general information
According to statistics, at least every tenth person on the planet suffers from migraine.
Women get sick approximately twice as often as men. This is associated with cyclical hormonal changes during the menstrual cycle. Typically, the disease makes itself felt before the age of 30-35; cases of the pathology occurring in childhood have also been described.
The biomechanism of the development of the disease is not precisely known. There are several theories about the occurrence of pain and accompanying symptoms, the most popular of which is neurovascular. According to this point of view, migraine begins against the background of activation of the trigeminal nucleus, which first causes spasm and then dilation of cerebral vessels. As a result, the tissue around the arteries becomes swollen, which leads to pain. In addition, the pathological process is associated with impaired serotonin metabolism.
Some scientists believe that pain occurs solely against the background of a sharp spasm and subsequent relaxation of blood vessels, resulting in tissue swelling (vascular theory). It has been clearly proven that the risk of developing the disease is significantly higher in women, as well as in people whose parents or close relatives also suffered from migraine.
Make an appointment
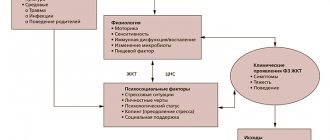
Migraine from a psychosomatic point of view
Probably each of you has heard the concept of psychosomatic illness. It gained great popularity and forever entered our culture and knowledge about man.
We are one whole, and our body is one of the components of our common self. Through it we feel the world, live and experience emotions. It also shapes us in different ways. Our first acquaintance with the outside world passes through touching and crying.
The body is involved in our experience and emotional life. It also “records” our emotional experiences from periods when we do not yet have conscious (verbal) memory. Through the body we also learn to influence our feelings, for example by breathing deeper or inhaling air.
It also happens that through the body we express what we cannot express in words, and what we have often long forgotten or hidden from ourselves.
Causes
Migraine occurs against the background of various external and internal causes (triggers), each of which can cause another attack:
- mental and psycho-emotional stress;
- constant severe stress;
- sleep disturbances, insufficient rest at night;
- chronic fatigue (mental and physical);
- smoking;
- previous head injuries (even many years ago);
- excessive physical activity for a particular person;
- hormonal surges: puberty, menstruation (“menstrual migraine”), pregnancy;
- consumption of foods containing tyramine (chocolate, coffee, citrus fruits, nuts, cheese, smoked meats);
- drinking alcohol, especially low-alcohol drinks;
- sharp fluctuations in atmospheric pressure, changes in air temperature;
- overstrain of the senses: sharp sound, bright light, strong unpleasant odor, etc.;
- staying in a hot or stuffy room, etc.
Each person has his own “dangerous” factors. Most of them can be calculated and, if possible, avoided in the future.
Symptoms
A migraine attack follows a standard scenario, consisting of several successive stages.
- Prodromal (initial) stage. A person’s mood begins to change, yawning and drowsiness appear, or, conversely, insomnia. Some report sensitivity to noise and bright light. Sometimes there is a slight numbness in one of the hands. For most patients, these symptoms are enough to know that a full-blown migraine attack is on the way. The duration of the prodromal stage ranges from several hours to several days; it is not present in all patients.
- Aura. Occurs against the background of cerebral vascular spasms. Most often it manifests itself in the form of visual disturbances (flashes in the form of spots, zigzags or lightning in front of the eyes, distortion of the contours of objects, loss of individual fields of vision). Less common are taste or hearing disorders, problems with coordination of movements, etc. Aura is not observed in all patients.
- Actually a migraine attack. In most cases, it manifests itself as a unilateral headache that is pulsating in nature. It starts with slight discomfort and gradually gains strength, becoming simply unbearable. Movements, changes in body position, bright lights and loud sounds intensify the sensations, which is why patients try to spend this time lying in a darkened room. Against the background of a headache, many patients report nausea, vomiting, soreness in the muscles of the neck and shoulders, nasal congestion, lacrimation, chills and even fever. The duration of the attack is individual and ranges from 2-3 hours to several days.
- Resolution stage. At this time, the headache goes away on its own or after taking medications. Many patients fall asleep at first, but within 24 hours after the attack they may feel weak, lethargic, dizzy, and depressed. Increased sensitivity to light, sounds and smells also does not go away immediately. Less common is the opposite type of resolution stage, in which patients note increased activity.
32nd city clinical clinic
Migraine has been known since ancient times. Many prominent people suffered from this disease: Julius Caesar, Beethoven, Darwin, Wagner, Chopin, Tchaikovsky, Freud, etc. Migraine is not a fatal disease, but in most cases it significantly disrupts the social adaptation and quality of life of patients. Approximately half of patients with migraine have a family history of headaches, but relatives do not always have classic migraine. Women get sick more often, or at least go to the doctor more often than men.
The pathogenesis of migraine is the subject of wide and lively debate. Many mechanisms of migraine headaches are not fully understood. For an attack to occur, the interaction of many factors, primarily neurogenic, vascular, and metabolic, is necessary.
