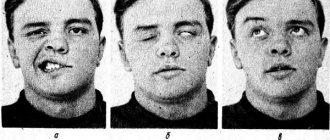
Sleep paralysis, or otherwise sleepy stupor, is a condition characterized by the occurrence of temporary paralysis, while the person’s consciousness remains preserved. As a rule, sleep paralysis occurs when waking up or falling asleep. People with sleep paralysis may experience complex hallucinations and intense fear.
This condition occurs in 10-40% of people aged 12 to 30 years, most often in those suffering from narcolepsy. Sleepy stupor is physically harmless, but experiencing it regularly without understanding the essence of what is happening can cause significant psychological trauma.
The neurology clinic of the Yusupov Hospital carries out comprehensive diagnostics, identifying the true causes of sleep paralysis and the diseases that lead to its occurrence.
General information
Sleep paralysis is sometimes also called old witch syndrome .
It is expressed in the form of a special phenomenon of complete or partial stupor - paralysis of various muscles, which occurs when falling asleep or, in more rare cases, when waking up from sleep, usually lasts from several seconds to several minutes, and can be interrupted by touch or a sharp sound. Pathology refers to sleep disorders and is a secondary disorder; it can be provoked by mental, neurological and somatic diseases. For paralysis during the transition to awakening and falling asleep, the most characteristic state is immobility and it is diametrically opposed to somnambulism - the ability of a person to perform movements in a dream. In a state of sleep paralysis, people are unable to speak, walk, move their arms, or even open their eyes, although they retain the ability to control eye movements.
Being one of the most common forms of rapid eye movement sleep disorder, paralysis can occur both in completely healthy individuals and in those suffering from hypnagogia , narcolepsy and catalepsy . Sleep paralysis is usually isolated, otherwise it may be associated with other disorders.
Available statistics (source Wikipedia) indicate that approximately 7% of people surveyed have experienced an attack of sleep paralysis at least once in their lives. However, it is very important to distinguish the medical phenomenon from fictional stories, when the pathological condition is attributed to fantastic explanations such as alien abduction or demonic attacks, although this type of parasomnia has received wider publicity.
Causes of pathology
Most often, sleep paralysis occurs when a person falls asleep on their back or right side. It can only happen if a person wakes up on his own - forced awakening or sharp sounds always lead to a complete interruption of sleep.
Attacks are provoked by the following factors:
- moving between time zones, leading to a disruption in the biological rhythms that regulate sleep - the risk of sleep paralysis will drop sharply after a short period of adaptation;
- restless sleep associated with stress and various experiences;
- lack of sleep;
- addictions - drugs, nicotine, alcohol, gambling and others that do not allow a person to completely relax;
- restless legs syndrome;
- psychiatric diseases;
- hormonal imbalances;
- taking antidepressants, neurostimulants.
There is also an assumption about the hereditary nature of sleep paralysis. Researchers know of entire families who suffer from repeated attacks of this condition from generation to generation.
Pathogenesis
This type of parasomnia, the occurrence of a motor phenomenon in a specific phase of sleep associated with the process of waking up and falling asleep, can be diagnosed by qualified neurologists even in healthy people. The condition is usually triggered by partial activation of the system responsible for REM sleep.
REM sleep is characterized by dreaming. To prevent a person’s physical ability to react to dreams and act in an emotional outburst, brain structures temporarily “paralyze” the possibility of muscle activity. Muscle dystonia occurs as a result of suppressed excitation of skeletal muscles in such parts of the brain stem as the pons and in the ventromedial region in the medulla oblongata.
Sleep structure
Inhibition occurs with the participation of glycine , γ-aminobutyric acid and other neurotransmitters that can suppress the functions of motor neurons located in the spinal cord.
Hallucinations and various strange physiological sensations are associated with the functioning of the vestibular apparatus and the need of the brain to establish the causes of disturbances and prevent the consequences of motor skills during sleep.
Night paralysis is characterized by the ability to be completely conscious while the body goes through the stages of rapid eye movement sleep. As a result, consciousness finds itself in a kind of trap: it is possible to see the world around us and everything that is happening around us, to control the breathing process, but there is no opportunity to move or speak.
Non-epileptic paroxysms during sleep
According to the International Classification of Sleep Disorders ICSD, the following groups of disorders are distinguished:
- parasomnias:
- dyssomnia;
- sleep disorders in somatic diseases,
- sleep disorders in psychiatric diseases.
PARASOMNIAS
Parasomnias are phenomena of non-epileptic origin that occur during sleep, but are not per se sleep disorders (Parkes, 1985).
In most cases, parasomnias occur during full or partial awakening, or when changing stages of sleep. Within the heterogeneous group of parasomnias, there are disorders of awakening, disorders of the transition from sleep to wakefulness, disorders combined with the REM sleep phase, etc. Polysomnography plays an important role in the differential diagnosis of parasomnia and epileptic paroxysms.
AWAKENING DISORDERS
Sleepy intoxication (ICSD 307.462)
The term "sleep intoxication" refers to a state of confusion during or after awakening from sleep (usually awakening from deep sleep in the first half of the night) (Roth et al, 1981). Sleepy intoxication is a nonspecific phenomenon observed in many hypersomnias,
Clinical characteristics. Sleepy intoxication can occur spontaneously or be provoked by a sudden awakening. Disorientation and short-term (several minutes) slowness after awakening are characteristic. Episodes of sleepy intoxication in some cases can be longer - up to 1 hour or more.
Episodes of sleepy intoxication are not accompanied by vegetative symptoms (tachycardia, tachypnea), hallucinations, fear, or circling around oneself.
Data from laboratory and functional studies. Polysomnography. Changes occur during deep sleep - non-REM-IV.
Differential diagnosis should be made with complex partial seizures, other parasomnias (for example, nightmares).
Sleepwalking (somnambulism) (ICSD 307.46-0)
The term “somnambulism” means a pathological condition characterized by sleepwalking and changes in behavior during deep sleep.
