The simplest single-celled organism, Naegleria Fowler, usually lives in fresh water bodies with warm water. During bathing, this parasite can enter the human body through the nasal cavity, then through the olfactory canal it enters the brain area. As a result, this organism causes such a rare but very dangerous pathology as amoebic meningoencephalitis.
During this pathological process, damage to nerve cells, necrosis of the meninges, as well as swelling and hyperthermia of the brain are observed. As a result, the formation of purulent exudate around the bulbs occurs. This disease usually has a poor prognosis, often accompanied by death. Each person exhibits different symptoms, their intensity and severity depends on the degree of damage to the nervous system. Therefore, it is imperative to know the main causes and symptoms of this disease so as not to become infected with this terrible pathology.
This is what amoebas look like
Content
Definition and general information [edit]
The source of invasion is water, soil, etc. contaminated with amoebas. A person becomes infected through contact, household, water and food routes.
The incidence is sporadic, infection is possible in all seasons of the year.
Etiology and pathogenesis[edit]
Acanthamoebas are free-living protozoans. For humans, 6 species of amoebae of the genus Acanthamoeba are pathogenic: Acanthamoeba astronyxis and Acanthamoeba palestinensis - affect the central nervous system, Acanthamoeba hatchetti - eyes, Acanthamoeba polyphaga, Acanthamoeba culbertsoni and Acanthamoeba Castellanii - central nervous system and eyes. Some of them affect the skin.
Once in the human body, acanthamoebas are capable of switching to parasitism and completing their development cycle in the host’s body, forming cysts.
Amoebas are introduced into the brain hematogenously from primary lesions of the cornea or respiratory tract.
Acanthamoebas are often found in nasopharyngeal swabs and in the feces of healthy people. In persons with immunodeficiency conditions, especially with HIV infection, acanthamoebiasis manifests itself in a manifest form (opportunistic invasion).
Clinical manifestations[edit]
Acanthamoeba keratitis and skin lesions develop more often. Granulomatous amebic encephalitis is rarely reported.
occurs when drops of water containing amoebas or their cysts enter the conjunctival cavity in people who use soft contact lenses and do not follow hygienic rules for caring for them.
In the central part of the cornea, a sluggish superficial and then deep (stromal) infiltrate appears in the shape of a ring or oval with a clear or relatively clear center. The disease develops slowly, over weeks or even months.
Possible complications: iridocyclitis with hypopyon (accumulation of pus in the anterior chamber of the eye), with progression of the process - perforation of the cornea.
Acanthamoeba skin lesions
can be primary or secondary, developing after damage to the central nervous system.
The skin is primarily affected when amoeba or cysts come into contact with open skin wounds with contaminated water or through household contact.
Gray-black spots with a diameter of 3 cm, single or multiple papules and nodules with a diameter of 0.5-1 cm appear on the skin of the face, back, chest, upper and lower extremities. Ulcers form at the site of the spots and nodules, which are covered with a scab.
When examining a biopsy specimen, fibrosis of the tissue with an inflammatory infiltrate is noted, and thick-walled cysts of spherical amoebae are detected.
With a long course of the disease, the formation of amoebic abscesses in the muscles, lymph nodes, lungs, liver and other internal organs is possible.
Granulomatous acanthamoeba encephalitis
are recorded extremely rarely.
The clinical picture and nature of the disease are determined by:
• localization of lesions in the brain and damage to the substance of various parts of the brain, pia and arachnoid membranes, basal ganglia;
• resistance of the body: with preserved resistance of the body, the granulomatous process predominates, in immunodeficiency states - necrotic.
The incubation period ranges from several weeks to several months.
In the initial period of the disease the following is noted:
• headaches, drowsiness, convulsions;
• hemiparesis, focal symptoms of damage to certain parts of the brain;
• sometimes convergence disorders;
• often intermittent fever with body temperature rising to 38 °C. The disease gradually progresses, coma and death occur.
Acanthamoebiasis: Diagnosis[edit]
A postmortem examination reveals swelling of the cerebral hemispheres, areas of softening with exudate on the surface of the cortex, and thickening of the soft membranes. On sections in most parts of the brain, multiple foci of softening with hemorrhagic necrosis with a diameter of 1.5-6.5 cm are found. Trophozoites and Acanthamoeba cysts are found in necrotic masses.