Migraine is characterized by stereotypical attacks of pulsating headaches, often unilateral localization, mainly in the orbital-frontotemporal region, which is accompanied in most cases by nausea, sometimes vomiting, poor tolerance of bright light and loud sounds, drowsiness, and lethargy after the end of the attack.
It often turns out that a patient with migraine had a nonspecific paroxysmal headache in childhood. In addition, the history often contains indications of attacks of abdominal pain accompanied by vomiting. In adult patients, pain is unilateral only in 65% of cases. More often it begins in the frontotemporal region, then spreads to the entire half of the head. The pain is often throbbing, boring or deep. It is enhanced by external stimuli such as light and sound. The patient looks pale, the temporal artery is painful on palpation. The pain reaches its maximum relatively quickly, within one or several hours, and in 60% of cases is accompanied by nausea and vomiting. During an attack, the patient becomes hypersensitive to light and sounds and prefers to be in a quiet, darkened room. Sometimes he is also intolerant of odors. The side of pain in many patients changes very rarely, but the absolute constancy of the location should always raise suspicion of a symptomatic form of headache. Sometimes there is an unusual localization of pain: in the back of the head, neck. Autonomic manifestations are often observed: sweating, abdominal pain, diarrhea, tachycardia, dry mouth. After an attack, large amounts of urine are often released. The duration of the attack is several hours, and the frequency of attacks varies from several times a year to almost daily.
An attack can be provoked by atmospheric influences, as well as visual stimuli, menstruation, rest and prolonged stay in bed (migraine on weekends and holidays), as well as mental stress (increased responsibility, reports, conflicts).
In patients with migraine, attacks often stop during pregnancy and after menopause. Sometimes a provoking factor for migraine-like headaches is the use of drugs that suppress ovulation. If a woman first develops migraine due to the use of oral contraceptives, especially if it is accompanied by an aura, there is a risk that neurological symptoms will persist for a long time. This danger is even higher in smoking patients. In these cases, drugs that suppress ovulation should be replaced with other means of contraception. In some patients, the consumption of certain types of cheese is a provoking factor.
Clinical manifestations of migraine:
Distant warning signs are bad mood, irritability, general anxiety, lethargy, drowsiness, decreased performance, cravings for specific foods, such as sweets.
Aura – neurological symptoms, visual disturbances. In typical cases, the patient sees flashes of light and flickering zigzag lines. Sensory symptoms: tingling, crawling sensation, numbness in the fingers, spreading along the ulnar surface to the perioral area and to the tongue. There may also be speech disorders. The duration of the aura is from 4 to 60 minutes. Headache occurs no later than 60 minutes after the aura. The headache usually grows, throbbing in nature, usually in one half of the head, but can also be bilateral. In the final stage, the pain gradually decreases, weakness, lethargy, weakness, and drowsiness occur. After sleep, the state of health often returns to normal before the next attack occurs.
In differential terms, it is necessary to keep in mind the so-called danger signals that indicate other causes of headache:
- Sudden intense headache with a feeling of a “blow” in the occipital region, “spilled boiling water in the head” (subarachnoid hemorrhage).
- The appearance and increase of headaches when coughing, sneezing, after physical exertion, sexual activity, straining (increased intracranial pressure).
- Headache is the cause of night awakenings, intensifies with changes in the position of the head and body (tumor).
- The appearance of accompanying symptoms in the form of hiccups, nausea, vomiting in the morning; dizziness, which intensifies when changing the position of the head and body.
- Having half headaches for several years on one side.
The occurrence of cephalgia of a different nature, unusual for the patient: increasing headache over time: over hours - days (meningitis, encephalitis), weeks - months (tumor, etc.).
- Age onset of headache is 50 years and older.
The presence of the above symptoms indicates a structural headache. If they occur, a detailed neurological examination is necessary to exclude an organic process.
Complications of migraine.
- Status migraine is a series of severe attacks following each other, accompanied by repeated vomiting.
- Brain infarction. In some cases, during a migraine attack, a heart attack develops, which is often localized in the posterior parts of the brain. The diagnostic criteria for migraine infarction are the presence of migraine with aura, the appearance of focal neurological symptoms that persist for more than 3 days, sometimes 3 weeks or more.
- A migraine attack can transform into an epileptic seizure.
Migraine treatment should be selected individually, including two main areas: attack relief and interictal – preventive treatment. The main criterion is the frequency of attacks. The use of the latest methods in the treatment of migraine makes it possible to prevent exacerbations and improves the quality of life of both the patient and his family members.
The material was prepared by A.P. Oleshkevich, a neurologist (head of the department).
Types of pathology
Migraines are most often classified according to the presence of an aura and its type. The following types of disease are distinguished:
- classic migraine: before an attack of pain, a typical aura occurs with visual, auditory, olfactory and other disturbances;
- migraine without aura: symptoms appear suddenly against a background of relative well-being; the rest of the clinical picture is characteristic of the disease.