Clinical characteristics. The disease manifests mainly during puberty (Kavey et al, 1990) and ends in the postpubertal period (Cirignotta et al, 1983). It is also possible for the disease to develop in adults, however, in comparison with children, severe psychopathological disorders are observed in adults. Clinical manifestations of somnambulism have been well known since ancient times. The leading symptom is sleepwalking. Attempts to wake up a patient with somnambulism, as with other parasomnias, are futile and can lead to manifestations of aggressiveness. Sometimes aggression in patients with somnambulism can be observed spontaneously (Gottlieb et al, 1986). People around should be warned about the possible aggressive actions of patients and the undesirability of interrupting an attack by forcibly awakening. Sometimes sleepwalking becomes complex, which is manifested not only by wandering around the room, but also by leaving the house. The duration of episodes of somnambulism ranges from a few seconds to several minutes. Provoking factors are: stress, emotional disorders, taking various medications - neuroleptics, antidepressants, antihistamines, barbiturates (Niarahua, 1979), and sometimes lithium preparations (Charney et al, 1979).
Data from laboratory and functional studies. Attacks of somnambulism are observed during the deep non-REM-IV sleep phase (Blatt et al, 1991). A polysomnographic study reveals prolongation of slow-wave sleep phases, an increased frequency of incomplete awakenings, and hypersynchronous delta activity.
The differential diagnosis of somnambulism should be carried out, first of all, with psychomotor attacks of temporal and frontal localization. Psychomotor attacks are usually shorter, often accompanied by an aura and oroalimentary automatisms. In addition, it is fundamentally important to have a history of daytime paroxysms, which supports the diagnosis of “partial epilepsy.” Significant assistance in differential diagnosis is also provided by neuroradiological research methods - CT, NMR, positron emission tomography, which often detect structural brain damage in partial epilepsies. EEG video monitoring allows us to identify patterns characteristic of partial epilepsies.
Treatment. Regular sleep and strict control by others over the child’s behavior are necessary. Benzodiazepines have a satisfactory effect (Clement, 1970: Reich, Gutnik, 1980), as well as hypnosis (Hurwitz et al, 1991).
Nightmares (ICSD 307.46 1)
Nightmares are a pathological condition characterized by sudden awakening during deep sleep, screaming, autonomic disorders (tachycardia, tachypnea, redness of the skin, mydriasis) and changes in behavior accompanied by a pronounced feeling of fear.
Clinical characteristics. Nightmares occur primarily in childhood and disappear in adolescence. Boys are more often affected (Kramer, 1979). Paroxysm occurs in the first third of the night. The patient suddenly screams loudly, sits up in bed, there is disorientation and an expression of fear on his face. Sometimes the behavior of patients becomes panicky. Autonomic symptoms such as tachycardia and tachypnea are also typical. Clinical manifestations are more pronounced the longer the patient remains in a state of deep sleep. Attempts to calm a child during an attack are of little help. Children with nightmares usually have normal intelligence. There were no behavioral disturbances in the interictal period.
Data from laboratory and functional studies. Nightmares occur during the slow-wave sleep phase - non-REM-III-IV. The EEG shows a normal alpha rhythm.
Differential diagnosis should be made with nocturnal paroxysmal states of epileptic and non-epileptic origin. For the differential diagnosis of nightmares and epileptic paroxysms of frontotemporal localization, it is necessary to conduct an EEG study, which allows us to identify patterns typical of epilepsy. It is extremely difficult to clearly distinguish between nightmares and somnambulism. The transformation of nightmares into somnambulism, and vice versa, is often noted (Kales et al, 1980).
When differentially diagnosing nightmares with alpine slumbers, one should take into account the time of occurrence of paroxysms and some character traits. Alpine naps usually occur in the last third of the night, and the accompanying vegetative symptoms are moderate. During alpine slumbers, in comparison with nightmares, orientation is quickly restored in the post-attack period. It should also be noted that in some cases, patients with alpine drowsiness remember their night attacks.
Differential diagnosis should also be made with hypnoygic hallucinations in narcolepsy. However, unlike nightmares, hypnagogic hallucinations in narcolepsy occur during REM sleep.
Treatment. Benzodiazepines and tricyclic antidepressants have a satisfactory effect. Sometimes an evening dose of anti-depressants and antipsychotics is sufficient (Flemenbaum, 1976). Improved sleep hygiene is also necessary (Hauri, 1982).
Sleep disorders associated with disruption of the transition from sleep to wakefulness
Sleep disorders associated with disruption of the transition from sleep to wakefulness are a group of pathological conditions characterized by sleep disturbances as a result of rhythmic movements, startling when falling asleep, somnilokia, and calf muscle cramps.
Rhythmic movement sleep disorders (Nighttime rhythmic head shaking ICSD 3073)
Clinical characteristics. The main symptoms occur in the first 2 years of life. Stereotyped movements of the head and neck are typical, occurring immediately before falling asleep and persisting during light sleep
(Thorpy, Glovinsky, 1989). Various types of stereotypical movements are noted - head impacts, rotation, swinging to the sides, rolling the body. In adolescence, these disorders are sometimes observed in autism, minimal brain dysfunction, and “borderline” mental disorders (Snyder, 1987).
Data from laboratory and functional studies. A polysomnographic study records normal bioelectrical activity. There are no epileptic patterns.
Treatment. Effective therapy to correct these disorders has not been developed (Watanabe et al., 1980).
Jerks on falling asleep (ICSD 30747.2)
Clinical characteristics. Sudden short-term contractions of the muscles of the arms, legs, and sometimes the head that occur when falling asleep are typical. In this case, patients often experience sensations of falling, hypnagogic drowsiness, and illusions. These changes are not pathological and are observed in 60-70% of healthy people. In some cases, startles lead to partial awakening, which may interfere with falling asleep.
Data from laboratory and functional studies. A polysomnographic study reveals short, high-amplitude muscle twitches (myoclonus) at the moment of falling asleep, and partial awakenings (Broughton, 1988).
Differential diagnosis should be made with myoclonic epileptic syndromes and restless legs syndrome. It is also necessary to exclude organic and psychiatric diseases accompanied by similar symptoms.
Treatment. Benzodiazepines and L-DOPA preparations have a satisfactory effect. However, this therapy is indicated only for sleep disorders (Lund, Clarenbach, 1992).
Somnilokia (ICSD 307-47.3)
Clinical characteristics. The main clinical signs are sleep-speaking and screaming in sleep, which can be repeated several times during the night. Patients do not remember any episodes of sleep talk. Provoking factors are fever and stress. At the same time, other sleep disorders may occur, for example, somnambulism, nightmares, sleep apnea syndrome.