For the diagnosis of acanthamoeba keratitis
use:
• microscopic examination of tear-meibomian fluid, washings and scrapings from ulcers of the cornea and sclera (under low light or using phase contrast);
• bioassays with infection of laboratory animals.
Diagnosis of acanthamoeba skin lesions is based on the detection of amoebas and their cysts in native and stained preparations prepared from the substrate of infiltrates and biopsies of affected tissues.
Methods for diagnosing acanthamoeba encephalitis
:
• study of native CSF preparations, in which motile trophozoites stained according to Giemsa-Wright are determined; trophozoites and cysts stain purple;
• cultural method with inoculation of CSF on Culberston's medium. Differential diagnosis for acanthamoeba lesions of the eyes, brain and skin is carried out with keratitis, encephalitis and dermatoses of other etiologies.
Differential diagnosis[edit]
Acanthamoebiasis: Treatment[edit]
• refusal of contact lenses;
• Neomycin/polymyxin B/dexamethasone or Gramicidin C/Dexamethasone/Framycetin in the form of drops 6-12 times a day or in the form of an ointment 3-4 times a day; in combination with drops, the ointment is used once at night;
• drops of solutions of gentamicin 0.3%, tobramycin 0.3%, tetracycline 1%;
Despite drug treatment, keratoplasty is sometimes performed.
Treatment of acanthamoeba skin lesions:
• antibiotics from the aminoglycoside group (gentamicin);
Treatment of amoebic meningoencephalitis is effective only if it is diagnosed early, which is extremely rare. There are only 3 known cases of cure for granulomatous acanthamoeba encephalitis.
The main drug is amphotericin B intravenously or into the spinal canal: on the first day - 0.1-0.2 mg/kg, on the second day - 0.25-0.5 mg/kg, on subsequent days - 0.8 -1.0 mg/kg body weight daily, after achieving the effect - every other day.
At the same time, co-trimoxazole and antibiotics from the aminoglycoside group are prescribed.
Chloramphenicol (chloramphenicol) is used orally: for adults and children over 14 years old - 1.5-3.0 g (up to 4 g per day) for 2-4 doses; children 1 year and older – 50-100 mg/kg per day in 4 divided doses; parenterally (intramuscular or intravenous): adults – 50-100 mg/kg per day for 4 administrations; children over 14 years old – 50-75 mg/kg per day for 4 administrations; children from 2 weeks to 2 months – 25 mg/kg per day for 2 administrations; from 2 months to 1 year – 50 mg/kg body weight per day for 3-4 administrations.
Preventive measures
This pathology is considered dangerous and very scary, so you should protect yourself in advance from contracting this disease. In this case, it is worth remembering several important recommendations that will help avoid infection with amoebic meningoencephalitis:
- you should refrain from swimming in warm, stagnant bodies of water, especially with dirty water, which are not subject to sanitary control;
- It is better to protect your nose while diving - to do this, you can hold it with your hands or put a special clothespin on it;
- if you have to work in the garden or in a vegetable garden with wet soil, then you need to wear a mask and gloves on your hands;
- after working with wet soil, be sure to clean your hands and rinse them well; you also need to clean out all the dirt from under your nails;
- monitor children’s hygiene, do not allow them to pick their noses with dirty fingers;
- It is worth considering that amoeba cysts have increased vitality, so it is necessary to periodically clean air conditioner humidifiers;
- You should only drink boiled water.
Nose clips
Infection with amoebic meningoencephalitis can affect absolutely anyone. For this reason, it is important to follow preventive recommendations. These rules will help not only prevent infection, but also protect against unpleasant consequences that may arise from this pathology. Even if a person manages to be cured, he may still remain disabled for life. To prevent this from happening, you should carefully monitor where you swim in the summer, be sure to use protective equipment when working with the soil, as well as perform regular house cleaning and air conditioning cleaning.
Granulomatous amebic encephalitis
Granulomatous amebic encephalitis
(GAmE) is a protozoal disease characterized by progressive granulomatous-destructive brain damage, occurring predominantly in immunocompromised people due to invasion by free-living amoebae of the genus Acanthamoeba viBalamuthia mandrillaris.
B. mandrillaris
were first isolated from the water of natural reservoirs in the Telsa area (Oklahoma, USA). The first cases of HAME caused by these amoebae were described in 1990 by GS Visvesvara and AJ Martinez. GAME of acanthamoeba origin was first described in 1995 by JP Sison et al., Lowichik and JD Siegel among mentally retarded individuals in the USA.
Pathogens
- free-living amoebas of the genus Acanthamoeba: A.castellanii, A, culbertsoni, A.healyi (A.astronyxis), A. polyphaga, A. palestinensis, A. hatehetti, A.rhysodes, A. divionesis, as well as Balamuthia mandrillaris, belong to suborder Acanthopodina order Amoeba. The vegetative stage (trophozoite) of Acanthamoeba has dimensions of 14-40 µm, contains 1 nucleus with a nucleolus, and has thin ridges on the plasma membrane. Cysts, 12-16 microns in diameter, are enclosed in a double membrane with two pores.
Trophozoite
Balamuthia mandrillaris measures about 30 (12-60) µm and contains 1 nucleus. Cysts, with a diameter of 15 (6-30) microns, have a three-layer shell. Acanthamoebas are aerobes and reproduce at temperatures of 25-35 °C.
In natural conditions
Acanthamoeba and B. mandrillaris live in water, soil and air in various regions of the world.
Protozoa are often found in the nasopharynx of healthy people. The discovery of seropositive
results in the population of various regions indicates a wide distribution of protozoa.
Pathogens enter the body
humans through the skin and mucous membranes when swimming in open water or in contact with soil. The most susceptible to invasion are mentally retarded or mentally ill persons, as well as immunocompromised people - patients with diabetes mellitus, HIV/AIDS, intravenous drug users, chronic alcoholics, recipients of bone marrow and other tissue transplants, free people receiving antitumor and immunosuppressive drugs. In rare cases, diseases in immunocompetent individuals have been observed.
Invasion
widespread everywhere.
Cases of amebic encephalitis have been described in the central and southern regions of the United States, Central America, South Australia, New Zealand, Europe, and Africa. Less than 200 verified cases of diseases
caused by Acanthamoeba and about 70 diseases caused by B. mandrillaris have been described, almost half of them in the USA.
At the site of Acanthamoeba
Torpidly developing inflammatory foci (ulcerative skin lesions, sinusitis, pneumonia) often occur. This suggests the possibility of hematogenous dissemination of protozoa with their penetration into the brain and other organs (lungs, lymph nodes, skin, etc.). The greatest damage develops in the brain. In the midbrain, brainstem and cerebellum, foci of granulomatous inflammation are formed, in which multinucleated cells, accumulations of lymphocytes, and macrophages are found. Areas of brain tissue necrosis are identified around the granule. In the perivascular space, trophozoites and amoeba cysts are detected, which indirectly confirms the hematogenous spread of pathogens in the brain tissue.
When macroscopically studied, it is determined
severe cerebral edema, hemorrhages in the brain tissue and meninges, cerebellar entrapment. In the genesis of cellular lesions, a large role is played by the effect of parasitic proteases and other cytolytic factors and the accumulation of free calcium in the cytoplasm of cells.
Infestation of B. mandhllaris
develops both among immunocompromised and immunocompetent individuals. At the site of amoeba penetration, primary inflammatory foci are often formed, which subsequently ensure hematogenous dissemination of parasites. Foci of subacute granulomatous inflammation appear in the brain tissue, in which accumulations of macrophages, lymphocytes, plasma cells, and giant multinucleated cells are found. Angiitis with perivascular localization of trophozoites and cysts is characteristic. The process involves areas of the meninges adjacent to the source of inflammation in the brain tissue.
– Return to section table of contents “
Microbiology."
Meningoencephalitis: symptoms in adults
The clinical picture consists of general infectious, meningeal, focal and liquor-hypertensive symptoms. The most typical symptoms are:
- Increased body temperature;
- General malaise;
- Lack of appetite;
- Rashes on the skin;
- Liqueur hypertension (severe headache, nausea, vomiting that does not bring relief);
- Disturbance of consciousness (drowsiness\excitement, disorientation in place and space, possibly coma);
- Meningeal syndrome (increased sensitivity to light, sound, touch, hypertonicity of the posterior neck muscles, flexor muscles of the limbs, convulsions, severe headache);
- Hemiparesis (incomplete paralysis);
- Sensorimotor aphasia (loss of speech);
- Hyperkinesis (involuntary movements);
- Cerebellar syndrome (motor coordination disorder);
- Vestibular ataxia (impaired gait and coordination);
- Cognitive impairment (decreased mental activity, memory);
- Oculomotor and visual disorders (with damage to the cranial nerves) – double vision, strabismus, limited mobility, etc.;
- Distortion of the face, drooping eyelids;
- Hearing loss;
- Swallowing disorders;
- Dysarthria (violation of the speech apparatus).
Free-living pathogenic amoebas
Free-living amoebas are protozoans that live in soil or water and do not require hosts.
They rarely cause disease, unlike the parasitic amoeba Entamoeba histolytica, which is a common cause of intestinal infection. Pathogenic free-living amoebas belong to the genera Naegleria, Acanthamoeba and Balamuthia.
They can cause:
- Primary amebic meningoencephalitis.
- Granulomatous amoebic encephalitis.
- Amoebic keratitis.
Acanthamoeba can also cause skin lesions.
Diagnostic features
Since this pathology is quite dangerous and the patient’s death can occur at almost any time, it is important to diagnose this disease immediately after the first symptoms appear.
Features of examination at the primary stage of amoebic meningitis:
- to identify primary amoebic meningoencephalitis, bacterioscopy of fluid in the spinal cord and bacteriological blood culture are performed;
- if the patient has this pathology, then an increased level of red blood cells, protein, leukocytes will be found in his cerebrospinal fluid, and a reduced concentration of glucose will also be noted;
- Microscopic diagnostics of the liquid is required to determine the presence of mobile microorganisms.
During amoebic meningitis, the greatest damage occurs to the gray matter of the brain. Necrosis of nerve tissue is also observed; a large number of vegetative forms of parasites may be present around the arteries.
The main affected areas may be the diencephalon region and its periphery, or the posterior cranial fossa, which is located in the brain stem area.
Additionally, a lumbar puncture is performed during diagnosis. Increased cerebrospinal fluid pressure is usually noted during this test. The fluid may have a hemorrhagic structure with pronounced neutrophilic pleocidosis.
When collecting information when taking an anamnesis, you must tell the doctor whether you have recently swum in bodies of water. If patients have immunodeficiency, the damage may affect the lung area and skin.
However, in most cases, an accurate diagnosis is usually established after the death of the patient.
Granulomatous amebic encephalitis
Granulomatous amoebic encephalitis is characterized by a subacute course and is caused by free-living amoebae of the genus Acanthamoeba and Balamuthia, more often in debilitated individuals and those with weakened immune systems. Usually ends in death.
Acanthamoeba sp. and Balamuthia mandrillaris are present in water, soil and dust throughout the world. Infection in humans is likely, but infection is rare. CNS infection with Acanthamoeba occurs in almost completely immunocompromised or malnourished patients, but B. mandrillaris can also infect healthy hosts. The route of entry is believed to be the skin or lower respiratory tract, followed by hematogenous spread to the central nervous system.
Onset is sudden, often with focal neurological manifestations. Impaired mental functioning, seizures and headaches are common. B. mandrillaris can also cause skin lesions. Survival is very unlikely (and only among immunocompetent patients); death occurs between 7 and 120 days after illness onset (mean 39 days).
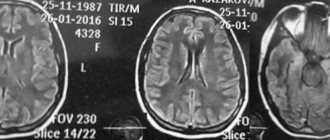
Diagnosis is often made after death. CT and routine CSF tests are done, but they are not specific. CT may show multiple nonenhancing clear areas; in the CSF there is an increased number of white blood cells (lymphocytes predominate), but trophozoites are rarely seen. Visible skin lesions often contain amoebas and should be biopsied; If pathogens are detected, they must be subjected to a test culture and tested for sensitivity to drugs. Brain biopsy is often positive.
Some patients with Acanthamoeba granulomatous encephalitis have responded to drug combinations that may include pentamidine; sulfadiazine or trimethoprim; sulfamethoxazole; flucytosine; fluconazole, ketoconazole, itraconazole or voriconazole; amphotericin B and other drugs. Skin infections caused by Acanthamoeba sp. are usually treated with the same medications and surgical debridement.
B. mandrillaris was treated with a combination of pentamidine, flucytosine, fluconazole, and sulfadiazine plus either azithromycin or clarithromycin, along with surgical resection.
Symptoms
Amebic meningoencephalitis can also occur in people with excellent health. Almost anyone, both adults and children, can become infected with this terrible pathology. The incubation period is from 2 to 10 days.
Typically, amoebic meningitis appears within 7 days after infection; during this period the following symptoms may be observed:
- Pain in the throat area.
- A dry cough may appear.
- Problems with smell.
- The appearance of vomiting, which does not bring relief.
- Migraine.
- There may be an increased degree of excitability.
- High body temperature.
These symptoms usually appear in other diseases, so this pathology can easily be overlooked or attributed to another disease. For this reason, examination of amoebic meningitis at the initial stage is quite difficult. Patients may think that this is a simple cold, for this reason they may not come to the doctor for a long time for diagnosis. After just 10 days, the following disorders of a neurological nature may be observed:
- increased tone of muscle fibers in the back of the head;
- the occurrence of seizures;
- problems with consciousness;
- manifestation of visual hallucinations;
- epileptic seizures;
- the occurrence of blindness;
- hearing problems, complete deafness may occur;
- coma state.
Amoeba in an approximate state
In the subsequent period, the causative agent of the disease, amoeba naegleria, begins to actively develop and multiply. In the course of its life, it quickly eats brain cells, for this reason, if treatment is not carried out in a timely manner, this can lead to death. It is worth noting that the mortality rate from this pathology is very high; patients cannot be saved in 90% of cases. The main reason for the increased mortality is that this disease is quite difficult to diagnose because the clinical signs are similar to those of bacterial meningitis. Often death occurs within 3–7 days after the first signs of this disease appear.
Amoebic keratitis
Amoebic keratitis is an infection of the cornea caused by Acanthamoeba sp., typically occurring in contact lens wearers.
Acanthamoeba sp. may cause chronic and progressive keratitis in the normal host. The main risk factor (85% of cases) is the use of contact lenses, especially if you swim in the lenses or if you use non-peryl lens solution. Some infections are the result of damage to the cornea.
The lesions are typically very painful and give the sensation of a foreign body. Initially, the lesions have a tree-like appearance resembling herpes simplex keratitis. Later, patchy stromal infiltrates and sometimes a characteristic ring-shaped lesion appear. There is usually preexisting uveitis. Vision deteriorates.
The diagnosis is confirmed by analysis of scrapings from the cornea using Giemsa staining or tricolor staining and test culture on special media. A test culture test for the virus is done if herpes is suspected.
Meningitis is an inflammation or infection of the meninges and cerebrospinal fluid (CSF). The meninges are three layers of protective tissue surrounding the brain and spinal cord. Liquor is a special liquid between the layers of the meninges that nourishes the brain.
According to the World Health Organization (WHO), the incidence of meningitis in the world is approximately 82 million cases per year. The Centers for Disease Control and Prevention (CDC) estimates that more than 1.2 million cases of bacterial meningitis occur each year worldwide.
Symptoms of meningitis
Meningitis usually causes nonspecific symptoms, but sometimes it can cause focal neurological symptoms (those that affect a specific function or part of the body).
Common symptoms of meningitis include:
- Fever
- Headache
- Stiff neck
- Fatigue and lethargy
- Photophobia (a feeling of discomfort when looking at light)
- Nausea and vomiting
- Dizziness
- Backache
- Confusion
- Drowsiness or trouble waking up from sleep
- A petechial rash, which looks like clusters of tiny purple dots on the skin, can occur with bacterial meningitis, especially meningococcal meningitis.
Signs of meningitis in children include crying, fussiness, loss of appetite, vomiting, excessive sleeping, decreased alertness, and decreased physical activity. The anterior fontanel may bulge.
Less commonly, meningitis can cause symptoms indicating brain damage, including:
- Weakness of the face, arms or legs or sensory changes on one side of the body
- Changes in vision
- Hearing loss
- Convulsions
Typically, viral meningitis and non-infectious meningitis cause mild to moderate generalized symptoms that can progress to severe signs and complications.
Bacterial meningitis can cause rapid worsening of generalized or focal symptoms with a high risk of complications. Fungal, parasitic, and amoebic meningitis are not common and may cause focal symptoms and/or seizures.
Complications after meningitis
If meningitis is not treated properly, it can lead to severe acute illness that requires intensive treatment. And sometimes meningitis leads to long-term problems, such as permanent hearing loss or cognitive deficits.
Types of meningitis
There are several types of infectious and non-infectious meningitis. They have different risk factors, expected outcomes, treatments, and complications. Meningitis can be diagnosed based on symptoms and a physical examination, and brain imaging studies may show signs of inflammation of the meninges.
The specific type of meningitis and the infecting organism can be determined using a lumbar puncture (LP), which is an invasive test.
- Viral meningitis
Viral meningitis is the most common type of meningitis. It can be caused by viruses that are commonly contagious in the community, including enterovirus, mumps virus, herpes simplex virus, varicella zoster virus (which usually causes chickenpox), Epstein-Barr virus, and West Nile virus.
Viral meningitis can develop as a complication of infection with any of these viruses, although most people who become infected with them do not.
Viral meningitis can develop in anyone, but is more common in children. Sometimes it is diagnosed clinically, without a lumbar puncture. People with healthy immune systems usually recover quickly from viral meningitis, but it can cause complications, especially in people with immune problems.
People whose meningitis is caused by a virus can pass the virus on to others, but those people are unlikely to get meningitis as a result.
- Bacterial meningitis
Bacterial meningitis is the second most common type of infectious meningitis, and it can be dangerous. The most common causes are streptococcal pneumonia, Neisseria meningitidis, Haemophilus influenzae, Listeria monocytogenes, and group B streptococcus.2 These organisms are common in the environment and are contagious.
Meningococcal meningitis, caused by N. meningitidis, is particularly associated with outbreaks among groups of people living in close quarters, such as dormitories or bunk rooms. Symptoms may progress rapidly and treatment should be directed at the infecting organism.
Typically, bacteria are identified by lumbar puncture.
Bacterial meningitis can develop in anyone, but is more common in people with weakened immune systems, who have had brain surgery or a head injury.
- Fungal meningitis
Fungal meningitis is not a common disease; a weak immune system is the leading risk factor.
Fungal meningitis can be caused by Candida (which is usually present on the skin), Cryptococcus, Histoplasma, Blastomycetes and Coccidioides. Organisms that can cause fungal meningitis are widespread in the community. They come into contact frequently, but do not usually cause infections in healthy people.
- Parasitic meningitis
Parasites can invade the body through exposure due to contamination from food that is not fully cooked or from the environment.
According to the CDC, the most common parasites that cause meningitis are Angiostrongylus cantonensis, Baylisascaris procyonis, and Gnathostoma spinigerum.
The parasitic infection can cause inflammation of the brain and may also appear as a mass or growth on the brain. Parasites can multiply after invading the body, or die and remain in the body, continuing to produce a mass effect in the brain. It is treated with antimicrobials and the organism can be surgically removed.
- Amoebic meningitis
Amoebic meningitis is very rare. An amoeba is a type of single-celled organism that typically lives in fresh water, lakes, rivers, soil, or contaminated sewer water. Organisms that can cause amoebic meningitis include Naegleria fowleri and Acanthamoeba species.
Because the disease is rare, it may not be easy to recognize, and brain imaging studies can reveal patterns of inflammation. Amoebic meningitis is often described as meningoencephalitis because the infection and inflammation affect the brain in addition to the meninges.
Symptoms may progress, and complications may occur if the condition worsens.
Treatment may include a combination of antimicrobial drugs commonly used to treat fungal infections, as well as surgery to treat fluid pressure in and around the brain.
- Non-infectious meningitis
Inflammation of the meninges and cerebrospinal fluid can occur without infection. Sometimes called aseptic meningitis, it can occur due to autoimmune diseases such as lupus, sarcoidosis, or rheumatoid arthritis. Not everyone who has these autoimmune diseases will develop associated meningitis. When this happens, meningitis caused by an autoimmune disease is usually uncommon and can cause fatigue, trouble concentrating, or confusion.
Non-infectious meningitis can also occur as a result of medications or radiation to the brain used to treat cancer. Cancer is a more serious cause of non-infectious meningitis. This can lead to leptomeningeal carcinomatosis, which is the spread of cancer cells throughout the lining surrounding the brain and spinal cord. This complication of cancer can be treated with intrathecal chemotherapy, which is injected into the cerebrospinal fluid.
Risk factors
Meningitis can affect anyone, but certain risk factors can make it more likely.
- Non-infectious meningitis is more common in people with underlying medical conditions such as sarcoidosis.
- Having a weak immune system, for example due to HIV infection or immunosuppressive therapy, is a major risk factor for infectious meningitis. Immunosuppressive treatments, such as steroids and more targeted drugs, are often prescribed to prevent organ rejection in people who have had organ transplants, or they may be prescribed to treat chronic inflammatory or autoimmune diseases. Chemotherapy drugs used to treat cancer also cause immunosuppression.
Complications from meningitis are more likely if the condition is not treated. Additionally, having a weakened immune system may predispose someone to a flare-up of meningitis, with an increased risk of long-term consequences.
Prevention of meningitis
There are several ways to prevent meningitis, and the most established preventive strategy is vaccination.
This disease is more common in areas of the world where vaccination rates are low. Vaccines that can prevent meningitis include vaccines that protect against:
- Pneumococcus
- Chicken pox
- Haemophilus influenzae
- Measles
- Piggy
- Neisseria meningitidis
Vaccines against N. meningitidis are specifically aimed at preventing meningitis:
- Meningococcal conjugate vaccine MenACWY (Menactra or Menveo) is recommended for everyone aged 11 to 12 years, with an increase at age 16, and for any children or adults who are at greater risk of meningococcal disease. This vaccine protects against four serogroups of bacteria.
- Meningococcal serogroup B vaccine MenB (Bexsero or Trumenba) is recommended for adolescents and young adults (especially ages 16 to 18) and anyone 10 years of age or older who is at increased risk of meningococcal disease. It is given in addition to the threat vaccine to add protection to serogroup B.
Even with vaccination, it is possible to develop this disease. Preventing infection is important for your overall health and can reduce your risk of getting meningitis.
Strategies to prevent meningitis include:
- Washing your hands, especially before eating and after using the toilet
- Avoiding contact with people who have an infection (even if the infection is not meningitis)
- Keeping your immune system healthy by getting enough sleep, eating fresh food, and staying active
Treatment
- Corneal sanitation.
- If necessary, propamidine plus biquanide.
- Possibly systemic fluconazole or itraconazole.
Early, superficial infection is more treatable. The encapsulated stage of the life cycle usually causes severe attraction difficulties.
Epithelial lesions are treated and drug treatment is prescribed. Propamidine isethionate 0.1% plus either polyhexamylene biguanidine or biguanidine chlorhexidine drops are often the drugs of choice initially; for the first 3 days, the drugs are given every 1 to 2 hours. Other drugs that may be used include aminoglycosides, hexamidine deisithionate, miconazole, and neosporin.
Systemic treatment with fluconazole or itraconazole has also been used, especially in patients with preexisting uveitis or scleral involvement. Early detection and treatment have eliminated the need for keratoplasty in most cases, but it remains the treatment of choice when pharmacologic therapy fails. Intensive treatment is carried out during the first month; then the dosage of the drug is reduced as the severity of clinical signs decreases, but often continues for up to 6-12 months. Relapse is possible if treatment is stopped prematurely.
Treatment of the disease
It should be remembered that amoebic meningitis is difficult to detect and treat.
In most cases, patients infected with Naegleria died. Treatment with amoebicidal drugs is ineffective. However, amoebas are sensitive to Amphotericin B (if necessary, it is injected directly into the ventricles of the brain), Miconazole, Rifampicin, and Tetracycline. The drugs of the Artemisinin B group had a positive effect. Anti-Negleria immune serum or monoclonal antibodies can be used. It should be remembered that the disease develops rapidly (counting the hours), so treatment should only take place in a hospital under the supervision of a doctor.
The disease cannot be treated at home. You should not self-medicate or use folk remedies. If the patient managed to survive and was transferred to outpatient treatment, the following recommendations must be followed:
- drinking plenty of fluids and eating quality food;
- twilight indoors;
- taking vitamins;
- bed rest;
- physiotherapeutic procedures.