Classification of autoimmune diseases in neurology
The main autoimmune diseases affecting the central nervous system are:
- Multiple sclerosis and some rarer demyelinating diseases. Antibodies are produced against the sheath of nerve processes - myelin. The result is a disruption of signal transmission along nerve fibers. Main symptoms: various visual impairments, weakness and numbness of the arms and/or legs, unsteadiness, urination problems.
- Autoimmune encephalitis. A large group of diseases, the common feature of which is damage exclusively to the brain. Each encephalitis is distinguished by a specific type of antibody and, therefore, by some features of the clinical picture. However, for all autoimmune encephalitis there are a number of common symptoms: mental disorders, memory impairment, seizures.
Autoimmune diseases affecting the peripheral nervous system (nerve roots and nerves):
- Guillain-Barre syndrome. Acutely developing autoimmune disease. Antibodies are produced against the myelin of peripheral nerves. It manifests itself as ascending muscle weakness up to weakness of the respiratory muscles, less often numbness.
- Chronic autoimmune polyneuropathies. A group of diseases that manifest themselves as various combinations of weakness and numbness of the limbs and have a slowly progressive course.
Autoimmune diseases affecting the muscles and neuromuscular system:
- Myasthenia. Antibodies in myasthenia gravis affect the area where nerves and muscles connect—the synapses. As a result of exposure to antibodies, the sensitivity of the muscles to the signal coming from the nerves is reduced. Clinically, the condition is manifested by muscle fatigue - muscle weakness is not felt constantly, but increases gradually during movement.
- Myopathies. Muscle damage can also be autoimmune in nature. These diseases are united by a common symptom - muscle weakness, the severity and localization of which, however, varies depending on the disease and the type of antibodies.
PsyAndNeuro.ru
Neuroleptic malignant syndrome (NMS) is a rare but extremely dangerous complication of neuroleptic therapy, occurring with central hyperthermia, catatonic symptoms with muscle hypertonicity, impaired consciousness and a complex of somatovegetative disorders. The course of NMS is accompanied by changes in the basic parameters of homeostasis and the function of vital organs and systems of the body and can lead to death. Mortality in NMS, according to various publications, ranges from 5.5 to 10% [5, 9, 13, 29, 34, 37, 43], and the incidence of development from 2 to 0.01% of all patients receiving antipsychotics [14, 22, 39, 43]. NMS most often develops during neuroleptic therapy in patients with schizophrenia or schizoaffective disorder. The world literature describes cases of the development of complications in patients with affective disorders, dementia and organic psychoses [34]. The development of NMS can be observed when antipsychotics of various chemical groups are prescribed, regardless of their dosage. The most common development of complications was observed when prescribing a traditional antipsychotic, haloperidol [5, 21, 34, 39, 43]. There are descriptions of the development of NMS with the use of atypical antipsychotics - clozapine, risperidone, quetiapine and olanzapine [34, 35, 43], as well as during the immediate withdrawal of psychotropic drugs [5].
The etiology and pathogenesis of NMS remain to date not fully understood. Most researchers explain the development of NMS by blockade of dopamine receptors in the basal ganglia and hypothalamus, and not by the direct toxic effect of neuroleptics [13, 29]. In patients with NMS, there is a suppression of dopaminergic and increased adrenergic and serotonergic activity [40]. A number of researchers consider NMS as a manifestation of acute neuroleptic encephalopathy [1]. In this case, the EEG reveals signs of metabolic encephalopathy with generalized inhibition of electrical activity of the brain [14, 43]. The results of clinical and pathogenetic studies have established that in the pathogenesis of NMS and febrile schizophrenia, an important role is played by immunological disorders and increased permeability of the blood-brain barrier, with neurosensitization of the body and subsequent autoimmune damage to the central nervous system, mainly the hypothalamus and visceral organs [9, 10]. Proof of this is high humoral sensitization to various autoantigens of the brain with the detection of antibodies to the frontal lobe, thalamus and the maximum amount (up to 66%) to the hypothalamus [9]. The cause of death is increasing disturbances of homeostasis and, first of all, water-electrolyte balance and hemodynamics, and the phenomenon of cerebral edema.
Analysis of pathomorphological changes in patients with lethal NMS is not presented in the world literature. The discovered pathomorphological changes in the brain in febrile (hypertoxic) schizophrenia, and a number of researchers consider NMS as a drug-induced form of lethal catatonia, do not fit into any specific nosological form and can be attributed to a toxic-dystrophic process in combination with generalized dyscirculatory disorders. In the thalamo-pituitary region of the brain in these patients the following changes are detected:
1) acute swelling, vacualization, ischemia and death of nerve cells;
2) swelling and swelling of the myelin sheaths of gangliocytic fibers;
3) hypertrophy and dystrophic changes in microgliocytes [7].
Risk factors for the development of NMS are the presence of residual cerebral organic failure in patients (previous antenatal and perinatal injuries, traumatic brain injury, infections and intoxications) [5, 9]. It is assumed that physical exhaustion and dehydration, occurring against the background of psychomotor agitation, can lead to increased sensitivity to neuroleptics and contribute to the development of NMS [21, 43]. Risk factors for NMS also include the presence of catatonic disorders [43].
Diagnosis of NMS is based on identifying the main symptoms of the complication: central hyperthermia, catatonic symptoms with the development of stupor and muscle rigidity, impaired consciousness, as well as characteristic changes in laboratory parameters (moderate leukocytosis without band shift, leukopenia and acceleration of ESR, sharp activity of CPK in the blood plasma).
The earliest sign of the development of NMS in patients with schizophrenia and schizoaffective psychosis, which is important for the diagnosis of complications, is the appearance of extrapyramidal symptoms with simultaneous exacerbation of psychosis and the development of catatonic disorders in the form of stupor with symptoms of negativism and catalepsy [5, 43]. In this regard, some researchers consider NMS as a neuroleptic variant of malignant or febrile catatonia, classifying them as diseases of the same spectrum [3, 31, 30]. This is confirmed by both the common clinical manifestations of febrile schizophrenia and NMS [7, 8, 41], and the similarity of biochemical and immunological disorders [9], as well as the general principles of therapy. They include the abolition of antipsychotics, the prescription of tranquilizers, infusion therapy and ECT [5, 9, 14, 19, 36, 43, 45]. The effectiveness of the dopamine receptor agonist bromocriptine and the muscle relaxant dantrolene in NMS has not been confirmed by evidence-based studies [6, 37, 38]. There is data on the effectiveness of plasmapheresis and hemosorption [3, 5]. The prognosis for the course of NMS depends on how quickly neuroleptic therapy is discontinued and intensive infusion therapy is prescribed to correct homeostasis. With timely withdrawal of neuroleptics, adequacy of infusion therapy, and differentiated use of ECT methods, it is possible to achieve a therapeutic effect in most patients within the first 3–7 days [5]. In accordance with the recommendations of DSM-5, NMS must be differentiated from diseases such as viral encephalitis, volumetric , vascular and autoimmune lesions of the central nervous system, as well as with conditions associated with the use of other drugs (amphetamines, phencyclidine, monoamine oxidase inhibitors, serotonergic antidepressants and a number of other drugs).
In 2007, a case series of autoimmune NMDA receptor encephalitis was first described, occurring with psychotic symptoms and catatonia, autonomic disorders and hyperthermia, and the risk of death [16]. The symptoms of this disease are similar to NMS and febrile catatonia and cause difficulties in differential diagnosis [15, 23]. The disease is caused by antibodies to the NR1 and NR2 subunits of the glutamate NMDA receptor. Anti-NMDA receptor encephalitis was initially described in young women with ovarian teratomas [16]. Subsequently, without connection with the tumor process in people of both sexes and different ages [26]. Diagnosis of anti-NMDA receptor encephalitis is based on the detection of autoantibodies to the NR1 and NR2 subunits of the glutamate NMDA receptor in the blood plasma and cerebrospinal fluid [17, 18, 20]. In recent years, cases of autoimmune encephalitis have been identified in psychiatric patients with initial diagnoses of schizophrenia, schizoaffective disorder, narcolepsy and major depressive disorder [42, 46]. Treatment of the disease involves immunotherapy with the administration of immunoglobulin and methylprednisolone. Second-line drugs used when there is no effect are rituximab in combination with cyclophosphamide. To relieve psychomotor agitation, tranquilizers, atypical antipsychotics, or chlopromazine can be used [25, 44]. There is positive experience with the use of ECT [12, 24, 27, 29, 32] and plasmapheresis [11, 33].
Patient Sh., born in 1988, was admitted for treatment to the Clinical Psychiatric Hospital No. 4 named after. P.B.Gannushkina June 18, 2015 with a diagnosis of acute polymorphic psychotic disorder.