Data from laboratory and functional studies. Somnilokia can occur at any stage of sleep, but most often during REM sleep.
Differential diagnosis must be made with nocturnal paroxysms of both epileptic and non-epileptic origin, accompanied by verbalization. Treatment. No special therapy is required.
Nocturnal calf cramps (ICSD 729.82)
Clinical characteristics. Night cramps of the calf muscles are observed in children and adults. Familial cases have been described (Jacobsen et al, 1986). Typical are paroxysms of sudden awakening, accompanied by intense pain in the calf muscles. The attack continues for 30 minutes, then suddenly passes. Often, such paroxysms can be secondary and occur in a wide range of diseases: Parkinson’s disease, rheumatism, endocrine, neuromuscular and metabolic diseases.
Data from laboratory and functional studies. A polysomnographic EMG study reveals increased activity of the affected muscles.
Treatment. During an attack, calf massage, movement, warming are recommended (Saskin el A1, 1988), and sometimes taking magnesium and iron supplements (Lund, Claren-bach, 1992).
Parasomnias that occur during RKM sleep
Parasomnias that occur during the REM sleep phase include the following pathological conditions - alpine naps, sleep paralysis, REM sleep-dependent asystoles, behavior disorders in REM sleep.
Alpine Slumbers (ICSD 307.470)
Clinical characteristics. Alpine naps occur at the age of 3-5 years in ordinary children. Girls are more often affected (Kramer, 1979). Typical are sudden awakening, accompanied by severe fright, fear, and a feeling of threatening danger. Episodes are observed, as a rule, in the last third of the night. The content of the dream is remembered and can be clearly described. There are a number of factors that provoke the development of alpine naps. In children, alpine naps are most often provoked by psychogenic stress, sleep deprivation, and taking medications that suppress REM-COH (tricyclic antidepressants, MAO inhibitors).
The pathogenesis of alpine naps is not clear enough. In 60% of cases, alpine slumbers are associated with traumatic events in the anamnesis (Kals et al, 1980). Facio et al (1975) described alpine naps in 69% of Vietnam War veterans.
Data from laboratory and functional studies. A polysomnographic study reveals awakening in the REM sleep phase, tachycardia, and tachypnea.
Differential diagnosis should be made primarily with nightmares. Compared to alpine naps, nightmares occur upon awakening during the slow-wave sleep phase. The content of sleep during nightmares is usually fragmentary and not remembered.
Along with nightmares, alpine naps should be differentiated from behavioral disorders during REM sleep, which are characterized by motor phenomena and preservation of muscle tone during the REM sleep phase.
Treatment. In children, alpine naps pass spontaneously. For frequent, at least weekly episodes, psychotherapy is recommended. Among medications, L-DOPA and β-blockers have a positive effect.
Sleep paralysis (ICSD 780.56-2)
Clinical characteristics. Typical episodes of “sleep paralysis” are hypnagogic hallucinations, oneiric states. Both familial (Rushton, 1944) and sporadic cases (Hishikawa, 1976; Meier-Ewert, 1989) have been described.
Data from laboratory and functional studies. A polysomnographic study reveals depression of muscle tone, the beginning of the sleep cycle with the REM sleep phase (sleep onset REM) or fragmented REM sleep.
Differential diagnosis. The range of diseases with which a differential diagnosis should be made is quite wide and includes hysterical states, paroxysmal myoplegia, drop attacks of various etiologies. Treatment. Pathogenetic therapy has not been developed.
Painful erections during sleep (ICSD 780.563)
Clinical characteristics. Paroxysmal pain in the penile area during erection, observed during the REM sleep phase, is characteristic.
REM sleep - dependent asystole (ICSD 780.56-4)
Clinical characteristics. Cardiac arrest during REM sleep. During the day, patients may experience a feeling of heaviness in the chest.
Data from laboratory and functional studies. In a polysomnographic study during the REM sleep phase, asystoles lasting up to 2.5 seconds are noted (Guilleminault et al, 1984).
REM sleep behavior disorders (ICSD 780.59-0)
Clinical characteristics. The age of onset of the disease is variable, although there is a tendency for the disease to predominately occur in adults and even the elderly. The most typical symptoms of the disease are paroxysmal episodes of sudden awakening during the REM sleep phase, accompanied by screaming or crying, searching movements, and a feeling of stiffness. Sometimes attacks become more complex: patients jump out of bed, rush around the room, and in some cases leave the house. Often the behavior is aggressive. During the day, no naroxysmal disorders were observed. Both symptomatic and idiopathic forms have been described (Uchiyama et al, 1995). A symptom complex of behavioral disorders during REM sleep is often observed in some neurological diseases - Shy-Drager syndrome, Parkinson's disease, narcolepsy, encephalomyelitis, cerebral astrocytoma. It is also possible that this symptom complex may develop when taking alcohol or a number of medications (imipramine, amphetamine).
The pathogenesis is not clear enough. The relationship between the genesis of the disease and biochemical disorders in the metabolism of adrenaline and norepinephrine is discussed.
Data from laboratory and functional studies. A polysomnographic study 60-90 minutes after falling asleep during the REM sleep phase reveals increased motor activity. In this case, muscle tone, as a rule, does not change. There is also an increase in deep sleep and an increase in REM sleep phases. There are no associated autonomic reactions. After an attack, the patient can be quite easily awakened (Shondienst, 1995).
Differential diagnosis should be made with nightmares, somnambulism, epileptic paroxysms of frontal and temporal localization. Compared to behavior disorders during REM sleep, nightmares and somnambulism are observed mainly in children during the slow-wave sleep phase. Behavioral disorder during REM sleep differs from epileptic paroxysms in the “coupling” with REM-CHOM, the absence of an aura, impaired consciousness, and motor stereotypies.
Treatment. Clonazepam has a satisfactory effect.
Other parasomnias
According to the International Classification of Sleep Disorders, this group includes the following diseases and pathological conditions - bruxism, nocturnal enuresis, abnormal swallowing syndrome associated with sleep, nocturnal paroxysmal dystonia, sudden nocturnal death syndrome, including in children, lethal familial insomnia, primary snoring , sleep apnea in children, congenital central hypoventilation syndrome, benign myoclonus of newborns during sleep.
Bruxism (ICSD 306.8)
Clinical characteristics. The main symptoms are stereotypical teeth grinding and biting teeth during sleep. In the morning, the patient often complains of pain in the facial muscles, jaw joints, and pain in the neck (Lavigne et al, 1991). An objective examination often reveals abnormal teeth, malocclusion, and inflammation of the gums. According to the literature, about 90% of the population have had an episode of bruxism at least once in their lives, but only 5% have symptoms so severe that they require therapy. Provoking or trigger factors are often dental prosthetics and stress (Pingitore et al, 1991). Familial cases of bruxism have been described.
Data from laboratory and functional studies. A polysomnographic EMG study reveals increased activity of the jaw muscles, which is combined with the appearance of K-complexes and partial awakening. Bruxism occurs both during non-REM and REM sleep (Ware and Rugh, 1988).
Differential diagnosis. Diagnosis and differential diagnosis of bruxism usually does not present any difficulties (Glares, Rao, 1977). In some cases, the diagnosis of bruxism is mistakenly made in patients with epileptic paroxysms, who experience tongue bite during night attacks. The diagnosis of bruxism is supported by the lack of tongue bite and severe wear and tear of the teeth.
Treatment. The use of biofeedback methods is being discussed (Glares, Rao, 1977; Punch, Gale, 1980).
Nocturnal enuresis (ICSD 780.56-0)
Clinical characteristics. Nocturnal enuresis is repeated involuntary urination during sleep. There are primary and secondary nocturnal enuresis. With primary enuresis, urinary control is not acquired. With secondary enuresis, acquired control over urination is lost. Approximately 15% of boys and 10% of girls suffer from primary enuresis. Primary enuresis usually goes away on its own at puberty. Sometimes primary enuresis is combined with somnambulism and nightmares.
Data from laboratory and functional studies. A polysomnographic study reveals an increase in the duration of deep sleep. During non-REM sleep III-IV, non-specific body movements are noted; when sleep phases change, urination occurs, followed by a decrease in muscle tone (Mikkelsen et al, 1980).
Differential diagnosis. In differential diagnosis, it is necessary to exclude diseases such as diabetes mellitus and urinary tract infections (Mikkelsen, Rappaport, 1980; Schmitt, 1982).
Treatment. It is recommended to limit fluid intake in the evening. Among drugs, antidepressants, in particular imipramine, have a satisfactory effect (Mikkelsen et al, 1980). For enuresis caused by a urinary tract infection, the underlying disease should be treated. Automotive training and wearing special trousers with a built-in sound device during the day are also recommended. When urinating, the sound device is activated (De Leon and Sacks, 1972).
Abnormal Swallowing Syndrome Associated with Sleep (ICSD 780.566)
Clinical characteristics. The main manifestations are excessive, frequent swallowing movements, which contribute to coughing and a feeling of suffocation. Often the attack ends with awakening. Fear of another attack can cause another attack.
Data from laboratory and functional studies. Polysomnographic studies show an increased incidence of incomplete awakenings (Guilleminault et al, 1976).
Differential diagnosis. The most difficult differential diagnosis is bronchial asthma. Anamnestic information about the presence of allergic disorders is informative.
Hypnogenic paroxysmal dystonia (ICSD 780.59-1)
Clinical characteristics. Hypnogenic paroxysmal dystonia is a rare variant of paroxysmal dystonia (Lugaresi, Cirignotta, 1981). It occurs exclusively during the non-REM sleep stage and is triggered by awakening. Characteristic attacks are accompanied by choreoathetoid, ballistic movements and/or dyskinesias. The duration of attacks varies from several seconds to several minutes. Consciousness is always preserved. Familial cases have been described (Lee et al, 1985). Epilepsy is common in the pedigree (Sellal and Hirsch, 1991).
Data from laboratory and functional studies. A polysomnographic study reveals a disturbance in the sleep profile; multiple motor artifacts are recorded at the time of the attack. A number of researchers have discovered typical epileptic patterns when using depth electrodes in the frontotemporal areas (Mierkord et al, 1992). The question of the epileptic genesis of hypnogenic paroxysmal dystonia is debatable. Differential diagnosis should be made with pseudoepileptic (psychogenic) paroxysms, as well as with epileptic seizures of frontal and temporal localization. Pseudoepileptic paroxysms, in comparison with hypnogenic paroxysmal dystonia, are characterized by a longer duration of attacks, the presence of psychopathological character traits, and the absence of stereotypies.
In epileptic seizures of frontal and temporal localization, in contrast to hypnogenic paroxysmal dystonia, a disturbance of consciousness is often observed, and epileptic EEG patterns are also recorded.
Treatment. Clonazepam and carbamazepine have a satisfactory effect (Blank et al, 1993).
Sudden nocturnal death syndrome (ICSD 780.59-3)
Clinical characteristics. The syndrome is observed predominantly in young people, mainly of South Asian origin. Often these patients have a history of nightmares. The episode can occur at any stage of sleep and manifests itself with an attack of sudden suffocation, dyspnea. Attempts to wake the patient are unsuccessful. After resuscitation, ventricular flutter is determined. In the deceased patients, no changes were found in the heart that could explain sudden death.
Data from laboratory and functional studies. In a polysomographic study, pathology is not determined (Cobb et al, 1984; Lown, 1987).
Pediatric sleep apnea (ICSD 770.80)
Clinical characteristics. The term “childhood sleep apnea” refers to central or obstructive sleep apnea observed in children. There are 4 variants of this syndrome: apnea in prematurity, apparent life-threatening event, apnea in early childhood, obstructive sleep apnea syndrome.
Premature infants, especially those born before 37 weeks of gestation, have severe immaturity of the respiratory system. In this regard, this group of children often experience episodes of apnea during sleep. The occurrence of apnea in newborns is also due to decreased sensitivity to carbon dioxide. A risk factor for apnea in prematurity is gestational age. 50-80% of preterm infants born at 31 weeks of gestation have episodes of sleep apnea (Henderson Smart, 1985). In the development of an “obvious life-threatening episode” and apnea in young children, a decisive role is played by insufficient maturity of the central regulation of breathing (Brazy et al, 1987). Episodes of apnea in young children can be provoked by factors such as sudden tilting of the head, feeding, vomiting, and painful external stimuli.
Apnea in children manifests itself during sleep and is characterized by signs of hypoventilation (pallor of the skin or cyanosis, muscle hypotension). With frequently recurring episodes of apnea in children, hypertension of the pulmonary arterioles, right ventricular hypertrophy, and, in some cases, increased erythropoiesis in the liver may develop (Naeye, 1980).
Diagnosing sleep apnea in children is difficult. Compared to adults with sleep apnea, children do not have symptoms such as snoring or daytime fatigue.
Data from laboratory and functional studies. During a polysomnographic study, episodes of apnea are recorded, including a central phase lasting up to 20 seconds and an obstructive phase lasting about 10 seconds. Bradycardia and decreased oxygen saturation are also noted.
Treatment. Pathogenetic therapy has not been developed.
Congenital central hypoventilation syndrome (ICSD 770.81)
Clinical characteristics. From birth, shallow breathing is detected during sleep, sometimes with episodes of apnea (Fleming, 1980). Subsequently, due to dysmetabolic disorders caused by impaired respiratory function (hypoxia, hypercapnia), pulmonary hypertension, cor pulmonale, and brain hypoxia develop (Paton el al, 1989). As the disease progresses, cyanosis, generalized hypotension, and hyporeflexia occur. The prognosis is unfavorable.
Data from laboratory and functional studies. A polysomnographic study reveals decreased respiratory function against the background of hypercapnia and hypoxia. Sometimes episodes of apnea are recorded.
Treatment. Oxygen administration is recommended (Schlake el A1, 1991).
Sudden infant death syndrome (ICSD 798.0)
Frequency. 1 4:1000 births die as a result of sudden death (Byard, 1991). Sudden infant death syndrome most often occurs in children in the first year of life; 40% of all deaths in the first year of life are due to sudden infant death syndrome. After 3 months of life, the risk of developing sudden death syndrome decreases (Harrison, 1991).
The pathogenesis of sudden death syndrome is unclear. The role of dysfunction of brain stem structures is discussed (Stumer et al, 1990; Takahashima, Becker, 1991; Kinney et al, 1991). A number of researchers point to the significance of changes in cardiac function - prolongation of the QT interval, asymmetry in the maturation of sympathetic innervation of the right and left parts of the heart (Schwartz et al, 1982), reduced heart response to changes in heart rate in the QT phase (Sadeh et al, 1987). In the genesis of sudden death syndrome, according to James et al (1990), gastroesophageal reflux, intoxication, infections, incompetence of the immune system, hyperthermia due to high temperature in the room or excessively warm clothing may also play a role. The following risk factors for the development of sudden death syndrome in children have been identified (Hoppenbrouwers, Hodgman, 1982):
- prematurity (especially <1500 g);
- twins or triplets;
- the presence of sudden death syndrome in childhood among relatives;
- short intervals between births;
- smoking or maternal drug use (opiates, cocaine).
Socioeconomic factors also play a certain role, which undoubtedly positively correlate with the risk of sudden infant death syndrome. Lying on the baby's stomach also appears to be a risk factor. It has been noted that in southern Australia and the Netherlands, where children lie on their stomachs less, the risk of developing sudden death syndrome is lower.
Treatment. It is necessary to target and monitor children at risk. For respiratory motility disorders, breathing exercises are recommended. Avoid lying on the baby's stomach for long periods of time. For respiratory disorders, it is advisable to prescribe theophylline, and for hyperexcitability, phenobarbital.
Benign sleep myoclonus in newborns (ICSD 780.59-5)
Clinical characteristics. Debut - in early childhood. Asynchronous twitching of the limbs and trunk is typical during quiet sleep (Coulter, Alien, 1989).
Data from laboratory and functional studies. In a polysomnographic study, short (40-300 ms) asynchronous myoclonus is recorded (Resnick et al, 1986).
Lethal familial insomnia (ICSD 337.9)
Clinical characteristics. The age of onset is variable. Progressive insomnia is typical, starting with difficulty falling asleep, which after a few months leads to complete loss of sleep. Objectively, autonomic disorders are significantly pronounced - hypersalivation, anhidrosis, cardiopulmonary dysfunction. The disease progresses rapidly, after 2 years a coma develops, and patients die.
Data from laboratory and functional studies. A polysomnographic study reveals the absence of deep sleep and/or dissociated REM sleep, myoclonus.
Treatment is symptomatic.
<< Return to top
Classification
Depending on when paralysis occurs - during the transition to falling asleep or waking up, it has its own characteristics and is divided into 2 forms:
- When going to sleep, a person’s state enters the brain-conscious phase of REM sleep, whereas normally falling asleep should be accompanied by a cessation of vigilance a couple of moments before the onset of paralysis, which explains why people practically never remember how they fell asleep. The main feature of this form is the complete or partial preservation of consciousness and the feeling of the work pattern and structure of the body, its motor skills - the ability to move the fingers, but the time for the transition of thought to the execution of the movement takes a fairly long period of time.
- The second, more common form is awakening paralysis, which is accompanied by sensations such as suffocation, irrational fear, lack of air, false perception of body movements and disorientation in space . In practice, this can be expressed in the form of a false sensation of a rapid heartbeat and a turning over of the body, although the person is actually calm and immobilized. In attempts to wake up and in anticipation of the final awakening, people groan and twitch their limbs, which is caused by strong psycho-emotional impulses. Such sensations can lead to fear of death, falling into a lethargic sleep , nightmares and auditory hallucinations of someone’s voice, creating the impression of the presence of an outside force and hostile entities (humanoids, demons, etc.), most often perceived as otherworldly or alien forces. They are usually provoked by swelling of the arms and their raised position above the head. This pathological condition is promoted by sleeping on the stomach, with the head in the pillow, and is caused by the body's wake-up signals and lack of oxygen. The position of the body while sleeping, lying on its side, rarely causes sleep paralysis.
Causes of sleep paralysis
As a result of surveys, it was found that students and mentally ill people are more susceptible to sleep paralysis. Approximately a third of surveyed people in these categories experience a motor phenomenon while falling asleep, and in more rare cases, upon awakening.
Therefore, presumably, the causes of sleep paralysis may lie in irregular, fragmented and restless sleep and constant stress. The incidence in women is several percent higher than the incidence in men, but the difference is too small and does not make it possible to talk about the gender predisposition of the disease. Etiogenesis has not been fully and completely studied.
