General information
Encephalopathy occurs due to metabolic disorders in brain cells. Regardless of the cause, the pathology follows a single scenario. First, there is a decrease in the activity of neurons, then their gradual death. Foci of dystrophy are located throughout the brain, which causes a variety of symptoms.
The damage is irreversible, but with timely consultation with a specialist and quality treatment, the patient’s condition can improve. The remaining intact neurons partially take over the function of the dead cells, and brain function is significantly improved. If the disease was caught at an early stage, the patient retains complete clarity of mind.
Make an appointment
Stages of encephalopathy
The disease has three degrees of severity:
- The first one . There are no external signs, but instrumental diagnostics demonstrate diffuse changes in the brain tissue.
- Second . Brain activity is impaired, but symptoms occur only occasionally.
- Third . Negative symptoms are pronounced. There is a high risk of disability for the patient.
A disease detected at the first stage is more treatable.
Causes
Damage to nerve cells can occur due to exposure to various pathological factors.
- previous trauma;
- acute or chronic intoxication with salts of heavy metals, narcotic substances, alcohol;
- blood supply disorders (atherosclerosis, arterial hypertension, amyloidosis, etc.);
- infectious diseases (diphtheria, botulism, tetanus and others);
- disorders of the liver or kidneys, accompanied by the accumulation of toxins in the blood;
- disorders of glucose metabolism;
- lack of vitamins (especially group B);
- water retention, lack of sodium in the blood and resulting swelling;
- immunodeficiency states;
- exposure to ionizing radiation;
- hypoxia: insufficient oxygen supply to brain cells.
Description of the disease
Encephalopathy is intoxication or chronic cerebral ischemia. It is characterized by multiple neuropsychological and neurological disorders. The disease develops due to two abnormal mechanisms occurring in the body:
- Deficiency of oxygen supplied to brain tissue cells due to vascular damage due to intracranial/arterial hypertension, thrombosis, diabetes.
- Poisoning of brain neurons by toxic decay products. This problem occurs in alcoholics, drug addicts, substance abusers, and with severe liver and kidney diseases.
According to statistics, people over fifty years of age are more likely to experience the disease. But it also occurs in newborns and pregnant women.
Believing positive reviews about alternative treatment for any type of encephalopathy is a road to nowhere. Only experienced doctors know how to cure this pathology. Therefore, seeking qualified medical help is mandatory.
Kinds
Doctors distinguish between congenital and acquired encephalopathy. The first occurs against the background of an abnormal course of pregnancy or childbirth and, often, develops while the fetus is in the womb. Its signs are detected immediately after birth or appear in the first weeks of life. Neonatologists and pediatricians are involved in the diagnosis and treatment of this condition.
Acquired encephalopathy occurs in adulthood. It is divided into several types depending on the cause of neuronal death:
- post-traumatic: occurs against the background of a traumatic brain injury; often develops within a few years after it and often leads to severe mental disorders;
- toxic: associated with acute or chronic poisoning of the body with alcohol, poisons, narcotic drugs, medicines, salts of heavy metals, etc.; Alcoholic encephalopathy is often distinguished separately within this type;
- metabolic: associated with metabolic disorders in the body; The following subtypes of pathology are distinguished: hepatic: occurs when the liver or biliary tract is damaged;
- uremic: associated with impaired renal function;
- diabetic: is one of the frequent complications of diabetes mellitus, occurs against the background of persistent microcirculation disorders and increased blood viscosity;
- anoxic: develops after clinical death and is associated with oxygen starvation of the brain with the subsequent development of a “metabolic storm”;
- Gaye-Wernicke syndrome: encephalopathy caused by vitamin B1 deficiency;
- pancreatic: is a complication of inflammation of the pancreas;
- hypoglycemic: occurs against the background of a sharp decrease in blood glucose;
- atherosclerotic: develops due to atherosclerosis and thickening of the walls of blood vessels;
Depending on the speed of development of the process, encephalopathy is divided into acute and chronic. The first can develop within a few days or hours, and more often occurs against the background of severe intoxication, trauma, or an infectious process. The chronic process can last for years or decades.
Dyscirculatory encephalopathy: principles of treatment
D
The demographic situation in Russia is such that among the population an increasing proportion is occupied by people of older age groups - “elderly” [1]. The very widespread approach to the problem of aging as a natural process that does not require the intervention of specialists cannot be considered fair and justified. With age, the human body ages, the capabilities of the cardiovascular system decrease, hormonal levels are disrupted, the function of all sensitive analyzers deteriorates, food absorption becomes difficult, age-related changes in the joints and spine make movements difficult. In people over 70 years of age, gross metabolic disorders are observed in 70%, diseases of the musculoskeletal system in 85%, and a decrease in the functional capabilities of the brain (impaired memory, thinking, depression, destruction of the sleep structure) exceeds 90%.