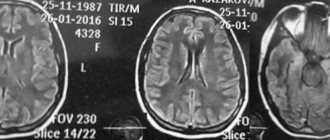
History . Heredity is not burdened with psychopathology. The patient's mother's pregnancy and childbirth proceeded without pathology. Born on time. The eldest of 2 children. Has a younger sister. Early development is correct. By nature she was calm, balanced, sociable and active. She suffered from childhood infectious diseases without complications. I went to school at the age of 7. I studied well. She graduated from 9 classes of general secondary school, then a pedagogical college and a pedagogical institute. At the age of 22 she got married. She lived with her husband, a 3-year-old child from the marriage, good family relations. Works at school as a primary school teacher. Has no bad habits. According to her husband, the patient’s mental state changed for the first time since the beginning of June 2015. She became distracted, forgetful, and anxious. She constantly asked her loved ones: “did she feed the baby?”, “did she go to the toilet”, said that it was as if her “head was separate from her body”, at times she unexpectedly fell to the floor, but immediately got up. On June 16, 2015, she applied for examination to the National Center for Neurology. MRI of the brain revealed signs of an area of gliosis in the right parietal lobe (8 mm–13 mm–18 mm), which must be differentiated from an ischemic and demyelinating or space-occupying process. No data were obtained for the presence of aneurysms or arteriovenous malformations at the levels studied. In the evening of the same day, she became anxious, restless, confused, asking “what is happening around?” There was an increase in systolic blood pressure to 180 mmHg. It was a restless night. The next day she began to express ridiculous ideas, she believed that she had been “bitten by a tick” and that she was pregnant. She claimed that songs were playing in her head. She periodically experienced fear and anxiety, was concerned that she would not be able to work, believed that her child would be “taken away”, said “I will die”, noted that it was as if someone was controlling her, her movements were happening against her will. On June 18, 2015, she returned to the neurology center. At the reception she was excited, shouting “where is my mommy?”, talking to herself, waving her arms chaotically, growling, spitting. Due to inappropriate behavior, she was examined by the psychiatrist on duty and was involuntarily hospitalized in PKB No. 4.
Mental state upon admission . She was taken to the department accompanied by orderlies and subjected to physical restraint. Examined within the bed. There is little access to productive contact. Tense, anxious, listening to something, looking around. Only responds to whispered speech. Answers in a quiet voice, brief, often nods or shakes his head. From the conversation it was possible to reveal that she had not slept for several nights and was experiencing influxes of thoughts in her head, “the sound of thoughts.” He does not deny the presence of “voices” that interfere with sleep and prohibit him from answering questions. The answer is mostly “I don’t know.” At times he screams loudly, wriggles, and spits.
Somatic condition : tall, correct physique, satisfactory nutrition. The skin and visible mucous membranes are of normal color. There are injection marks on the right elbow. There are isolated red rashes on the face. Body temperature is normal. Zev is calm. In the lungs there is vesicular breathing, no wheezing. NPV 16 per minute. Heart sounds are muffled and rhythmic. Heart rate 82 beats/min. Blood pressure 130/80 mmHg. The tongue is clean and moist. The abdomen is soft and painless on palpation. The liver and spleen are not palpable. The “tapping” symptom is negative on both sides. There is no swelling.
Neurological status : symmetrical face, D=S pupils, photoreaction preserved. There is an increase in tendon reflexes. Muscle tone is not increased. There are no meningeal signs, focal neurological symptoms are absent. Laboratory examination data. A study of general clinical and biochemical blood and urine tests did not reveal any significant pathological changes; RW, HIV, HBSAg, HCV were negative, BD, BL were not detected. RPGA – tetanus – 0.77, diphtheria – 0.17. ECG – sinus rhythm, heart rate 55–62 per minute. Normal EOS.