Risk factors
People at risk of experiencing muscle atonia when waking up or falling asleep include those who:
- suffer from migraines and poor, disturbed sleep;
- engage in activities that stimulate the nervous system in the evening;
- often fly on an airplane with time zone changes;
- sleep on their back;
- have a neurotic type of personality development;
- experiences increased levels of anxiety;
- work in shifts;
- suffer from hyperglycemia, arterial hypertension, anxiety disorder ;
- abuse alcohol and various medications;
- suffer from hypertension , idiopathic hypersomnia , sleep deprivation, narcolepsy , obstructive sleep apnea syndrome, Wilson-Konovalov disease ;
- have an increased level of dissociation and imaginative development with a belief in paranormal or supernatural phenomena;
- have a hereditary predisposition, since the likelihood of developing sleep paralysis due to family affinity has been established (presence of genes PER1, 2, 3, ABCC9, CACNA1C, ARNTL2, CLOCK, DBP).
How to induce sleep paralysis?
Since the state of sleep paralysis causes out-of-body experiences in some people, although this state can be frightening, people try to induce it on their own of their own free will. It is believed that this technique is used by Tibetan monks and shamans of various nations of the world, who are specially trained in techniques “how to control the phases of REM sleep and get into sleep paralysis.” They do not consider this phenomenon terrible and strive to get the sensation of floating above the body.
It is believed that you can enter a state of REM sleep while maintaining consciousness through the habit of sleeping on your back, interrupted fragmented sleep, many hours of meditation, shamanic rituals accompanied by special music and dancing, taking various herbal narcotic herbs and decoctions, and smoking them. Incense, light and music can also create a special atmosphere.
Symptoms of sleep paralysis and a detailed description of the phenomenon
In most cases, sleep paralysis is not a chronic disorder, and its occurrence is simply an unpleasant episode in the life of some people. But in 90% of cases the attacks are accompanied by an inexplicable animal fear. It is caused by the fact that a person loses control over the body and breathing, and also feels the appearance of something otherworldly.
Manifestations of paralysis, plots of conditions and stories of people who experienced stupor in a dream may differ. But for all cases almost identical symptoms are observed:
- inability to move for several seconds or minutes;
- understanding what is happening and remaining conscious;
- inability to utter a single word, call for help, or scream;
- a feeling of strong pressure in the chest, the touch of someone’s hand;
- acute premonition of impending death, strong animal fear;
- sound and visual hallucinations - steps, sighs, foreign presence;
- inability to think rationally and separate reality from fiction;
- pain in the chest area and muscles of the limbs.
Symptoms of sleep paralysis are more common in people who sleep on their backs. Pathology can occur in completely healthy individuals or be caused by narcolepsy, panic disorders, and post-traumatic syndromes.
Symptoms
The main manifestation of sleep paralysis is muscle atonia in the REM sleep phase, which occurs during falling asleep and waking up. In addition to immobility, most patients experience other symptoms:
- they see dreams - very vivid and quite unpleasant;
- they experience fear or, on the contrary, bliss, strange sensations of out-of-body experiences, it may seem to them as if the body is soaring, flying, accelerating, circling;
- while in a state of sleep, the brain is capable of activity and awareness of the surrounding world, control of breathing, etc.;
- chest pressure and difficulty breathing;
- pain;
- visual and auditory hallucinations, most often frightening, because atony is combined with a state of wakefulness;
- “flies” is another manifestation of illusions or hallucinations, expressed in the form of sound vibrations in the ears with increases in acoustic range and volume, smoothly turning into “white noise” and ringing in the ears, perhaps the predominance of a certain “squeak” that an ordinary person hears. a person is at rest in silence.
Section 2. Neurophysiological basis for the occurrence of the phenomenon
2.1. Mechanisms of transition to REM sleep
The structure of our sleep includes two alternating phases: the fast REM phase (rapid eye movement phase) and the slow NREM phase (non-rapid eye movement sleep, i.e. sleep without rapid eye movements). slow sleep). In this article, we will discuss the first of these phases in more detail, since it plays a key role in the occurrence of the phenomenon of sleep paralysis. This phase is also called the paradoxical phase, as it is characterized by increased brain activity, increased cerebral blood flow and increased serotonin levels, which is accompanied by increased blood pressure and heart rate; rapid and shallow breathing is noted, as well as intense movements of the eyeballs and contractions of facial muscles. Dreams usually occur during REM sleep.
One theory suggests that REM sleep is initiated by small clusters of cells located in the pons and medulla oblongata. The main mediators of these structures are acetylcholine and glutamate [10]. Groups of these cells are not arranged into a single “center” of REM sleep, but work as individual components of a wide network (Fig. 1) [11]. For example, activation of locus coeruleus (LCα) neurons leads to the development of muscle atonia; rapid eye movements are initiated by neurons of the reticular formation (RF), located near the abducens nucleus (PAb); muscle contractions occur when neurons in the nucleus giant cell are activated [11], [12].
Activation of a certain group of brain stem cells (
red ovals ) causes a change in the corresponding indicators of the body during the REM sleep phase, which are recorded in the form of curves (Fig. 1, right column). For example, EEG signs of cortical activation during REM sleep are realized due to the simultaneous activation of midbrain RF (MRF) neurons and magnocellular nucleus (MN) neurons in the medulla oblongata; generation of the theta rhythm in the hippocampus is initiated by neurons of the pontine oral reticular nucleus (PO); an increase in brain temperature and cyclical fluctuations in the parameters of the cardiorespiratory system are provided by neurons of the parabrachial nucleus (PBN).
Figure 1. Cellular-molecular-network model of the physiological mechanisms of REM sleep formation. Blue square: LC — neurons of the locus coeruleus, RN — neurons of the raphe nuclei; Green circle: GABA - local GABAergic neurons; Red ovals: MRF - neurons of the midbrain reticular formation, MN - neurons of the magnocellular nucleus of the medulla oblongata, LCα - neurons of the locus coeruleus alpha, PAb - neurons located near the abducens nucleus, PO - neurons of the oral reticular nucleus of the pons, PBN - neurons of the abrachial nucleus; C-PBL—neurons of the posterolateral peribrachial region, Sub C—neurons located under the locus coeruleus; Yellow rectangle: mPRF - medial pontine reticular formation; Red square: PPT - neurons of the pedunculopontine nucleus, LDT - neurons of the posterolateral part of the tegmentum; above the arrow: KR - kainate receptors; Yellow oval: Glutamate - glutamate [13]; Curves on the right (from top to bottom): EEG of a rat in the REM sleep phase, EMG of a rat in the REM sleep phase, EOG of a rat in the REM sleep phase, the theta rhythm of the hippocampus in the REM sleep phase, cyclic oscillations (BP - blood pressure, HR - heart rate, RESP - respiratory rate, BT - body temperature), PGO waves.
[eleven]
These groups of brainstem cells responsible for triggering REM signals are activated by increased release of cholinergic neurotransmitters, while the amount of aminergic neurotransmitters is either reduced or completely absent. Sources of acetylcholine (Fig. 1, red arrows) are cholinergic neurons of the pedunculopontine nucleus (PPT) and the posterolateral tegmentum (LDT). The sources of aminergic neurotransmitters (Fig. 1, blue arrows) are noradrenergic neurons of the locus coeruleus (LC) and serotonergic neurons of the raphe nucleus (RN). On the membrane of the former there are kainate receptors, which these neurons need to start working. A similar system is formed by both GABAergic and aminergic neurons.
The development of REM sleep begins with increased release of glutamate (Fig. 1, yellow oval); Consequently, the kainate receptors of cholinergic neurons (KR) are activated, which leads to their excitation and increases the release of acetylcholine in each of the REM sleep signal generators (Fig. 1, red arrows). Bidirectional communication of cholinergic neurons of the pedunculopontine nucleus (PPT) and a group of cells of the posterolateral tegmentum (LDT) with neurons of the medial pontine reticular formation (mPRF) is also triggered. Simultaneously with the described processes, local GABAergic cells are also activated (Fig. 1, green circle), which leads to active inhibition of aminergic neurons of the locus coeruleus and raphe nuclei and reduces or completely stops the release of aminergic neurotransmitters in the structures responsible for the generation of REM sleep.
The key role of the aminergic system is to stop its activity in time when cholinergic neurotransmitters are released. To further maintain episodes of REM sleep, increased acetylcholine release in mPRF neurons activates glutamatergic neurons, which continue to release glutamate in the PPT and LDT to maintain the activity of cholinergic neurons. Thus, cholinergic cells PPT and LDT and glutamatergic cells LC and RN form a positive feedback loop to maintain REM sleep cycles [11].
Another mechanism for the occurrence of REM sleep was proposed by Jouvet and Thompson and called it the “activation-synthesis hypothesis.” According to scientists, dreams - just as in the mechanism described above - are the result of nonspecific activation of neurons in the brainstem. But the analysis does not end there, and the signal is further transmitted to the cerebral cortex and subcortical formations for subsequent synthesis of the received information. Scientists have divided all nerve cells into two categories: cholinergic and monoaminergic REM sleep neurons. REM sleep is the result of the reciprocal interaction of these nerve cells [9].
However, the nerve centers for sleep regulation are located not only in the brainstem, but also in the diencephalon. The GABAergic “NREM sleep center” is located in the anterior hypothalamus, and the orexinergic neurons that ensure the process of turning on the “REM sleep center” are located in its middle part (Fig. 2).
Almost simultaneously, two groups of researchers from Japan and the USA discovered two amino acid sequences that were similar to each other, but named them differently [14]. It soon became clear that these were the same substance - the oligopeptides orexin A, containing 33 amino acid residues, and orexin B, consisting of 28 amino acids [15]. The protein proorexin is cleaved from preproorexin, from which orexins A and B are derived. The effect of the latter is determined by two G-protein-coupled metabotropic receptors. OX1R is a type 1 receptor that selectively binds only to orexin A, while OX2R is a type 2 receptor that is nonselective and binds to both orexins. The orexin A receptor is associated only with the Gq subclass of heterotrimeric G proteins, the orexin B receptor is associated with the Gq subclasses or Go and Gi proteins (Fig. 2) [16]. Orexinergic nerve cells interact with locus coeruleus neurons, inhibiting them [14].
Figure 2. Orexins and their receptors. LC - locus coeruleus, VTA - ventral tegmentum, VMN - ventromedial hypothalamus, DR - raphe nuclei, LDT/PPT - dorsolateral laterodorsal/pedunculopontine tegmentum, BST - bed nucleus of the stria terminalis, PVN - paraventricular hypothalamic nucleus, Arc - semicircular nucleus, TMN - tuberomammillary nucleus, DMH - dorsomedial nucleus, PVT - paraventricular thalamic nucleus.
[16]
2.2. How can disruption of the mechanisms of transition to REM sleep lead to SP?
Research by American scientists at the University of Pennsylvania has shown that the basis of SP is the perseveration of REM activity, that is, a violation of the switch from sleep to wakefulness [2].
- Perseveration (Latin perseveratio - “persistence”, “persistence”) - a stable repetition of something, in this case - REM activity.
During the REM phase of sleep, our brain systems are actively working, as we verified above, but the body remains motionless [6]. But sometimes during this period an awakening occurs, and if the brain structures do not have time to synchronize with each other, paralysis occurs [17]. At the molecular level, awakening is mediated by the following mechanisms. It is believed that the cholinergic and glutamatergic systems are mainly associated with the bioelectrical and behavioral manifestations of the awakening process [18]. The nuclei of the brainstem, responsible for excitation and containing acetylcholine, dopamine, serotonin or norepinephrine, activate the thalamus, hypothalamus, motor neurons of the spinal cord, forebrain and have an inhibitory effect on the ventrolateral preoptic area (GABA, galanin); The hypothalamic and thalamic excitatory centers activate the cortex and arousal-related areas in the basal forebrain and brainstem [19].
One of the most notable aspects of SP is vivid hypnogogic or hypnopompic hallucinations [1]. They can occur during a sudden awakening, along with visions of demonic images, a state of panic, and a feeling of the presence of strangers [20]. A possible explanation for this phenomenon may be that during REM sleep there is a decrease in the activity of the respiratory muscles; this is due to inhibition of motor neurons. During REM sleep, breathing becomes irregular, skeletal muscle hypotension occurs, which leads to a significant decrease in lung ventilation and tidal volume, which leads to excessive accumulation of carbon dioxide in the blood - hypercapnia - and a decrease in the amount of oxygen - hypoxia [21]. In addition, oligodendrocytes, the myelin-producing cells of the central nervous system, are selectively sensitive to hypoxia and sleep fragmentation [22].
