protein is that the body is unable to dissolve it or get rid of it on its own. This protein begins to be deposited long before the first symptoms of the disease appear.
Stages of the disease
Alzheimer's disease develops gradually, not all at once.
"Doubtful" dementia
The early stage may not be noticeable to others and can only be revealed through detailed neurocognitive tests. This stage is characterized by mild forgetfulness and inaccurate memories. You can also notice difficulties in determining the similarities and differences between objects and events. Abstract thinking and planning are difficult. In ordinary life, we won’t even notice this, so a person manages to hide or compensate for small problems in communication and work.
Mild dementia
Memory impairments become more obvious, especially for recent events. A person can get lost and forget his usual route. Confuse the order of events. Cannot find commonality or compare two objects or events. The ability to do calculations and write letters is lost. Such a person will speak slowly, use simple words, sometimes they may not be enough for reasoning. At the same time, the usual self-care activities are preserved.
Changes in behavior are already possible in the form of petty nonsense that someone is stealing from him, oppressing him, or causing harm. The state may be depressed due to the understanding that “something is wrong” with the head.
Moderate dementia
At this stage, learning new information becomes impossible. A person gets confused in the order of important events in his own life. He ceases to understand where he is and what time it is. The stock of memory and knowledge is constantly decreasing, they are becoming more and more inaccurate and blurred. Speech is impaired, first the ability to write is lost, then to read.
A “time shift” into the past may occur in consciousness. A person thinks and perceives everything as if he were not living today, but in a time that he still remembers. This may be accompanied by energy and a persistent desire for pseudo-activity.
Severe dementia
A person completely loses touch with reality, he not only does not orient himself in time and space, but also loses the idea of himself, his personality. Such a person cannot live independently. Attention is very weak. Reactions are more template, “automatic”. At the same time, emotional contact is preserved; an example would be “imaginary” conversations, when the patient tries to maintain a conversation, but its content is completely meaningless. The mood can change from aggression to apathy.
The patient is weakened psychologically and physically. Activity decreases sharply, complications develop in the form of bedsores, pneumonia, which leads to death.
Symptoms
Each stage is characterized by certain symptoms. The early stage is characterized by:
The late stage is characterized by:
These are common symptoms that in most cases appear in all patients. However, we must remember that individual symptoms are also possible. For example: repetition of phrases, fear and anxiety when faced with difficulties.
Attention! We must remember that all these symptoms and the patient’s future lifestyle will lead to a decrease in immunity, which means complications such as:
It is very important to consult a doctor when the first symptoms of the disease appear. It is also important to undergo preventive medical examinations for early detection of the disease.
Diagnostics
It is very difficult to recognize the disease, since when diagnosing one has to rely on symptoms and complaints - in the early stages it is very difficult to differentiate the disease from stress or from the processes of physiological aging. And in most cases, the patient does not immediately turn to a specialist, since the symptoms may not bother him much. In the later stages, the diagnosis is easier to make – the characteristic symptoms become more pronounced. But it is worth remembering that other diseases can manifest themselves similarly:
- Stroke;
- Parkinson's disease;
- Atherosclerosis of cerebral vessels;
- Neoplasms of the brain.
For correct diagnosis, it is very important for the doctor to collect a complete medical history of the patient:
- When did the first symptoms appear?
- What symptoms does the patient have?
- How severe are the symptoms?
- Accompanying illnesses;
- Presence of injuries.
Due to the nature of the course of the disease, the patient cannot always independently answer all the doctor’s questions, so making a diagnosis can be difficult. If possible, all the necessary information is provided to the doctor by knowledgeable relatives of the patient.
Diagnosis also includes neuropsychological tests, which help assess the severity of cognitive impairment, and PET scans, which are used to detect amyloid accumulations in the brain.
Differential diagnosis
To carry out differential diagnosis, a biochemical study of the patient’s blood is performed to exclude all possible inflammatory diseases. In the early stages of the disease, you can perform a CT or MRI to exclude the possibility of tumors in the brain and stroke, and angiography to look at the patency of blood vessels and the presence of atherosclerosis. Psychological tests are used to identify specific organic thinking disorders and to determine concomitant depression, anxiety, and other symptoms that may aggravate the course of dementia.
At later stages, CT and MRI will show significant brain atrophy in characteristic areas. It is also advisable to conduct a chemical analysis of the cerebrospinal fluid to detect pathological or disease-specific cellular elements in it. Genetic analysis will determine predisposition to this disease, as well as detect mutations characteristic of Alzheimer's disease.