Depending on the predominant symptoms, the following types of migraine are distinguished:
- ocular (ophthalmic): accompanied by classic visual impairments: glare, flickering, flare in certain areas of the visual field;
- retinal: the disease manifests itself as complete or partial loss of vision in one eye due to impaired blood circulation in the vessels of the retina;
- ophthalmoplegic: manifested by double vision, visual distortions, drooping of the eyelid;
- basilar: accompanied by dizziness, ringing in the ears, unsteadiness when walking, blurred speech;
- hemiplegic: characterized by loss of sensation and impairment of motor function of one arm or arm and leg on one side;
- cervical: occurs against the background of impaired blood flow in the vertebral arteries and is accompanied by a very severe headache;
- aphasic: pain is accompanied by speech disorders, as with a stroke;
- abdominal: additionally manifests itself as severe pain throughout the abdomen, diarrhea, nausea and vomiting; this form is very common in children;
- “decapitated”: the patient does not feel a headache, as a rule, only visual disturbances are noted, while the prodromal period and aura occur typically.
Migraine status stands apart. This is a severe condition in which two or more attacks occur in a row with less than 4 hours between them. This type also includes pain that lasts for more than 3 days. Against the background of migraine status, the patient experiences repeated vomiting, which does not allow him to eat, drink, or take medications normally.
Migraine in women
Migraine is a disease that is significantly more common in the female population: the ratio of the prevalence of migraine among men and women of reproductive age is 1:2–1:3. Changes in hormonal status associated with menarche, pregnancy, lactation and menopause are often accompanied by changes in the nature and frequency of migraine attacks. Thus, female sex hormones determine strict correlations between headache frequency and the menstrual cycle.
Menstrual migraine
Menstrual migraine is a common form that occurs in more than 50% of migraine patients. Typically, menstrual migraine is characterized by more severe and prolonged attacks, lasting several days. This leads to significant maladaptation of young women: they cannot go to work or their performance is significantly reduced, they cannot devote enough time to family and personal interests. However, menstrual migraine is underdiagnosed by neurologists, gynecologists, and general practitioners. This is largely due to the fact that the patients themselves do not complain of headaches, as they consider it a manifestation of premenstrual tension syndrome.
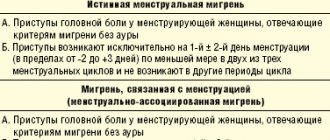
The International Classification of Headaches distinguishes two types of menstrual migraine - true menstrual migraine without aura and migraine without aura associated with menstruation (Table). True menstrual migraine is observed in 7–19% of patients [9, 10].
The menstrual cycle and migraine
Normally, hormonal fluctuations associated with the menstrual cycle are regulated by the activity of the hypothalamic-pituitary-ovarian axis. Thus, the influence of the activity of the hypothalamus on the activity of the pituitary gland is carried out through gonadotropin-releasing hormone (GHR), the secretion of which is regulated by various neurohormonal substances - norepinephrine, serotonin, dopamine, endorphins, corticotropin-releasing hormone (CRH), corticosteroids. It is known that norepinephrine has a stimulating effect in this case, and opioids, corticosteroids and CRH suppress the secretion of GnRH. GnRH, in turn, regulates the secretion of pituitary gonadotropins - follicle-stimulating and luteinizing hormones, which are necessary for the secretion of hormones by the sex glands. Androgens and estrogens are also involved in the regulation of gonadotropin secretion, providing a feedback mechanism. The development of menstrual migraine is associated with two factors:
- with an increase in the content of prostaglandins in the endometrium and systemic circulation in the luteal phase of the cycle with a subsequent increase during menstruation;
- with a sharp drop in estrogen and progesterone levels in the late luteal phase of the cycle.
A comparison of the profile of fluctuations in the level of hormones that determine the normal menstrual cycle and the onset of menstrual migraine convincingly proves that a drop in estrogen levels in the late luteal phase of the cycle is, if not the cause, then a powerful provocateur of the development of a migraine attack. This clinical observation is supported by experimental data. It was shown that the administration of progesterone in the premenstrual period delayed the onset of menstruation in women, but did not affect the occurrence of a migraine attack; on the contrary, the administration of estrogen did not affect the timing of the onset of menstruation, but significantly delayed the onset of a migraine attack [17, 18]. Thus, the key factor that ensures the onset of a menstrual migraine attack is a drop in estrogen levels.
A series of experimental studies have shown that both progesterone and estrogen can influence cortical hyperexcitability, the main pathophysiological mechanism of migraine, through activating neurotransmitters (glutamate) and inhibitory neurotransmitters (gamma-aminobutyric acid (GABA)). In particular, estradiol has been shown to increase the activity of N-methyl-D-aspartate (NMDA) glutamate receptors and also reduce the synthesis of GABA [11]. Progesterone, on the contrary, has an inhibitory effect, potentiating GABA-mediated neurotransmission. Both estrogen and progesterone influence cortical spreading depression (SCD), which underlies the development of migraine attacks. Exposure to both hormones increases both the frequency and amplitude of RCD, whereas exposure to estrogen alone lowers the threshold for the occurrence of RCD. It is assumed that estrogen affects the activity of genes encoding molecules of substances that trigger and support the development of RCD [20].
Moreover, the effects of ovarian steroids on the trigeminovascular system have been shown. The fall in estradiol in the late luteal phase of the cycle leads to a significant increase in the expression of neuropeptide Y, which modulates both the conduction of pain impulses and vascular tone. A sharp change in the activity of neuropeptide Y, associated with a drop in estrogen levels, can trigger a migraine attack [13]. On the other hand, high estrogen levels correlate with higher pain tolerance. Thus, the administration of estradiol and progesterone to female rats after ovarectomy demonstrates a significant increase in pain thresholds in response to electrical stimulation [4]. The presence of a dense network of estrogen receptors in the cerebral cortex, limbic system, hypothalamus and other formations involved in the pathogenesis of migraine attacks: periaqueductal gray matter, monoaminergic nuclei and trigeminal nucleus of the brainstem, which determines the regulatory influence of estrogens on genomic, intracellular signaling and other processes of neuroplasticity. The stimulating effects of estrogens on the formation of growth factors (neurotrophins), primarily the brain-derived neurotrophic factor BDNF, are well known.
Estradiol has a modulating effect on neuronal excitability, changing the plastic properties of axon terminals and receptors. In particular, the administration of estradiol to experimental female rats is accompanied by an increase in the density of the spiny apparatus on the lateral branches of the apical dendrites of CA1 pyramidal cells of the hippocampus, populated by NMDA receptors, which increases the level of glutamatergic activity [1, 2]. Estradiol has the ability to activate glutamatergic transmission through allosteric stimulation of NMDA receptors. In addition, estradiol reduces the neuroinhibitory effect of GABA by inhibiting the activity of glutamate decarboxylase. Multiple effects of estrogen within the serotonergic system are known: an activating effect on the synthesis of serotonin and an inhibitory effect on its enzymatic metabolism [3].
These data are confirmed by clinical observations, where pain perception was studied in women with chronic pain syndromes over several menstrual cycles. A significant increase in pain perception was obtained in the first five days compared to other days of the cycle [6]. Healthy women also experience decreased pain thresholds during the premenstrual and menstrual phases of the cycle [14].
Clinical picture of menstrual migraine
Menstrual migraine is characterized by the development of migraine attacks, most often without aura, characterized by a duration of 4–72 hours (untreated), the presence of two of the following characteristics: unilateral localization, pulsating nature, moderate to severe pain intensity, worsening of headache after normal physical activity (for example, walking), as well as one of the accompanying symptoms (nausea and/or vomiting, sensitivity to light or sound). To make a diagnosis of migraine, at least five such attacks are required, as well as the absence of other causes causing these disorders.
In outpatient settings where time is a concern, practitioners may use a menstrual migraine screening questionnaire to assist in diagnosis. The patient is asked three questions:
- Do you have headaches associated with your menstrual cycle (occurring between two days before and three days after your period) most of your menstrual cycles?
- Are your cycle-related headaches significantly worse than usual?
- When you develop headaches related to your menstrual cycle, do lights irritate you more than usual?
Menstrual migraine can be suspected if the answers to the first question and one of the subsequent ones are positive. The sensitivity of this test is 0.94, specificity is 0.74 [19].
Unlike migraine not associated with menstruation, menstrual migraine is characterized by greater severity of attacks, longer duration, greater maladaptation and resistance to standard therapy.
Management of patients with menstrual migraine
A feature of the management of patients with menstrual migraine is the extreme importance of keeping a headache diary. The purpose of keeping a diary is to establish a connection between the development of migraine attacks and the onset of menstruation, to identify the frequency of attacks, and to determine the pattern of prescribing preventive treatment. For three months, the patient should fill in the diary for the days of menstruation (for example, with the symbol “0”), the days of migraine headache (for example, with the symbol “X”), the days of non-migraine headache (for example, with the symbol “+”) (Fig.).
Treatment of patients with menstrual migraine consists of pharmacological and non-pharmacological methods and includes two areas - relief of attacks and their prevention. Relief of an attack of menstrual migraine is carried out according to the same principles as relief of an attack of non-menstrual migraine. To relieve an attack, drugs from the following pharmacological groups can be used:
- Nonsteroidal anti-inflammatory drugs (NSAIDs): ibuprofen (400 mg), acetylsalecylic acid (Aspirin) (1000 mg), diclofenac (25–50 mg)). In the presence of nausea and/or vomiting, as well as to enhance the effect of NSAIDs, it is recommended to combine them with antiemetics (metoclopramide (10 mg), domperidone (10 mg)).
- Ergotamine preparations (Sincapton, Dihydrergot).
- Triptans are specific anti-migraine drugs, agonists of 5HT1B/1D serotonin receptors (sumatriptan (100 mg), zolmitriptan (2.5 mg), eletriptan (40 mg)).
When selecting a drug, the following recommendations must be taken into account: analgesics and NSAIDs should be used for moderate attacks, no more than 10 days a month. If drugs in this group do not stop the attack completely, then it is necessary to prescribe triptans or ergotamine drugs. It is necessary to avoid taking drugs from the group of combined analgesics, especially those containing opiates, barbiturates, and caffeine, since taking these drugs significantly increases the risk of developing drug-induced or abuse headaches. Numerous studies have shown that triptans are most effective for relieving menstrual migraines. It is necessary to recommend that the patient use drugs in an adequate dose and at the beginning of the attack, when the headache has not reached its maximum [3].
Prevention of menstrual migraine
Standard preventive pharmacotherapy can be used in patients with menstrual migraine in cases where there are also frequent attacks not associated with menstruation, as well as in cases of resistance. The following drugs can be prescribed: topiramate (100 mg/day), amitriptyline (100 mg/day), propranolol (40–80 mg/day), verapamil (40–80 mg/day). In addition to standard therapy, magnesium preparations (360 mg/day) can be used to prevent menstrual migraine.
Another form of prevention for menstrual migraines is hormone therapy. The effectiveness of combined oral contraceptives (COCs) and estrogen replacement therapy (ERT) is discussed. The use of COCs is most suitable for women who need contraception, as well as patients with heavy bleeding, severe dysmenorrhea, and endometriosis. It must be remembered that prescribing COCs to patients with migraine with aura increases the risk of stroke, therefore, before starting hormonal therapy, it is necessary not only to diagnose the form of migraine, but also to make sure that there are no other risk factors for stroke, and that the patient is not a smoker. As a rule, monophasic drugs containing 35 mg or less ethinyl estradiol are used (in most low-dose COCs, the estradiol content ranges from 20 to 35 mg). Patients who do not require contraception are prescribed low-dose estrogen at a dose of 0.9 mg/day, which can be in either tablet or transdermal form [7, 8].
Since with menstrual migraine it is almost possible to accurately predict the onset of the next attack, such a direction of therapy has appeared as short-term prophylaxis, which is prescribed two days before the expected menstruation for 5-7 days of daily use. For the purpose of short-term prevention, drugs of several pharmacological groups are used: NSAIDs, estrogen-containing drugs, triptans.
Non-pharmacological methods of treating menstrual migraine include psychotherapy (cognitive behavioral therapy, relaxation techniques, feedback), patient education, correction of risk factors (diet, sleep hygiene, external factors, increasing stress resistance). Various methods of physiotherapy can be used - acupuncture, therapeutic exercises, massage. General recommendations may be the choice of a qualified specialist to carry out non-drug treatment, while the patient must be motivated to carry out such therapy; these methods can be used as basic methods or in addition to medication.
Pregnancy, lactation and migraine
According to clinical observations, 60–70% of women suffering from migraine note a significant improvement in the course of the disease during pregnancy, especially in the second and third trimesters, which is apparently associated with stabilization of estrogen synthesis. In a menstruating woman, the corpus luteum synthesizes progesterone and estradiol for 14 days. At 10–12 weeks of pregnancy, the placenta secretes progesterone and estradiol in concentrations sufficient to support pregnancy. There is a clear relationship between the increase in estrogen levels during pregnancy and a decrease in the frequency of attacks: in the first trimester, a decrease in migraine attacks is observed in 47% of patients, in the second trimester - in 83%, in the third - in 87%. Complete remission occurs in 11% of patients in the first trimester, in 53% in the second and in 79% in the third [15]. It should be noted that this pattern is typical for migraine without aura and does not apply to migraine with aura [5].
For practicing physicians, the question is always important what medications for the prevention and relief of migraine attacks can be recommended to patients with migraine during pregnancy and lactation. When selecting therapy, it is always necessary to remember that any prescribed pharmacological drug (with the exception of iron and folic acid supplements) may carry a potential risk for the fetus and newborn. However, there is evidence of the relative safety of low therapeutic doses of the following drugs:
- in the first trimester: paracetamol, ibuprofen, Aspirin, domperidone, metoclopramide, propranolol;
- in the second trimester: paracetamol, ibuprofen, aspirin, domperidone, metoclopramide, propranolol, amitriptyline, verapamil;
- in the third trimester: paracetamol, domperidone, metoclopramide, propranolol, verapamil;
- during lactation: paracetamol, ibuprofen, domperidone, metoclopramide, propranolol, verapamil.
When managing patients with migraine during pregnancy and lactation, the emphasis should be placed, first of all, on non-drug treatment: patient education with elements of psychotherapy, control of provocateurs, adherence to diet, sleep, rest and physical activity.
Migraine and menopause
During the perimenopausal period, most migraine patients also experience a change in the course of their migraine. During menopause, the secretion of progesterone and estradiol by the ovaries stops, and a period of hormonal stabilization begins [16]. In 67% of patients, the frequency of migraine attacks decreases by half or more, in 9% the frequency of attacks increases, in 24% the pattern of migraine does not change [12]. Treatment of migraine during the perimenopausal period follows the same principles as migraine in general, with the exception of the possibility of prescribing hormone replacement therapy.
Literature
- Tabeeva G.R. Menstrual migraine // Ross. honey. magazine 2008, vol. 16, no. 4, p. 195–199.
- Tabeeva G.R. Gromova S.A. Estrogens and migraine // Neurological journal. 2009. No. 5, p. 45–53.