- Hypnogic hallucinations are visual illusions that appear before falling asleep.
- Hypnopompic hallucinations are visual illusions of perception that appear after awakening.
A century ago, American neurologist Weir Mitchell described the state of “night paralysis” as follows: “The subject awakens and is aware of his surroundings, but cannot move his muscles; lying there, apparently still sleeping. He is really involved in the struggle for the movement, fraught with acute mental disorder; if he had time to move, the spell would have disappeared instantly” [23].
It is assumed that in addition to the secondary (and sometimes primary) sensory cortex, dysfunction in other areas - the premotor cortex, the cingulate cortex, the subcortical and cerebellar areas - also contributes to the occurrence of hallucinations. The disorder that causes hallucinations is almost always located in areas of the brain associated with sensory systems. It is assumed that compensatory overactivation of brain regions surrounding these pathways is also the cause of hallucinations [24]. However, within seconds to minutes of awakening, the perceptual, cognitive, and motor components of the sleep cycle are synchronized, hallucinations disappear, and mobility is restored when the person is fully awake.
The mechanisms of REM-on and REM-off systems block impulses arriving along incoming sensory fibers, supplying the cortex with internal stimuli that form the content of dreams. They also block the activity of motor neurons in the cortex, thereby immobilizing the dreamer [1].
Thus, when sleep paralysis occurs during a sudden unplanned awakening during REM sleep, eye movements remain unchanged, showing the same high activity, and sensory sensations are clear.
Tests and diagnostics
Old witch syndrome is most often identified during a conversation with a patient or a questionnaire. In this case, the patient has the ability to control eye movements and breathing, hallucinates and experiences suffocation.
At the moment, no types of tests similar to polysomnography have been developed to diagnose this type of parasomnia, but it has been assigned an ICD-10 code: G47.0 and the name “Disturbances in falling asleep and maintaining sleep, expressed in the form of complaints of unwanted and disturbing events and sensations during sleep." To diagnose pathology, a few repeated episodes that cause anxiety and fear are enough.
Prevention
It is believed that repeated episodes of muscle atony during falling asleep and waking up can be eliminated by following the rules of sleep hygiene:
- fall asleep and wake up at the same appointed time;
- take water procedures in preparation for bed;
- practice meditation and breathing exercises to relax in the evening;
- adhere to the normal amount of sleep typical for your age;
- choose a comfortable mattress and bed linen;
- ventilate the room before going to bed;
- worry about the room temperature – 18-20°C;
- Avoid drinking alcoholic and caffeinated drinks several hours before bedtime;
- Avoid falling asleep lying on your back or stomach.
Competition “Bio/Mol/Text”-2020/2021
This work was published in the “Free Topic” category of the “Bio/Mol/Text” competition 2020/2021.
The general partner of the competition is the annual biotechnology conference BiotechClub, organized by the international innovative biotechnology company BIOCAD.
The sponsor of the competition is SkyGen: a leading distributor of life science products on the Russian market.
Competition sponsor: the largest supplier of equipment, reagents and consumables for biological research and production.
"Book" sponsor of the competition - "Alpina Non-Fiction"
Imagine opening your eyes just before dawn, trying to roll over in bed, and suddenly realizing that you are completely paralyzed. Lying helplessly on your back and unable to scream for help, you notice sinister figures lurking in your bedroom. As they approach the bed, your heart begins to beat faster and you feel like you're suffocating. You hear a buzzing sound and feel electrical impulses throughout your body. After a moment, the visions disappear and you can move again. Horrified, you think about what just happened. The above experience is an episode of sleep paralysis accompanied by hypnopompic hallucinations [1]. This frightening description has been interpreted in various cultural contexts since the time of the ancient Greeks, with a variety of spiritual and supernatural explanations ranging from witchcraft and evil spirits to aliens [2], [3]. Modern medical explanations of SP are not so colorful, but they help us understand the problem much more deeply.
The artist Henry Fuseli dedicated a series of four paintings to this phenomenon - “Nightmare”. The embodiment of the nightmare is personified by the dissolute demon of the mythology of medieval legends - an incubus sitting on the chest of a young girl. The tone of the picture evokes a depressing feeling, plunging the observer into an atmosphere of hopelessness and horror, making one feel the full severity of the charming girl’s condition under the pressure of a “sleepy stupor.”
Diet for sleep paralysis
Diet for the nervous system
- Efficacy: therapeutic effect after 2 months
- Timing: constantly
- Cost of food: 1700-1800 rubles per week
Reducing stress, avoiding drugs, alcohol, excessive physical activity, and most importantly, proper diet can help reduce the risk of attacks of paralysis. It is important to strictly arrange meal times, choose a balanced menu, make breakfasts more filling and dinners lighter, and 3-4 hours before going to bed. It is recommended to enrich the diet with the following products that improve sleep quality:
- bananas;
- boiled eggs (1-2 per day);
- a handful of almonds for an afternoon snack or salad;
- seafood (at least 2 times a week);
- light fermented milk drinks (a glass of yogurt in the evening will improve the general condition of the body and give a blooming appearance);
- different types of cabbage and leafy greens should be included in both soups and salads on your plate every day;
- fresh berries are good if they complement morning oatmeal;
- honey, molasses and grapes are the best sweet substitutes.
When to see a doctor
Sleep paralysis rarely requires medical advice. Here are signs that you should still see a therapist or neurologist:
- sleep paralysis occurs regularly - once a week or month;
- because of this, you are afraid to go to bed or cannot get enough sleep;
- in addition to the main symptom, you constantly feel very sleepy during the day. Or have you had episodes when you suddenly fell asleep literally on the go.
The doctor will advise you on how to normalize your sleep. Most likely, his recommendations will relate to your lifestyle. However, in particularly difficult cases, a specialist may suggest taking a course of antidepressants. These drugs partially change the REM sleep phase. When treating sleep paralysis, they are prescribed in lower doses than for depression.