Alzheimer's disease: causes, diagnosis, treatment
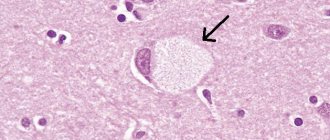
Alzheimer's disease is a form of dementia or dementia that cannot be reversed. The disease is accompanied by progressive memory loss, decreased intellectual abilities, and deterioration of language and speech skills. All these symptoms together lead to a change in a person’s behavior and a decrease in the quality of his life, resulting in complete social maladjustment. In Alzheimer's disease, damage to brain tissue is primary. The pathological process is associated with the accumulation of amyloid protein in the interstitial substance of the brain and the formation of senile plaques, tau protein in the cells of the nervous tissue and the formation of typical structures called neurofibrillary tangles. The formation of pathological structures leads to damage and death of nerve cells, a decrease in the level of neurotransmitters, and a deterioration in interaction between parts of the brain.
Alzheimer's disease begins with minor memory problems as the temporal lobes of the cerebral cortex are the first to be affected. A person forgets where he put the thing, what this cutlery is for, what he went to the store for, what time he should come to work, etc. A person may not remember his date of birth, his residential address, the names of his own children, and may get lost in simple questions, for example, what day is it today, what time is it, where and who does he work for. Later, speech disturbances appear, the patient cannot remember the right word, orientation disorders are observed, and the person cannot find his way home.
Stages of the disease
There are three stages in the course of Alzheimer's disease. At the first stage, the patient can take care of himself independently; at the second stage, he cannot do without the help of loved ones. A person cannot dress himself, take a shower, wash dishes, etc. During the third stage, dependence on the presence of a loved one becomes total: the patient cannot perform a single daily activity without outside help.
Disease and age
The risk of Alzheimer's disease and other forms of dementia increases significantly with age. Isolated cases of the disease are observed after 40 years of age; in people over 65 years of age, the disease is detected in 10–12% of cases; in people over 85 years of age, in 30–40% of cases.
There are early and late onset Alzheimer's disease. Early onset manifests itself before the age of 65 and is characterized by rapid progression. A number of assumptions have been made about the genetic component of the disease. “Late onset” Alzheimer's disease appears after 65 years of age, is not considered inherited, and its course is smoother.
Genetic predisposition
Alzheimer's disease is caused by many factors that are not yet well understood. Three genes have been identified whose mutations are associated with rare early familial forms of the disease. They account for 5% of all cases. The PSEN1, PSEN2 and AP genes, located on chromosomes 14, 1 and 21, are responsible for the synthesis of abnormal protein structures, which are the pathomorphological substrate of Alzheimer's disease. There is a 50% chance that the gene mutation will be passed on to each of the children of a carrier of the pathological gene.
Other genes have been linked to late-onset Alzheimer's disease. They are not considered to be the direct cause of the disease process, although they may explain why there is an increased risk of developing late onset in individuals with a family history of the disease. The APOE gene is one of them. The APOE gene is responsible for the production of apolipoprotein E, a protein that transports lipids (fats and cholesterol) in the blood. The APOE gene exists in three different forms (alleles): E2, E3 and E4. Each person inherits two APOE alleles, which are a combination of these three. E3 is the most common allele in the population, found in 60% of the general population. The presence of the E4 APOE allele is associated with the majority of familial cases and an increased risk of developing Alzheimer's disease, and is therefore considered a prognostically unfavorable combination.
Risk factors
Along with genetic factors, there are other risk factors for Alzheimer's disease. These include type 2 diabetes and milder forms of insulin resistance, obesity, high blood pressure, dyslipidemia, and high levels of inflammatory markers such as C-reactive protein (CRP).
Diagnostics
An accurate clinical diagnosis of Alzheimer's disease is made based on the clinical picture, using various tests and procedures to rule out other causes of dementia. The doctor evaluates the person's personal and family medical history and administers neuropsychological tests to measure memory, language skills and other cognitive functions.
Imaging tools such as computed tomography (CT) and magnetic resonance imaging (MRI) are often used to look for signs of injury, tumors and stroke, as well as atrophic changes in the brain seen as the disease progresses.
Unfortunately, there are no laboratory tests to diagnose Alzheimer's disease during life. The only accurate tool to confirm the presence of the disease is a histological examination of a section of the brain after death. Pathologists describe senile plaques and neurofibrillary tangles characteristic of Alzheimer's disease. Since the formation of plaques and tangles is also observed during normal aging, the sample is compared with a control sample of normal brain tissue from a person of the same age who does not have the disease.
In 2011, new criteria and recommendations for diagnosing Alzheimer's disease were developed. Preclinical, subclinical and clinical stages of the disease have been identified, and new criteria for dementia syndrome in Alzheimer's disease have been developed.
The preclinical stage of Alzheimer's disease is characterized by the absence of cognitive impairment, but amyloid bodies can be detected in the brain. The appearance of biomarkers in neuroimaging is a harbinger of dementia 10–15 years before its manifestation. This stage is highlighted to help guide research towards early diagnosis of the condition.
Mild cognitive impairment due to Alzheimer's disease is the presence of mild changes in memory and thinking ability that do not interfere with daily activities.
Dementia due to Alzheimer's disease. Memory, thinking, and behavioral symptoms that interfere with a person's ability to function in daily life.
The recommendations are intended to provide more information about the current understanding of Alzheimer's disease and provide a basis for future research.
Treatment
Drug therapy includes a group of cholinesterase inhibitors and antiglutamatergic drugs. Non-drug therapy is aimed at improving cognitive functions and the formation of neural connections: aerobic physical activity, maintaining an active social life, and performing cognitive training.
Drug treatment
All drugs prescribed by doctors are aimed at relieving the symptoms of the disease:
- The use of antioxidants improves blood supply to the brain, hemodynamics and reduces cholesterol levels (preventing the development of atherosclerosis);
- Prescribe drugs that improve thought processes and memory;
- Antidepressants are introduced into the course of treatment to maintain psycho-emotional balance;
- Cholinesterase inhibitors reduce the rate of destruction of neurotransmitters, and thereby increase their concentration in the brain;
- Antipsychotics help reduce aggression and stop psychosis (however, according to statistics, long-term use of these drugs increases mortality);
- Beta-secretase inhibitors – reduce amyloid synthesis and the creation of amyloid plaques.
Treatment
Unfortunately, there is no cure for Alzheimer's disease or slow the progression of the disease, but medications can help relieve symptoms. To correct cognitive impairment, drugs from the group of cholinesterase inhibitors (physostigmine, galantamine, proserine) and memantine are prescribed. Antipsychotics are used for aggression, psychosis and behavior problems, although their long-term use in dementia increases the mortality rate.
A very important aspect of the rehabilitation of patients with Alzheimer’s disease is psychosocial support, training relatives in behavioral tactics and care skills. A sick person should not feel like a heavy burden or disabled. Art therapy, hippotherapy, music therapy, etc. can be used as an auxiliary treatment.
Psycho-emotional intervention
Used as an additional method. The general condition does not improve, however, individual problems such as incontinence may be alleviated. This therapy helps patients adapt to the disease. In the early stages, memory therapy is carried out: patients discuss the events they have experienced, using photographs, objects, favorite music, videos and other well-known objects. However, this method affects the patient individually. The method of simulating presence is based on attachment theory: audio and video recordings with the voices of family and friends are used. In patients undergoing this therapy, feelings of anxiety decrease and behavior becomes calmer. Stimulating methods include music therapy, art therapy, communication with animals, and physical exercise, which have a positive effect on behavior and mood.
Alzheimer's treatment
Experts believe that about half of the world's dementia cases are associated with known lifestyle risk factors, such as smoking, physical inactivity, unhealthy diet, obesity, diabetes, hypertension and alcohol consumption.
There are also methods of effective therapy; they cannot always stop the progression of the disease, but they reduce the severity of symptoms, have a beneficial effect on behavior, and reduce the need for outside help and care. Treatment is most effective in the early stages of the disease. For Alzheimer's disease, medications are prescribed that block cholinesterase and prevent the formation of amyloid and plaques. These are donepezil, rivastigmine and galantamine; it should be remembered that only a doctor can prescribe medications, taking into account the symptoms of each patient.
Psychosocial therapy complements drug treatment. It allows patients in the early stages of Alzheimer's disease to adapt to the disease. Working with memories, communication, and performing intellectual tasks stimulate brain function and have a positive effect on the patient’s psycho-emotional state. Such work is possible both individually with each patient and in groups.
Back to articles
Patient care
Relatives have the hardest time. It is important to realize that a loved one is becoming more and more helpless and to understand that the patient’s behavior is provoked by an illness. The key to success is patience with the patient. It is necessary to create safety, proper nutrition, prevent bedsores and maintain immunity, and try to provide complete protection from stressful situations. Doctors recommend making an appointment with a psychologist, since in the life of a person caring for a patient, as a rule, psycho-emotional disorders, depression, and social and economic problems arise. As the disease progresses, the patient will experience various complications, such as diseases of the teeth and oral cavity, impaired ability to feed independently (later problems with swallowing food), respiratory diseases, eye and skin infections, etc. It is imperative to monitor the general somatic condition of the patient and at the first manifestation of problems, urgently look for solutions. Monitor the patient’s hygiene independently, including brushing teeth after each meal. Grind the food or turn it into a mushy state (if necessary, feeding is done through a tube). If necessary, restrain the patient to prevent harm to themselves or others.
Prevention of Alzheimer's disease
Unfortunately, since this is a progressive and incurable disease, prevention is ineffective and is aimed at increasing immunity and reducing the signs of the disease:
- Diet;
- Prevention of cardiovascular diseases;
- Intellectual loads;
- Getting enough vitamins;
- Fighting bad habits;
- Physical exercise;
- Fighting obesity.
Some foods should be included in the diet, as they have useful and necessary properties: fruits, vegetables, cereals, olive oil, red wine, grapes (namely seeds), cinnamon, coffee. Some of these foods have anti-amyloid properties, while others contain optimal amounts of essential nutrients and minerals.
What influences the development of Alzheimer's disease?
1. Age
is the strongest factor in the development of Alzheimer's disease.
According to various estimates, about 13 percent of people over 65 years old
suffer from dementia.
Women suffer from it somewhat more often. Scientists explain this by the longer life expectancy of the fairer sex. Many men simply do not live to see the development of Alzheimer's disease. 2. Lifestyle
. A growing body of research into Alzheimer's disease has linked the disease to lifestyle factors such as obesity, diabetes, high blood pressure and elevated cholesterol. As a rule, these factors are the consequences of a sedentary lifestyle and unhealthy diet.
Prevention of dementia
Learn how to prevent cognitive decline by avoiding bad habits and getting outside for walks and runs.
3.
Education
. Research shows that Alzheimer's disease is less common among educated people. Scientists say that reading, analytical work and memory training are suitable for preventing the disease.
Alzheimer's analogues
Hackebusch-Heuer-Geimanovich disease (syndrome) is an “Alzheimer-like” picture that develops as a result of atherosclerotic lesions of cortical vessels joining the senile-atrophic process.
Psychotic forms of senile dementia represent a heterogeneous group. The belonging of most observations to senile dementia is beyond doubt. These are affective, paranoid, hallucinatory, confabulatory psychoses that last for 1–3 years, developing at a late age, usually following a personality shift, reminiscent of the initial stage of senile dementia. After a gradual reduction of psychotic symptoms, dementia slowly increases, more or less close to senile. Such variants of senile dementia usually develop as a result of a special combination of factors: constitutional-genetic (hereditary burden of endogenous psychoses and the schizothymic personality of patients) and the relatively weak progression of the atrophic process. There are also cases that are less unambiguous in nosological terms, namely, chronic psychoses manifesting in old age, and sometimes in the involutionary period, developing according to the laws of continuously occurring schizophrenia. Usually these are hallucinatory-delusional psychoses with stabilization of the clinical picture at the paraphrenic stage - first at the fantastic-hallucinatory stage, and then at the confabulatory stage. Rare cases of chronic catatonia are also possible. The development of such psychoses is accompanied by personality changes: autism, isolation, inactivity. After a very slow reverse development of psychotic disorders (after 5 - 10 years or more), mnestic-intellectual disorders are discovered, which, however, do not reach significant depth. The relationship of these cases to the main form of senile dementia remains unclear; perhaps (taking into account their frequent hereditary burden with schizophrenia), they represent special age-related psychoses (with phenomena of increased mental aging) in a schizophrenic family circle.
- Services Prices
- Consultation with a psychiatrist-gerontologist 5000 rubles
- Calling a psychiatrist to your home for an elderly person 12,000 - 15,000 rubles
- Certificate of incapacity of an elderly person 5,000 rubles
- Initial consultation with a psychiatrist 5000 rubles
- Appointment with a psychiatrist, candidate of medical sciences, with 30 years of experience (50-60 min) 6,000 rubles
- Urgent call of a psychiatrist to your home (within the Moscow Ring Road) 12,000 - 15,000 rubles
- Psychiatric examination before the transaction (in the center) 5,000 rubles
- On-site psychiatric examination (60 min) 12,000 - 15,000 rubles
- Certificate of legal capacity when selling an apartment 5,000 rubles
- Conclusion on mental health 5000 rubles
Request a call back Make an appointment