- Tabeeva G. R. Menstrual migraine // Materials of the All-Russian scientific and practical conference with international participation “Headache 2007”. pp. 19–30.
For the rest of the bibliography, please contact the editor.
Yu. E. Azimova , Candidate of Medical Sciences G. R. Tabeeva , Doctor of Medical Sciences, Professor
First Moscow State Medical University named after. I. I. Sechenova , Moscow
Contact information for authors for correspondence
Diagnostics
The patient's headache has characteristic features that immediately suggest a migraine. For diagnosis, the doctor uses the following methods:
- collecting complaints and medical history to determine the nature of the pain; special attention is paid to: the time of onset and end of the attack;
- provoking factors;
- nature of pain;
- the absence or presence of an aura, its symptoms;
- well-being after an attack;
If necessary, additional examinations and consultations with specialists are prescribed. The diagnosis of migraine is made by exclusion when no other causes of headache have been identified.
Make an appointment
Treatment
Migraine treatment is divided into two areas:
- relief of the patient’s condition during an attack;
- preventing the occurrence of new attacks.
Help during a seizure
At the first signs of an impending migraine attack, it is necessary to eliminate as quickly as possible all factors that can increase the pain:
- turn off the lights and TV, close the curtains;
- eliminate sources of extraneous sounds as much as possible;
- provide access to fresh, cool air;
- go to bed.
To prevent and relieve immediate pain attacks, painkillers of various groups are used:
- analgesics and non-steroidal anti-inflammatory drugs (analgin, ibuprofen, indomethacin and their analogs): used for mild attacks that do not affect a person’s daily life;
- combination drugs (codeine, tempalgin, solpadeine): prescribed for moderate attacks that have little effect on life activity;
- triptan drugs (amigrenin, sumamigren, zomig and others) are used if attacks interfere with normal life;
- hormonal drugs (dexamethasone): used for severe and prolonged migraines in combination with other medications.
Additionally, antiemetics (metoclopramide, cerucal) can be used.
Home remedies to prevent a migraine attack are used as an addition to the main therapy. Many patients benefit from:
- cold compress on forehead;
- rubbing essential oils into the temple area;
- infusion of chamomile, mint, lemon balm, lavender and other herbs that promote relaxation;
- acupressure on acupuncture points: at the base of the skull, between the eyebrows in the hollow above the bridge of the nose, on the back of the foot (the hollow between the first and second toes).
It is important to remember that these remedies do not replace primary therapy.
Treatment between attacks
Preventing the occurrence of attacks is no less important than relieving pain and nausea. Currently, various groups of drugs are used:
- beta-blockers (propranolol and drugs based on it);
- antidepressants (venlafaxine, milnacipran, etc.): have a good effect in the treatment of chronic pain, and also reduce the manifestations of depression characteristic of patients with frequent attacks;
- anticonvulsants (Depakine, topiramate): well tolerated and significantly reduce the frequency of exacerbations.
Medicines are used:
- if exacerbations occur more than 2 times a month;
- if attacks last more than 48 hours;
- with severe headache or complications.
In other cases, general preventive measures are sufficient.
Menstrual migraine: a modern view of the problem
There is an obvious relationship between the menstrual cycle and migraines. If before puberty the prevalence of migraine is the same among boys and girls, then after puberty it is higher among girls compared to boys. According to epidemiological studies, 50–70% of women report the occurrence of migraine during certain phases of the menstrual cycle. In 14% of women, migraines develop exclusively during menstruation. This connection is so important that the International Classification of Headache III (2013) identified working criteria for menstrual migraine (Table 1) [8]. According to the criteria, menstruation is defined as endometrial bleeding resulting from a normal menstrual cycle or the withdrawal of exogenous progestogens used for contraception or hormone replacement therapy. The first day of menstruation is day 1, the previous day is day 1, the next day is day 2 (day 0 is not provided). According to the classification, menstrual migraine is divided into “pure” menstrual migraine, in which attacks occur exclusively during the perimenstrual period, and menstrually associated migraine, in which attacks occur in the perimenstrual period, but can also develop in another phase of the cycle.
Pathophysiology of menstrual migraine
Data from basic research conducted in recent years have provided much insight into the pathophysiology of menstrual migraine. Sex hormones (estrogen, progesterone, testosterone) significantly influence brain function. Estrogens can modulate neuronal activity through estrogen receptors, which are widely present in the central nervous system (CNS), especially in the hypothalamus. Estradiol is synthesized in neurons of various areas of the brain that are involved in the pathogenesis of migraine. Thus, the level of estrogen is increased in the area of the thalamus, which has increased sensitivity to painful stimuli during migraine, the nucleus accumbens, which regulates the provision of the mechanism of emotional reinforcement, and the amygdala, which is involved in the development of anxiety and fear. By modulating the activity of these areas, estrogens can cause migraine symptoms such as allodynia, mood changes, and eating disorders. In addition, serotonin neurons in the midbrain, which have projections to the frontal lobes, limbic, diencephalic regions, and spinal cord and regulate both mood and pain, contain receptors for both estrogen and progesterone [14]. Polymorphisms of the estrogen gene ESR-1 594G>A and 325C>G increase the risk of migraine by 40-60%, and polymorphisms CYP19A1 rs10046 and CYP19A1 rs4646 of aromatase, which catalyzes the synthesis of estrogens, increase and decrease the risk of migraine, respectively. Progesterone is also widely present in the central nervous system and appears to have the opposite effects of estrogen. Thus, progesterone has an anticonvulsant effect. Testosterone is thought to have anti-migraine activity. Thus, synthetic testosterone derivatives improve the course of migraine in both men and women, apparently through the suppression of spreading cortical depression. In addition, the prevalence of migraine is higher among homosexual men, who have lower testosterone levels, compared to heterosexual men (15.5% and 7.2%, respectively). Research on sex hormones in migraine is of undoubted interest. Thus, in patients with “pure” menstrual migraine, compared with healthy individuals, there is an increase in the level of estrogen and progesterone in all phases of the menstrual cycle, especially in the luteal phase. Based on these data, it can be assumed that migraine involves dysfunction of the hypothalamus, which not only produces sex hormones and cortisol, but also regulates circadian rhythms. This is confirmed by a recent neuroimaging study by A. May, which showed that the “generator” of a migraine attack is dysfunction of the hypothalamus and its connections with subcortical and brainstem structures. How might sex hormones be associated with a migraine attack? The hypothalamus produces gonadotropin releasing hormone, which is released at regular intervals (Fig. 1). The frequency of gonadotropin releasing hormone release is higher during the follicular phase and the period of ovulation, while the greatest fluctuations in the level of this hormone are observed in the luteal phase. Estrogen regulates the release of gonadotropin releasing hormone according to the principle of negative feedback. Gonadotropin-releasing hormone regulates hormonal fluctuations during the cycle - the peak of estrogen in the late follicular phase and the peak of progesterone in the mid-luteal phase through increases in luteinizing and follicle-stimulating hormone levels at mid-cycle (day 14). The levels of sex hormones (estrogen and progesterone), as well as their releasing factors - luteinizing and follicle-stimulating hormones, fall by the 28th day of the cycle (before the onset of menstruation) (see Fig. 1). Further, in the next 7 days, estrogen and progesterone are at a stable low level, while from the 14th to the 28th day of the cycle, hormone levels change in waves. These wave-like fluctuations of sex hormones in the mid-luteal phase lead to increased neuronal excitability. Neuronal excitability increases during estrogen peaks - ovulatory and mid-luteal phase. Estrogens are able to influence the conduction of pain at all levels: at the level of the dura mater, trigeminal nerve, trigeminal ganglion, trigeminal nucleus, thalamus, cortical systems, as well as descending modulating systems. Data from preclinical studies indicate that estrogens play an important role in regulating the sensitization of trigeminal neurons through direct activation of calcitonin gene-related peptide. In a study by B. Barbosa Mde et al. pain sensitivity thresholds were studied in women in different phases of the menstrual cycle (menstrual, follicular, ovulatory, luteal, premenstrual). The lowest pain thresholds were observed in the premenstrual phase. Another factor determining the development and clinical features of menstrual migraine is dysfunction of higher pain perception centers. N. Maleki et al. Using functional neuroimaging, it was shown that women with migraine have damage to the parietal cortex (precuneus) and insula, compared with men with the same clinical picture of migraine. Given that sex hormones can damage neuronal circuits that regulate emotions, it can be assumed that different responses to painful stimuli in men and women are associated precisely with damage to these neuronal circuits.
Clinical picture of menstrual migraine
Menstrual migraine has clinical features. According to the analysis of diaries, most often in most patients a migraine attack occurs on the 2nd–3rd days of menstruation. Both population-based and clinical studies show that attacks of menstrual and menstrually-associated migraine are more intense, longer lasting, more often accompanied by nausea and vomiting, are more maladaptive in patients and respond worse to treatment. Attacks that occur 2 days before the onset of menstruation are with the highest level of intensity. The likelihood of their higher intensity is 2.1 times higher than that of attacks that develop in the first 3 days of menstruation, and 3.4 times higher than that of migraine attacks that occur in other phases of the cycle.