Dynamics of the condition and ongoing therapy . From the first day of admission, the patient was prescribed haloperidol 15 mg/day IM, trihexyphenidyl 6 mg/day, tiapride 400 mg/day IM, chlorpromazine 25 mg/day IM. Psychomotor agitation was stopped only in the evening. In the first days, the patient’s condition remained unstable, there were episodes of psychomotor agitation with an influx of hallucinatory experiences, she shouted incoherent phrases, talked to herself, and covered her head with a blanket while lying in bed. She took the treatment under duress and ate very little with persuasion. Productive contact remained inaccessible. Gradually, during therapy, psychomotor agitation was completely stopped. However, inhibition began to increase with an increase in muscle tone. The patient lay motionless in bed all the time, at times moving her lips. She responded only to whispered speech. Symptoms of “waxy flexibility” and “air cushion” appeared. Due to refusal to eat, from June 23, 2015, infusion therapy with saline solutions and glucose solutions up to 800 ml per day was prescribed. However, it was not possible to achieve improvement in the patient's condition. From July 1, 2015, haloperidol and tiapride were discontinued and olanzapine was prescribed at a dose of 20 mg/day, phenazepam 1 mg at night along with infusion therapy. After a relatively short period of improvement, when the patient began to independently move around the department and eat food, a deterioration occurred. From 07/06/2015, an increase in body temperature up to 38.5ºС and tachycardia up to 110 beats began to be noted. per minute, muscle rigidity of the lower and upper extremities, catalepsy with the “air cushion” symptom reappeared. In the blood, high levels of CPK (2,427 units/l) were detected in a biochemical blood test, slight leukocytosis (8.4 thousand), ECO 15 mm per hour. In order to exclude somatic pathology, the patient was repeatedly examined by a therapist: no evidence of somatic pathology was identified. X-ray of the lungs dated July 14, 2015 did not reveal any pathological shadows.
To prevent pneumonia, antibacterial therapy was prescribed - ceftriaxone 1.0 IM 2 times a day. From July 13, 2015, olanzapine was discontinued and infusion therapy was increased to 1,200 ml/day. Despite the therapeutic measures taken, the condition remained serious. The patient lay in bed all the time, refused to eat, practically did not respond to treatment, sometimes responded only to whispered speech, symptoms of “waxy flexibility” were noted, hyperthermia and muscle rigidity persisted. On July 15, 2015, she was examined by the emergency neurologist on duty.
Conclusion : phenomena of cerebral edema against the background of intoxication syndrome. It is recommended to perform a CT scan of the brain, MRI with contrast, and transfer to a hospital with an intensive care unit. At 19:50, accompanied by a resuscitation team, the patient was transferred to the PSO of the City Clinical Hospital named after. S.P. Botkin for continued treatment and examination.
Upon admission, the condition was assessed as serious. Retardation with elements of stupor remained, did not respond to addressed speech, and responded poorly to painful stimuli. There was an increase in tone in the muscles of the limbs and neck. Lethargy, which periodically gave way to excitement, limited to the confines of the bed, with the repetition of individual words, similar to speech stereotypies. In the somatic status, pallor of the skin and tachycardia up to 110 beats were noted. per minute, hyperthermia. For the purpose of differential diagnosis of demyelinating disease and encephalitis, a lumbar puncture was performed - cytosis 40 in 3 ml, protein 0.33, lymphocytes 37, neutrophils 3. Antibodies to the Epstein-Barr virus, herpes virus, mycobacterium tuberculosis and treponema pallidum were not detected in the cerebrospinal fluid.
After examination by an infectious disease specialist, the diagnosis of viral encephalitis was removed. An MRI of the brain with contrast on July 21, 2015 revealed an area of acute edema in the semioval centers on the right, which should be differentiated from acute ischemic cerebrovascular accident, tumor, demyelinating and autoimmune disease. The results of immunotyping of cerebrospinal fluid lymphocytes did not confirm the lymphoproliferative disease. In the intensive care unit, infusion therapy was administered up to 2 liters. per day under the control of diuresis, detoxification therapy, antibacterial therapy (cefritiaxone, amoxicycline). From July 24, 2015, dexamethasone 12 mg/day intravenously was added to the treatment regimen. Despite the therapy, the patient’s condition remained serious; there was an increase in body temperature to 40º C and a drop in blood pressure.
Conclusion of the consultation of doctors dated July 29, 2015 . The patient's condition is serious, febrile fever and catatonic symptoms persist. It seems most likely that the patient has febrile schizophrenia. The changes revealed in the MRI study, given their discrepancy with the clinical symptoms, are apparently an accidental finding and may be a consequence of a previous cerebrovascular accident.
On July 29, 2015, respiratory and cardiac arrest occurred. The resuscitation measures initiated did not lead to the restoration of breathing and cardiac activity. At 22:15 biological death was declared.
At the autopsy . Autoimmune encephalitis with predominant damage to the subcortical structures of the brain: hippocampus, thalamus, hypothalamus. Perivascular lymphoplasmacytic infiltrates with the release of immunocompetent cells into the substance of the subcortical structures of the brain; perivascular and pericellular edema; dystrophy of ganglion cells with partial cytosis and reactive gliosis with the formation of gliomesodermal foci. Cause of death: the patient's death (primary cause) was due to autoimmune encephalitis, complicated by cerebral edema with dislocation of its trunk into the foramen magnum (immediate cause of death).
This clinical case demonstrates the difficulties of differential diagnosis and treatment of NMS. A patient aged 26 years developed an acute psychotic attack of a polymorphic psychopathological structure with acute sensory delusions, verbal pseudohallucinations and mental automatisms. From the first days of manifestation, the structure of the attack was marked by catatonic disorders in the form of impulsivity, negativism (responded only to whispered speech), and elements of hebephrenic arousal (growled, spat). Thus, the structure of psychosis was characteristic of manifest attacks traditionally described in schizophrenia and schizoaffective psychosis. Against the background of neuroleptic therapy with haloperidol and tiapride, there is an increase in inhibition with an increase in muscle tone, catalepsy appears with symptoms of “waxy flexibility” and “air cushion”. This transformation of psychosis is characteristic of the initial stage of development of NMS. The discontinuation of haloperidol and tiapride and the prescription of the atypical antipsychotic olanzapine along with infusion therapy only led to an improvement in the patient's condition for a short time. Subsequently, there is an increase in catatonic disorders - stupor, followed by excitement, somatic disorders appear in the form of hyperthermia, tachycardia, instability of blood pressure, characteristic changes in laboratory parameters (minor leukocytosis without band shift, acceleration of ESR and a sharp (10 times), increase in CPK activity in blood serum).
A thorough somatic, laboratory and instrumental examination, including examination of the cerebrospinal fluid and MRI of the brain with contrast, could not establish the cause that could underlie the development of the patient’s severe mental and somatic condition.
The patient's death occurred against the background of hyperthermia and increasing signs of cerebral edema, despite the abolition of antipsychotics, intensive therapy and the prescription of dexamethasone. The data from the pathological examination revealed that the patient had a manifestation of autoimmune encephalitis with damage to the subcortical structures of the brain, which was the basis for a discrepancy in diagnosis. At the same time, the patient’s blood and cerebrospinal fluid were not tested to detect autoantibodies to NMDA receptors, on the basis of which autoimmune encephalitis is diagnosed. In addition, the results of the pathomorphological study do not contradict the diagnosis of NMS, since clinical and pathogenetic studies have proven the important role of autoimmune pathology with predominant damage to the hypothalamus in the pathogenesis of the development of febrile attacks of schizophrenia [9].
It is known that neuroleptics, when combined with blood plasma proteins, acquire the properties of haptens to which antibodies begin to form, blocking their antipsychotic effect [3]. Under certain conditions, they are apparently capable of triggering the development of an autoimmune process and causing the development of NMS. It should be noted that, until recently, the diagnostic algorithm for NMS did not involve testing the blood and cerebrospinal fluid for the presence of autoantibodies to NMDA receptors. At the same time, in the world literature there are descriptions of cases where the initially diagnosed diagnosis of NMS was revised after autoantibodies to NMDA receptors were detected in the blood and cerebrospinal fluid [23]. It can be assumed that early diagnosis of NMS with the abolition of antipsychotics, the appointment of adequate infusion therapy and ECT would prevent death. However, the peculiarity of this case was that even before the manifestation of psychosis, the patient showed changes on MRI of the brain in the form of an area of gliosis, which did not make it possible to completely exclude the presence of a current organic disease of the central nervous system and make a diagnosis of an endogenous disease - schizophrenia or schizoaffective psychosis based on the structure of psychopathological disorders.
Source: D.I. Malin, V.N. Gladyshev. Neuroleptic malignant syndrome or autoimmune anti-NMDA receptor encephalitis? Analysis of a clinical case with a fatal outcome. Social and Clinical Psychiatry 2021, vol. 27 no. 1.
Literary references can be viewed in the original
Causes of Rasmussen's encephalitis
The leading etiological factor is not fully understood. Scientists have formulated two probable hypotheses for the origin of the disease, namely:
- pathology occurs as a result of the penetration of viral microorganisms into the brain, while typical pathophysiological changes are observed - the appearance of infiltrative formations, proliferation of astrocytes at the site of death of neurocytes, proliferative processes of microglia. But during diagnostic procedures the pathogen is not determined;
- the autoimmune nature of the disease - in support of this hypothesis, specific antibodies to glutamate receptors were identified, under the influence of which necrosis of cells of the nervous system develops, and focal processes develop.