To clinically characterize brain dysfunctions that develop as a result of vascular disorders, the concept of “dyscirculatory encephalopathy” (DE) is widely used in our country. Dyscirculatory encephalopathy is a slowly progressive disorder of the blood supply to the brain, most often developing against the background of atherosclerosis, hypertension, and sometimes against the background of diabetes mellitus, syphilis and other diseases affecting the blood vessels of the brain [2]. It is important to note that DE is the result of diffuse multifocal brain damage
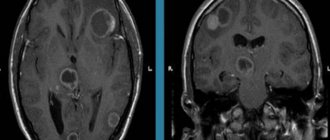
. In most cases, DE can be confirmed by various neuroimaging methods. On CT, DE is characterized by such signs as expansion of the subarachnoid spaces (“atrophy”), periventricular luminescence, expansion of the ventricles of the brain; on MRI, T2-weighted images usually reveal small-point multiple foci localized in the white matter.
For the main etiological reasons, atherosclerotic, hypertensive, mixed and venous DE are distinguished. Based on clinical signs, three stages of DE are distinguished. In stage I
Subjective disorders predominate in the form of headaches and a feeling of heaviness in the head, general weakness, increased fatigue, emotional lability, decreased memory and attention, dizziness, often of a non-systemic nature, instability when walking, and sleep disturbances. Focal neurological symptoms at this stage are manifested by reflexes of oral automatism, weakness of convergence of the eyeballs, and sometimes anisoreflexia.
Stage II
DE differs from the first by more persistent and pronounced symptoms, the appearance of signs of pyramidal and extrapyramidal insufficiency. Characteristic is the identification of a dominant neurological syndrome - discoordination, pyramidal, dysmnestic, etc.
In stage III
Against the background of distinct focal neurological manifestations, intellectual-mnestic disorders become clinically significant, which sometimes reach the level of psychoorganic syndrome. Paroxysmal conditions are more often observed - falls, fainting, epileptic seizures. It is believed that the core of the clinical picture of DE and its distinctive feature are motor and cognitive impairments. Severe movement disorders are usually associated with acute cerebrovascular accident. Another cause of severe motor impairment is progressive extrapyramidal syndrome. Sometimes the patient’s motor activity is hampered by increasing disturbances in coordination of movements.
Along with the progression of focal neurological symptoms as DE develops, higher brain functions are destroyed. Dementia is a common outcome of progressive disorders of the blood supply to the brain.
Successful treatment of DE requires an integrated approach to the problem, taking into account compensation of cardiovascular disorders, restoration of microcirculation and the application of the principles of metabolic therapy [3].
Restoration of central hemodynamics
The basis of therapeutic tactics for DE are methods that allow you to restore normal heart function (including restoration of sinus rhythm) and acceptable blood pressure (BP). It is difficult to count on the success of therapeutic measures if the patient has severe disturbances of central hemodynamics. Assessment of the state of central hemodynamics using echocardiography with calculation of ejection fraction and minute volume of blood, daily monitoring of ECG and blood pressure in most cases provide sufficient information for choosing adequate therapy. Correction of central hemodynamics is a necessary condition for successful treatment of DE. The most promising method of treating arterial hypertension in patients with latent and overt forms of circulatory failure should be considered combinations of small doses of beta-blockers and ACE inhibitors
. Of course, doses and combinations of antihypertensive drugs must be selected individually, in difficult cases with the help of a cardiologist. The goal of this type of treatment for DE is to stabilize blood pressure and restore effective heart function.
Restoration of cerebral hemodynamics
Critical stenosis and occlusion of the main arteries in combination with cardiac arrhythmias and heart failure create favorable conditions for the progression of cerebral ischemia. Reconstructive operations on cerebral vessels have no alternative for symptomatic stenoses, not only for the purpose of preventing stroke, but also for the treatment of chronic cerebrovascular insufficiency. Conservative treatment of symptomatic and asymptomatic stenoses is based on the use of statins
and
disaggregants
.
Improvement of cerebral hemodynamics is traditionally associated with the use of so-called vasodilators
– drugs that dilate intracerebral arteries. The group of drugs used for this purpose is the most representative. Derivatives of Vinca minor (vinpocetine, etc.), xanthine (theophylline, pentoxifylline, etc.), and nicotinic acid preparations have found widespread use. Cinnarizine remains one of the most commonly used drugs for cerebrovascular insufficiency. In recent years, fundamentally new drugs that primarily affect the tone of small arteries (trimetazidine) have been successfully used for this purpose. Calcium channel blockers (mostly nimodipine) and ACE inhibitors have a clear effect on cerebral hemodynamics. The use of modern beta-blockers, which have an effect on the NO-dependent mechanism of vasodilation (nebivolol), is very promising. The arsenal of “vasodilator” drugs for the treatment of cerebrovascular insufficiency is very large. But for their effective use, optimization of different areas of complex therapy is important. Firstly, it is necessary to avoid duplication of the vasodilatory effects of drugs from different pharmaceutical groups. For example, if a patient receives nifedipine, then there is no point in “intensifying” therapy with vinpocetine, because the vasoactive effects of these drugs are comparable. