Hospitalization and treatment under the compulsory medical insurance quota. More details after viewing the pictures.
Brain tumors can be benign or malignant; the latter are aggressive in nature and pose a significant threat to life. Neoplasms form inside the skull due to abnormal disturbances in the cellular genetic apparatus, which leads to uncontrolled growth of tissue structures. Atypical cells are formed from normal ones as a result of mutations, exposure to physical, chemical or other factors. These can be various cells of brain tissue, for example, neurons, glial cells and others. Often, metastasizing cells formed from cancer of other organs enter the brain, which leads to the formation of secondary malignant tumors. The main treatment involves surgical removal of pathological foci, additionally radiation and chemotherapy are prescribed, as well as drugs to relieve negative clinical manifestations.
Causes of tumors
At the moment, medical science does not fully understand the reliable causes of the formation of cancer. Doctors name factors that increase the risk of tumor formation. An important role is played by the age and gender of a person. Some types of cancer, such as meningiomas, are more often diagnosed in women over 45-50 years of age. This is due to the characteristics of the female endocrine system and hormonal levels. For example, during pregnancy, some neoplasms progress more intensively. Brain tumors in men, as a rule, have a more severe course and complex prognosis, because in this case the tumors are highly malignant.
Other provoking factors include:
- adverse environmental impacts: radiation, hazardous industries, living in contaminated areas, etc.;
- constant contact with toxic elements;
- infection with viruses that can contribute to the development of cancer;
- genetic characteristics (the presence of certain genes in the human genome that increase the risk of developing a brain tumor);
- head injuries of various nature and origin;
- treatment with drugs, for example, hormones, chemotherapy;
- bad habits;
- consumption of low-quality food saturated with carcinogenic elements.
These factors can influence the formation of diseases both separately (for example, heredity) and in combination.
Where is the reason
The occurrence of these neoplasms, like any other oncological processes of other localization, is associated with a violation of antitumor protection, which can be caused by chronic intoxication with toxic substances, radiation, significant environmental pollution, genetic predisposition and other factors.
Children may experience congenital (embryonic) tumors, the cause of which lies in a violation of embryonic development. Traumatic brain injury can act as a provoking factor and activate tumor growth. There is no single reason. The oncological process is considered as a multifactorial disease.
Types of tumors
Neoplasms that form in the brain can be:
- Benign – tumor tissue does not contain cancer cells. Neoplasia of this type is characterized by clear edges and slow growth. They are much easier to treat surgically, but can become malignant, that is, turn into cancer;
- Malignant tumors contain abnormal cells that can divide uncontrollably and metastasize to other organs. In this case, the disease is difficult to control; in the later stages, surgery is impossible. Treatment in this case is difficult, has a high cost and, as a rule, poor prognosis.
Brain glioma
Glioma
This type of tumor is diagnosed more often, accounting for approximately 60% of all types of cancer that form in the brain. The tumor is formed from glial cells. In most cases, this is a primary neoplasm, most often formed in the area of the chiasmata or ventricles, but it can also affect the brain stem; pathogenesis rarely extends to the bones of the skull, however, in rare cases this is possible. The size of gliomas is usually up to 14 cm. Metastases are rare, growth is usually slow, but due to penetration into adjacent tissues, the boundaries of the lesion are difficult to distinguish.
Three varieties are known
- astrocytoma – diagnosed more often than others (it accounts for about 50% of gliomas);
- oligodendroglioma – up to 10% of cases;
- ependymoma – less than 7%.
According to the World Health Organization classification, there are 4 stages of glioma:
- The first stage is benign. It is characterized by slow growth. Example: giant cell astrocytoma.
- Second stage. Features: borderline malignancy with slow tissue growth, easily progresses to stages 3 and 4. In this case, only one symptom of cancer is identified - cellular atypia.
- Third and fourth stage. In this case, the tumor has all the signs of cancer, for example, necrotic changes in glioblastoma multiforme.
Brain astrocytoma
Removal of a large GRADE II WHO astrocytoma of the right temporal lobe (before surgery)
This malignant neoplasm of varying degrees of aggressiveness is diagnosed quite often. The beginning is given by degenerated glial cells - astrocytes (hence the name - astrocytoma). There are:
- Common astrocytomas: protoplasmic, fibrillary and hemisrocytic.
- Special astrocytomas: cerebellar, piloid, microcystic and subependymal.
Astrocytomas are distinguished by the stage of malignancy:
- The first stage (benign tumor) includes piloid or pilocytic astrocytoma of the brain.
- Second stage of malignancy: fibrillary tumor is also an ordinary neoplasia, second degree of malignancy.
- The third stage is already cancer. It includes anaplastic astrocytoma of the brain.
- The most life-threatening are glioblastomas (giant cell glioblastoma and gliosarcoma), which are classified as stage 4 and are characterized by rapid growth and the ability to metastasize.
In addition to the ones mentioned, there are other types of astrocytomas, for example, ependymoma (develops from ventricular cells), oligodendroglioma (forebrain) - grow quite slowly without the formation of metastases, and glioma of the brain stem.
Meningioma of the brain
Removal of a large middle cranial fossa meningioma before surgery
Pathogenesis begins with pathogenic cells in the superficial membrane that surround the brain tissue. The neoplasm is oval in shape, grows slowly, and is therefore considered benign. Meningiomas are diagnosed in 15% of cases (of all brain tumors). The risk of degeneration into cancer is about 3-4%. The clinical signs that appear are caused by increased intracranial pressure and tissue compression. With malignancy (degeneration of somatic cells into carcinogenic ones), meningiomas become aggressive. Usually more than one lesion forms and may spread to the spinal cord. After surgical treatment, there is a high probability of relapses. As a rule, pathology is diagnosed by chance, because symptoms appear only when the lesion reaches a large size. There are no early signs of the disease.
Note. Meningiomas often form in females.
Other types of brain tumors
There are quite a lot of types of neoplasms. Here are some of those that are diagnosed relatively often (besides those mentioned above):
- medulloblastoma is a brain cancer that originates from the structures of the cerebellum;
- germinoma - formed from germ cells, most often it is detected in the first half of a person’s life;
- Craniopharyngeoma - develops in the pituitary gland at the base of the brain;
- Shawnoma – formed from degenerated Schwann cells;
- tumors in the pineal gland area.
Principles of treatment
Treatment of intracranial tumors is a complex task that requires a collegial approach with the participation of neurosurgeons, oncologists, and radiologists. Surgical treatment and biopsy are carried out in specialized neurosurgical centers.
The main methods of treating both primary and metastatic brain tumors today remain surgery, radiological methods and chemotherapy. At the same time, there are a large number of treatment tactics, depending on what kind of tumor we are talking about, as well as its location, degree of malignancy, growth rate, general condition of the patient, degree of influence on brain structures, characteristics of the primary focus (for metastatic tumors) and many other factors.
Chemotherapy is a method based on the use of drugs that inhibit the growth and reproduction of tumor cells. The method can be used before and/or after surgery or radiological treatment, or used entirely independently if other procedures cannot be performed.
Radiological treatment involves exposing the tumor to ionizing radiation. In this case, it is possible to irradiate all brain tissue, for example, in case of multiple metastases, or to use stereotactic radiosurgery methods - to expose the lesion to a large dose of radiation, practically without affecting the surrounding tissue.
Surgery is often the most radical, but not always feasible, treatment method. Surgery may be required not only to remove the tumor, but also if severe complications occur - cerebral edema, compression of vital structures. With multiple metastatic tumors, it is possible to remove one lesion if it determines the severity of the patient’s condition and there are prospects for its conservative treatment.
Clinical manifestations
Symptoms are usually divided into general and focal. In the latter case, the symptoms depend on where the tumor forms.
General symptoms
The clinical picture is caused by an increase in pressure inside the skull and the toxic effect of metabolites of pathogenic cells on healthy tissue. Common signs include:
- headache not relieved by conventional analgesics;
- various visual impairments, for example, fog, doubling, glare, decreased visual acuity and others;
- loss of appetite, poor health, nausea and vomiting that are not caused by food poisoning;
- changes in the usual emotional state: mood swings, depression or aggressiveness, and others;
- symptoms of an epileptic nature;
- weakening of the brain: it is difficult for a person to concentrate, mental activity is disrupted, there is a loss of concentration, memory problems, etc.
Important. Early signs of cancer are often misunderstood by sick people. They seek help when clinical signs significantly impair quality of life. In this case, the brain tumor is diagnosed late, which significantly complicates treatment and worsens the prognosis.
Focal symptoms
Signs of this type arise due to changes in the functioning of cerebral structures, so the clinic depends on the location of the neoplasm:
- when the hemispheres are damaged, tactile sensitivity decreases, muscles in the opposite part of the body weaken (in the presence of pathogenesis in the right hemisphere, problems arise on the left side);
- disease in the temporal lobe leads to a deterioration in the ability to speak, memory suffers, and the perception of smells changes;
- pathological changes in the cerebellum lead to disturbances in gait and coordination of movements;
- damage to the frontal lobe causes mental and cognitive changes;
- neoplasia in the parietal lobe changes tactile sensations and fine motor skills;
- damage to the occipital zone negatively affects vision, and hallucinations are possible.
Important. The presence of these signs (of any type and intensity) is a good reason to seek medical advice. Early detection of pathologies improves the prognosis of treatment.
Indications for surgical removal of a tumor
1. The indication for mole removal is the ABCDE test score:
- A – asymmetry of the neoplasm, uneven growth.
- B – fuzzy, blurry, jagged edges.
- C – heterogeneous color with blue, black, red splashes.
- D – large size, approximately a diameter of more than 5-6 mm.
- E – change in any of the characteristics (growth, pigmentation, surface relief).
If the mole begins to change in appearance, itching, swelling appears, and pain is felt on palpation, then you should immediately see a doctor.
2. Papilloma has a viral etiology and is the result of HPV infection. If the immune system cannot cope with the virus, then as a result of penetration and activation of a chronic infection, epithelium grows on the mucous membrane or skin. Not all papillomotosis is potentially dangerous, but there are strains of HPV that cause cell malignancy.
Oncogenic risk is carried by neoplasms that:
- They grow, increase in size, “spread”, their number increases.
- They darken, lighten, change color.
- They become denser and have a heterogeneous structure.
- Cause discomfort and pain.
It is recommended to remove any tumors that are easily injured due to their location. These can be papillomas (or moles) located on the neck, arms (especially on the elbow), and in women under the elastic bands of the bra. Large tumors on the lower back are also considered traumatic. When the skin is damaged, any infection easily penetrates through an open wound, creating more favorable conditions for inflammatory processes and suppuration. Therefore, it is recommended to remove potentially traumatic papillomas and nevi even if they do not bother you and do not carry an oncogenic risk.
3. Benign tumors have different etiopathogenesis. Some hormonally dependent forms (fibroids, etc.) require observation and are treated with medications (hormonal therapy), others are considered relatively harmless (fibroids), and others are considered precancer (for example, polyposis of the stomach and colon). Therefore, the treatment method is always chosen individually after a thorough examination and clarification of the diagnosis.
If benign tumors are detected, the nature of which cannot be determined, it is recommended to remove them surgically with histological examination of the excised tissue. Such neoplasms include tumors of the lymph nodes, internal organs and skin, which are externally similar to cystic formations or, for example, large inflamed lymph nodes.
Diagnostics
The initial examination involves an oral interview and a physical examination. The doctor assesses the patient’s general condition, determines the nature of clinical manifestations, their duration and intensity, evaluates coordination, reflexes, psycho-emotional state, and so on. Next, the patient will have to undergo a thorough diagnosis, which may include the following types of studies:
- general blood and urine tests;
- blood chemistry;
- Ultrasound (echoencephalography);
- angiography - X-ray contrast study of the condition of the blood vessels of the head;
- examination of eye function and level of vision;
- computed tomography or magnetic resonance imaging – obtaining high-precision layer-by-layer images, which allows you to identify all the nuances of the disease and determine the method of tumor removal;
- magnetic resonance spectroscopy – study of the functioning of pathogenic tissues at the biochemical level;
- positron emission tomography (PET) of the head shows the characteristics of metabolic processes in the painful focus, which makes it possible to talk about the rate of development of the disease;
- biopsy - tissue collection for histological examination; in this case, the material is obtained after tumor removal.
Also of great diagnostic importance is the study of cerebral fluid, in which pathological cells are located. The stereotactic biopsy method is the most informative in terms of determining the type of carcinogenesis and its characteristics.
Removal of lymph nodes
If there is a suspicion of damage to the lymph nodes closest to the organ (regional) by tumor tissue, they are also removed and sent for a biopsy. This operation is called lymph node dissection.
If the doctor is unsure whether the cancer cells have spread to the lymph nodes, a sentinel biopsy or sentinel lymph node biopsy is performed when the tumor is removed. A special dye is injected into the location of the tumor, which penetrates the lymphatic system, and they look at which lymph node it goes to first. This lymph node is called a sentinel lymph node - it was where cancer cells would first get if they began to spread through the lymphogenous route.
The sentinel lymph node is removed and biopsied. If cancer cells are found in it, lymph node dissection is performed.
Brain tumor removal
Therapy for neoplasms is complex, always complex and quite expensive. For example, in Russia, surgical treatment of a brain tumor is estimated at approximately 350 thousand Russian rubles. You can find out the final cost of treatment in one of the best oncology centers in the Russian Federation after consulting a neurosurgeon. Prices abroad are much higher. In Germany, for such therapy you will need to pay about 28,000-30,000 US dollars, in Israel it is several thousand cheaper, so it is important to take this fact into account when choosing a clinic. You need to pay attention to the nuances. For example, the equipment in foreign clinics is often better, although the treatment methods and results are not fundamentally different, but in the event of an unfavorable outcome, Western specialists will not have to deal with paying local insurance, so they easily take foreign patients who pay for everything themselves.
Note. The main treatment is a radical surgical operation; other methods used in combination act as auxiliary ones (chemotherapy, radiotherapy and other methods).
Brain cancer can only be removed through surgery. It is performed for nodular tumors and is impossible for diffuse neoplasms due to deep infiltration into nearby structures. In such circumstances, brain tumor surgery is performed to remove some of the abnormal tissue, relieve pressure inside the skull, and prevent dropsy. The size of the tumor and the stage of the cancer play a decisive role in deciding whether to remove the tumor.
Radiotherapy involves repeated exposure of cancer cells to radiation, which leads to blockade of division and death of the latter. With significant doses of radiation, pathogenic cells stop developing and most of them die.
At the same time, treatment involves the use of chemotherapy through oral and intravenous administration of cytostatics (toxic substances for pathogenic cells). These therapies have many negative effects. Recently, medicine has been producing more and more unique chemical drugs that selectively target tumor cells, which can significantly reduce the negative impact of poisons on the body.
At the same time, medications are prescribed to eliminate unfavorable signs that can be caused by both the tumor and side effects from the proposed treatment.
Surgery
Surgeries to remove tumors in the brain are the only effective treatment. This type of treatment is very complex. The possibility and effectiveness of the operation depends on many factors, among which important are the stage of cancer, the nature of the spread of pathogenic tissues, the presence of metastases and secondary foci, as well as the localization of pathogenic formations in brain tissue.
Any neurosurgical operation is quite complicated, because the doctor must remove a malignant tumor located between healthy brain tissue. Therefore, treatment of this kind is traumatic, and in some cases impossible. For example, cancer removal is not carried out if the tumor is large, when it affects vital parts of the brain, or if the disease is at a terminal stage. In addition, the person’s health status, the presence of chronic diseases, their stages, the patient’s age and other features are taken into account.
In each specific case, the choice of technique and method of tumor removal is selected individually. At the moment, doctors have a lot of specialized surgical equipment in their arsenal, for example, tomographs, laser and ultrasound equipment. This significantly increases the efficiency of operations to remove tumors.
Most often, surgical removal of brain cancer involves trepanation and resection of the skull. The methodology is as follows:
- At the beginning of the operation, the surgeon dissects the skin layers above the cranial vault (a scalp incision is made).
- After turning away the cut skin, the doctor moves the muscle layers aside.
- At the next stage of the operation, the required part of the bone tissue of the skull is removed so that the brain tumor becomes accessible for manipulation.
- Then the pathological focus is excised and the extracted bone tissue is installed in its original place (this is called trepanation). If part of the skull is not returned to its original place, then such an operation is called resection.
- At the final stage of the operation, the soft tissues covering the skull are restored and sutures or staples are applied.
After resection, the hole in the skull is closed with a special material or mesh. Removing pathogenic tissue reduces intracranial pressure, freeing up space for swollen tissue afterwards. In addition, craniotomy is necessary if the tumor process has spread to bone tissue. After removal, the extracted biological material is sent for histological analysis.
Cost of treatment
| Name of service | price, rub. | Unit measurements |
| Consultation with an oncologist and radiotherapist | 1 500 | PC. |
| Consultation with a pediatric oncologist | 0 | PC. |
| Repeated consultation with specialists | 500 | PC. |
| Primary topometry on a specialized computed tomograph | 15 000 | procedure |
| Repeated topometry on a specialized computed tomograph | 7 000 | procedure |
| Primary dosimetric planning of radiation therapy (tomotherapy) | 20 000 | PC. |
| Repeated dosimetric planning of radiation therapy (tomotherapy) | 7 000 | PC. |
| Radiation therapy (tomotherapy), including IMGRT (*) | 315 000 | well |
| Radiation therapy (tomotherapy) stereotactic radiofrequency surgery (*) | 315 000 | well |
| Accompanying drug therapy: intravenous administration in the treatment room (excluding the cost of medications) | 1 000 | procedure |
| Accompanying drug therapy: intramuscular administration in the treatment room (excluding the cost of medications) | 200 | procedure |
| Topometric marking | 750 | procedure |
The type of radiation therapy and the number of sessions of the course are determined by the medical commission individually for each patient based on the location, nosology of the tumor and taking into account the medical history.
Free online consultation
Sign up
Life forecast
Without surgery, treatment of malignant tumors is ineffective, and the prognosis is extremely negative. After removal of a tumor, life expectancy depends on the stage, level of malignancy, type of carcinogenesis and the degree of its germination into other structures. As a rule, after partial removal of the tumor, brain cancer comes back again, so surgery in this case prolongs the patient’s life for a very short time. The patient will live no more than a year if the relapse is aggressive, and only 25% of patients will live more than two years. After removal of the pathological focus at the first stage of malignancy, life expectancy in 80% of patients is estimated at more than 5 years (in the case of complete removal of carcinogenic tissue). The most dangerous are the late stages of the disease. The prognosis for life at the quadruple stage is not very encouraging - a person will not live longer than a year.
A revolution in understanding the nature of metastasis
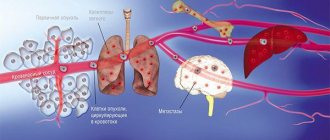
The efforts of many oncologists over the past decades have been aimed at establishing the details of the occurrence and development of cancer - the mechanisms of tumor initiation and regulation of its active growth, the formation of a favorable microenvironment of stromal cells [2]. This knowledge has undoubtedly led to the development of new approaches to the treatment of cancer. Over time, it became clear that the main threat of cancer lies in its ability to spread throughout the body. Thus, some cancer cells of the primary tumor (that is, those that developed initially) are separated from it due to epithelial-mesenchymal transition or other mechanisms [3] and, entering the bloodstream or lymph flow, travel through small capillaries to the main highways of the vascular system. They leave it due to retention in the narrow capillaries of organs, adhesion to their endothelial wall and exit from the lumen of the vessel into the stroma of the organ (Fig. 1). Only a small percentage of cancer cells that leave the primary tumor succeed in this process and survive in their new environment. These cells form future foci of tumor growth in new organs - metastases .
Figure 1. Metastasis and dispersal pathways of cancer cells.
Wikipedia, pictures adapted
The process of cancer cells dispersing throughout the body, called metastasis (from the ancient Greek “to change, transfer”: meta - “through” + histanai - “to establish”), was first described back in 1889 by Stephen Paget [4], but the mechanism of its development remained a mystery for the scientific community for a long time (Fig. 2).
Figure 2. The founders of the doctrine of metastasis: English surgeon Stephen Paget (left) and American pathologist James Ewing (right).
"Wikipedia"
Paget drew an analogy between this spread of cancer cells and the germination of seeds. They also survive and divide on fertile “soil” - in a suitable microenvironment. At that time, it was impossible to find experimental confirmation of this, and for a long time a completely different theory prevailed - that of James Ewing (Fig. 2). He argued that the main role in the distribution of metastases throughout the body is played by the dynamics of blood flow and the structure of the vascular system.
Finally, in the 1970s, through several experiments injecting radioactively labeled cancer cells into mice, Isaac Fiedler was able to prove that the outcome of metastasis also depended on the nature of the cancer cells. In this case, melanoma cells developed metastases only in the lungs, but not in the liver, in the vessels of which they also lingered, but later did not survive [5].
Later, even more facts were established confirming that cancer cells of different nature metastasize predominantly to certain organs and sometimes even in a given sequence. For example, breast cancer cells - first to the bones, liver, lymph nodes, lungs, and then to the brain; cancer cells of the gastrointestinal tract and ovaries - to the liver and lungs; prostate cancer - mainly in the bone (Fig. 1). The phenomenon of specific distribution of metastases throughout the body is called organotropy of metastasis. Most often, metastases occur in the lungs, liver and bones.
Despite active research, there are still many unanswered questions in oncology. Are metastatic cancer cells different from other cells in the primary tumor? What is the basis of organotropy? How do metastases survive after removal of the primary tumor and chemotherapy?
Initial signs
Brain cancer does not always present with a clear clinical picture. At the initial stages, the disease does not manifest itself in any way, and the first symptoms appear as the tumor grows and puts pressure on other centers. The first signs of the disease often resemble the symptoms of migraine or hypertension, so a person, unaware of the pathology, treats himself independently, refuses comprehensive diagnostics, which leads to an increase in formation and pronounced symptoms.
The first signs of the disease can appear acutely or bother a person for periods, depending on the location and size of the formation.
- Frontal lobe - the tumor is located in the front part of the brain, and may not bother a person for a long time. As it grows, changes occur in the mental state, and signs of epilepsy appear. If the formation is located in the posterior part of the frontal lobe, then problems with speech are noted. Common and early symptoms include chronic fatigue, pain in the legs and muscles.
- Parietal lobe - in the initial stages there is a decrease in the sensitivity of one limb, logical thinking decreases, and speech is impaired.
- Temporal lobe - damage to this area leads to mental disorders. The patient has hallucinations, vision impairment, memory loss, and signs of epilepsy may be present.
- Occipital lobe - the presence of a tumor in this area is negatively reflected in the visual system, intracranial pressure increases, and general cerebral symptoms are also present: headache in the back of the head, nausea.
- Ventricles of the brain - characterized by general cerebral symptoms, as well as disturbances in the hormonal and cardiovascular systems.
- Posterior cranial fossa - a tumor in this area causes difficulty concentrating, there is muscle weakness, general fatigue, and clouding of consciousness.
- Brain stem - accompanied by loss of coordination and decreased sensitivity of the limbs; there may be a change in the shape of the face. The disease develops slowly, and the first symptoms may appear a year after formation.
It is important to understand that the first signs of brain cancer appear when the tumor grows large and puts pressure on other tissues.
Nutrition after surgery in oncology
During the recovery period after cancer treatment, it is important for the patient to eat well. But the digestive system does not immediately recover after surgery, especially if it was performed for cancer of the digestive system.
Some time after surgery, the patient is allowed to drink water, then a liquid diet is prescribed. Gradually you can return to your usual food. The diet after surgery for cancer should be gentle and at the same time provide the body with all the necessary substances.
During the recovery period, the doctor assesses the patient's nutritional status. Some patients cannot feed themselves; in such cases, nutritional solutions are administered intravenously. After operations on the esophagus and stomach, a gastrostomy or jejunostomy may be removed - an opening connecting the skin to the stomach or colon. The patient may receive nutrition after cancer surgery through this opening using a catheter, either temporarily or permanently.
Even if the tumor is completely removed, in some cases there is a possibility that some cancer cells remain in the body. They may cause a relapse in the future. In order to prevent it, adjuvant treatment is prescribed. It may include courses of chemotherapy, radiation therapy, and targeted drug therapy.
Complications after surgery
In general, after surgical interventions in oncology, the same complications are typical as after other operations: pain, bleeding, poor wound healing, infections, damage to nerve trunks with subsequent impairment of their functions (movements, sensitivity). If a large part of an organ has been removed, its function is impaired.
In the postoperative period, adequate pain relief is of great importance. Pain after surgery for cancer in oncology is combated with the help of narcotic and non-narcotic analgesics. An elevated temperature after cancer surgery may indicate an infection. In this case, swelling and redness appear in the area of the surgical wound, and pus may be released from it. In such cases, they are treated with antibiotics; if an abscess has formed, it is opened and drained.
After removal of lymph nodes, the outflow of lymph may be disrupted with the formation of edema - lymphedema. The more lymph nodes removed during surgery, the higher the risk of this complication.
After surgery, cancer patients often have persistent health problems that limit their ability to work. In such cases, the doctor refers the patient to MSE, and after the operation, the oncology department establishes a disability group.