General information about the disease
Meningitis is a dangerous disease that can cause serious consequences. The pathology is characterized by inflammation of the lining of the brain, in which a large amount of cerebrospinal fluid (CSF) begins to form, the medulla is damaged, and blood microcirculation in the vascular bed deteriorates.
The consequences of such inflammation are neurological changes that negatively affect the life and health of the patient, as well as cerebral edema - an emergency condition requiring immediate medical attention.
Factors causing the development of meningitis are divided into aseptic and purulent subtypes. The aseptic type is characterized by the viral nature of infection: enterovirus, herpes and choriomeningitis viruses. The purulent type of infection is caused by the intervention of bacteria: meningococcal, pneumococcal, staphylococcal - or external surgical influence.
For meningitis, depending on the nature of the infection, special treatment is required. To diagnose the causative agent of the disease and determine the method of therapy, a specific study of the spinal cerebrospinal fluid is performed - a puncture for meningitis.
Excess cerebrospinal fluid (cerebrospinal fluid) is produced in the cerebral ventricles. At the bottom of these areas of the brain there are plexuses of blood vessels responsible for the production of fluid. The cerebrospinal fluid passes through the ventricles and penetrates the subarachnoid space of the brain and spinal cord. Liquor is necessary to maintain an optimal level of intracranial pressure, provide shock absorption during shock and injury, and nourish brain tissue and cells. Liquor washes the lining of the brain and therefore represents a certain container for the accumulation of viruses and bacterial microorganisms during illness.
Insertion of a special needle into the subarachnoid space - lumbar puncture - is a modern and accurate method for diagnosing the causative agent of infectious meningitis using spinal cord fluid analysis.
2.Why are bone marrow biopsies and spinal taps performed?
A bone marrow biopsy and puncture is performed to:
- Find the cause of changes in red blood cells, white blood cells, or platelets in patients with thrombocytopenia, anemia, or abnormal white blood cell counts.
- Identify blood disorders such as leukemia, anemia, or factors affecting the bone marrow (multiple myeloma or polycythemia).
- Make sure that Hodgkin lymphoma or another type of lymphoma has not spread to the bone marrow.
- Look for infections or tumors that may have spread to the bone marrow.
- Find the best treatment methods for bone marrow diseases.
- Collect bone marrow samples for medical procedures such as stem cell transplants or chromosomal analysis.
Features of the procedure
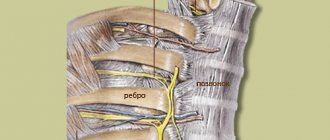
A puncture for meningitis is carried out as follows. The manipulation is carried out on the operating table, where the patient is positioned lying on his side with his legs pulled up to his chest. The head is tilted forward. The specific position of the body ensures the expansion of the intervertebral spaces, which facilitates the insertion of the needle and reduces the patient’s pain. In some cases, the procedure is performed while sitting (if the patient is overweight).
The target area from which material for analysis is taken is at the level of the 3rd – 4th lumbar vertebrae. To quickly and accurately determine the 4th vertebra, the following method is used: when connecting the iliac crests, a conditional line is drawn, which is located at the level of the desired vertebra.
The procedure is carried out under sterile conditions. The puncture site is treated with a disinfectant. After which the patient is injected with a drug for local anesthesia. The anesthetic is administered three times: intradermally, subcutaneously and additionally during manipulation.
The needle with the mandrel is inserted parallel to the spinous processes and slowly moved forward until it enters the cavity (feeling of failure). This means that the instrument has passed through the dura and ligaments and entered the subarachnoid space. An initial collection of cerebrospinal fluid is then performed to verify correct needle placement. After this, the material for research is collected into a clean test tube.
When assessing the result of the manipulation, the nature of the flow of cerebrospinal fluid into the test tube, the color and type of brain fluid are taken into account.
Normally, cerebrospinal fluid should flow out in the form of rare drops. With frequent and rapid flow, a significant increase in intracranial pressure is likely. The red tint of the secreted fluid indicates a possible hemorrhage in the subarachnoid space or damage to the vessel during puncture.
The duration of the procedure is about 7 – 10 minutes. In this case, the patient may experience quite unpleasant sensations. At the end of the manipulation, the needle is removed, the injection site is treated with an antiseptic and a bandage is applied. The patient must remain motionless for 2 to 3 hours after the puncture to eliminate the risk of cerebrospinal fluid leaking out of the hole.
A cerebrospinal fluid puncture can be taken not only to establish an accurate diagnosis and the causes of meningitis infection. The procedure is prescribed to eliminate intracranial hypertension through the direct administration of antibiotics. Also, during the manipulation, the pressure of the cerebrospinal fluid is measured and the patency of the cerebrospinal fluid tract is examined.
Analysis results
Each type of meningitis is characterized by a specific type of pathogen, which will describe changes in the spinal cerebrospinal fluid.
Viral meningitis is characterized by certain changes in the cerebrospinal fluid:
- the predominance of the concentration of lymphocytes over the content of leukocytes in percentage terms;
- absence of bacterial microorganisms in the sown material;
- clear color of cerebrospinal fluid.
Bacterial meningitis is accompanied by the following changes in the cerebrospinal fluid:
- increase in the number of neutrophils (above 1000 per 1 mm3);
- the predominance of the concentration of leukocytes over the number of lymphocytes in percentage terms;
- opaque color of cerebrospinal fluid;
- low glucose levels;
- the presence of a bacterial focus of infection;
- positive reaction on Gram stain.
In typical types of the disease, the level of neutrophils reaches 75–95%. The leukocyte norm for newborns is up to 30/mm3. At an older age, the concentration should not exceed 5 leukocytes per 1 mm3. In healthy children who do not suffer from viral or bacterial meningitis, monocytes and lymphocytes predominate in the cerebrospinal fluid.
Tuberculous meningitis is characterized by specific symptoms:
- the lymphocyte content reaches 100/mm3;
- low glucose;
- bacterial foci determined by staining of the cerebrospinal fluid;
- cloudy liquid.
Indications and contraindications for the procedure
Lumbar puncture is prescribed in the following cases:
- signs of neuroinfection (encephalitis, meningitis and others);
- risk of hemorrhage in the subarachnoid space;
- clarification of the diagnosis of liquorrhea;
- diagnosis of oncological processes and metastases in the lining of the brain;
- diagnosis of cerebrospinal fluid fistulas using cerebrospinal fluid puncture and injection of contrast agent;
- diagnosis and prevention of neuroleukemia in patients with hematological oncology.
If there are such indications, taking a puncture of liquor fluid is the only and key diagnostic method. In some cases, the procedure is used as an additional examination method:
- diseases accompanied by destruction of the membrane of neurons of the central nervous system and PNS (demyelinating processes);
- inflammatory polyneuropathy;
- attacks of fever in the absence of other symptoms.
Indications and contraindications for spinal puncture
The procedure can be performed according to absolute and relative indications. Absolute indications for lumbar puncture relate to:
- suspected neuroinfections;
- tumors of the meninges;
- confirmation/exclusion of central nervous system bleeding;
- determination of primary CNS tumors and metastases;
- impossibility of performing CT, MRI in case of disturbances of consciousness without symptoms of brain herniation;
- diagnosis of hydrocephalus with normal intracranial pressure;
- the need to administer a contrast agent to identify cerebrospinal fluid fistulas and leakage of cerebrospinal fluid from natural orifices;
- administration of antibiotics for severe bacterial meningitis.
Among the relative indications are:
- paraneoplastic syndromes;
- polyneuropathy;
- systemic lupus erythematosus;
- demyelinating diseases;
- septic vascular embolism;
- elevated temperature and absence of signs of inflammation in other organs.
Lumbar puncture is not performed if there is a suspicion of displacement of the brain, hydrocephalus caused by impaired outflow of cerebrospinal fluid, cerebral edema, or space-occupying formations in the skull. This procedure is also contraindicated for bleeding disorders and infections in the lumbar region (folliculitis, furunculosis, bedsores).
Main services of Dr. Zavalishin’s clinic:
- consultation with a neurosurgeon
- treatment of spinal hernia
- brain surgery
- spine surgery
Risks and consequences of a spinal tap
Complications after puncture occur primarily when the rules of manipulation are not followed and doctors make mistakes. In other cases, the following consequences may occur:
- wedging of individual structural elements of the brain;
- dislocation of midbrain structures;
- damage to nerve endings causing pain in the patient;
- headaches, nausea, vomiting;
- hematomas at the site of needle insertion when small capillaries are damaged.
When taking cerebrospinal fluid material from pregnant women, the risk of spontaneous abortion increases, especially in the first third. Patients suffering from cardiovascular diseases also represent a risk group during manipulation. In particularly serious cases, the launch of vasovagal processes can provoke cardiac and respiratory arrest.
Contrary to popular belief that puncture can lead to paralysis, this complication is unlikely. The needle is inserted into the part of the spine that is most poorly innervated and the risk of damage to nerve endings is very low. The incidence of complications after puncture in patients does not exceed 1%.
After two weeks of intensive treatment, the patient’s health condition and the effectiveness of the chosen therapy method are assessed. To do this, repeat manipulation is performed with the collection of spinal fluid material for research. Based on the results of the puncture, changes in the cellular composition are analyzed and the presence or absence of a bacterial culture in the contents is determined. Positive dynamics indicate the patient’s clinical recovery.
Meningitis is a serious disease that requires accurate identification of the causative agent of the infection and the appointment of competent treatment. Cerebrospinal fluid puncture is the only and reliable method for diagnosing the disease.
Is a dangerous spinal tap necessary to diagnose meningitis?
Answered by Komarovsky E. O.
We are talking about a disease that poses a real threat to the patient’s life.
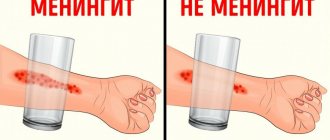
We suspect meningitis, but we are not sure, because, for example, with dysentery - a typical intestinal infection - there are often very similar symptoms, and until you see the contents of the pot, you cannot make a diagnosis. But you understand that dysentery and meningitis are treated slightly differently? Meningitis is serious, it requires huge doses of certain antibiotics, these are specific treatment regimens and medications. We have suspicions and we need an answer. The only way to do this quickly and reliably is to perform a puncture of the spinal canal. Often, even by the color of the liquid in a test tube, you can see whether there is meningitis or not. If the liquid is clear, you can wait; if it is cloudy, it means there are a lot of leukocytes, protein, pus, inflammation, and you need to act immediately. In just a few minutes, this liquid can be examined under a microscope and you can determine what kind of cells it is, what pathogen it is, and begin treatment.
Thus, puncture of the spinal canal is the only diagnostic method for suspected meningitis. Only after examining the cerebrospinal fluid are final conclusions made about the type of meningitis and treatment begins.
Regarding the dangers of spinal puncture - as a person who has performed about five thousand such manipulations in his life - I can say that these are typical old wives' tales. The fact is that antibiotics to treat meningitis appeared in the 1950s, and spinal taps in an attempt to help patients were used much earlier. Relatively speaking, here is a seriously ill person who is being helped in every possible way, including with the help of a puncture, trying to reduce the pressure, but he still dies. Why did he die? Well, of course, because of the puncture, although in fact it was the disease that killed him.
The puncture is done very low - no nerves emerge from that part of the spine, and the person cannot be paralyzed by this. These are all, I repeat, fairy tales.
If the doctor is faced with a choice: to perform a spinal tap or leave the child without a diagnosis, then the doctor will do it.
Please do not resist this procedure - it is virtually painless and I have never seen any side effects from it. It is better to do an unnecessary puncture than to leave the child without treatment for a disease that really threatens his life and health. All answers