Treatment of menstrual migraine
Treatment of menstrual migraine consists of relief of attacks and prevention. To relieve menstrual migraine, the same drugs can be used as for non-menstrual migraine, but there are certain features. Since attacks are much more severe and respond less well to therapy, it is recommended to start therapy immediately with triptans. Sumatriptan, zolmitriptan, olmotriptan, rizatriptan, naratriptan have a proven effect in relieving an attack of menstrual migraine. The effects of zolmitriptan have been the most studied. Thus, a randomized, prospective, parallel, double-blind, placebo-controlled study included 579 patients. Relief or significant regression of headache 2 hours after administration was observed in 48% of patients taking zolmitriptan and 27% of patients taking placebo (p<0.0001). In this study, zolmitriptan was superior to placebo within 30 minutes of dosing. Preventive therapy for menstrual migraine can be carried out according to the same rules as for non-menstrual migraine, or can be short-term, i.e., prescribed only during the perimenstrual period. Short-term prophylaxis is more appropriate for true menstrual migraine and is considered in cases where triptans are ineffective in relieving attacks. The drug for short-term prophylaxis is prescribed 2-3 days before the planned onset of menstruation for 5-6 days. Naproxen was effective in a small open-label study, but showed no benefit over placebo in a double-blind, placebo-controlled study. Several triptans have been shown to be effective: sumatriptan, zolmitriptan, naratriptan and frovatriptan. The most convincing study was with zolmitriptan (Fig. 2). Thus, when taking 2.5 mg of zolmitriptan 3 times a day, a reduction in menstrual migraine attacks by half or more occurred in 58.6% of patients, and when taking 2.5 mg of zolmitriptan 2 times a day - in 54.7%. Also, when taking zolmitriptan, there was a decrease in the number of menstrual migraine attacks in three consecutive menstrual cycles (Fig. 3). Currently, patients with menstrual migraine may be recommended the available Russian drug Migrepam. For short-term prevention, estradiol (transdermal gel) at a dose of 1.5 mg, prescribed 2 days before the start of the planned menstruation for 7 days, can also be used. There is evidence of the effectiveness of taking oral magnesium supplements from the 15th day until the end of menstruation. If patients have menstrually associated migraine or irregular cycles, it is better to use constant preventive therapy with beta blockers, anticonvulsants, and antidepressants. For menstrual migraine, constant prevention with hormonal drugs is also possible. Thus, the use of transdermal contraceptives for 84 days reduced the number of days with menstrual migraine.
The problem of organizing care for patients with menstrual migraine
Patients with menstrual migraine face insufficient competence of gynecologists regarding migraine and insufficient competence of neurologists regarding hormonal therapy. The selection of hormonal therapy should be carried out by a gynecologist, taking into account all the characteristics of the patient, and migraine therapy should be prescribed by a neurologist. In addition, 74% of patients with menstrual migraine have concomitant gynecological pathology and need specialist consultation. In 2012, a specialized menstrual migraine clinic was established in Denmark. Collaborative management of patients by neurologists and gynecologists has been shown to improve the quality of their care. Thus, the number of days with migraine decreases from 6 to 3.83 days, and the quality of life improves. This approach to the treatment of menstrual migraine can be considered the “gold standard”.
Azimova Yu. E. (University Headache Clinic, Moscow)
Prevention
Prevention of migraine attacks is not only properly selected drug therapy, but also correction of the patient’s lifestyle. Doctors recommend:
- normalize sleep: for the normal functioning of the body, at least 8 hours of night sleep every day are required;
- minimize the consumption of foods that can cause an attack, especially chocolate, spices, and alcoholic beverages;
- eliminate smoking;
- adhere to a balanced diet with a mandatory breakfast and intervals between meals of no more than 5 hours;
- observe the drinking regime and consume at least 1.5-2 liters of clean water per day; in hot weather this amount can reach 2.5-3 liters;
- establish a work and rest schedule, avoid mental and physical fatigue;
- reduce stress levels as much as possible;
- make a habit of light or moderate physical activity: swimming, walking, cycling, yoga, Pilates;
- promptly identify and treat chronic diseases, especially osteochondrosis of the cervical spine, atherosclerosis and other pathologies that contribute to the deterioration of blood flow in the brain.
Regular health resort treatment of a restorative nature and tourist trips without extreme changes in climate and time zones have a good effect.
Migraine prevention
Prevention involves taking the medicine daily for a certain period of time. Which one is prescribed by a neurologist individually. This medicine will act not on the symptoms, but on the cause of the disease, preventing attacks from developing. However, drug prevention is not indicated for everyone. It is prescribed if:
- number of attacks – up to 8 per month or 2 per week;
- Even specific anti-migraine medications - Zomig, Relpax and other triptans - hardly help the patient;
- Triptans and analgesics cannot be taken due to contraindications;
- The patient has hemiplegic migraine, a rare hereditary disease that leads to stroke.
Treatment at the Energy of Health clinic
Neurologists at the Health Energy clinic are ready to help with migraines of any severity. We offer each patient:
- individual selection of drugs for the relief and prevention of attacks;
- training in relaxation and self-help techniques;
- sessions of restorative massage and physical therapy in the absence of contraindications.
Treatment is selected according to the individual characteristics of the body. Before prescribing a specific regimen, a complete examination of the patient is carried out to exclude other causes of headache.
Advantages of the clinic
Medical facilities are equipped in accordance with modern standards of diagnosis and treatment of diseases. We try to make every patient feel comfortable within the walls of the clinic and offer:
- consultations with doctors of various specialties;
- informative methods of instrumental, functional and laboratory diagnostics;
- individual selection of treatment regimen;
- complex effect on the body using not only drugs, but also additional methods: physiotherapy, massage, exercise therapy, manual therapy, etc.
Reception is by appointment, without queues or long waits. The location of the centers allows both motorists and those traveling by public transport to reach us comfortably.
If migraine attacks are making your life miserable, do not endure the pain. Contact the neurologists at Health Energy. Together we will find a way to relieve you of this disease.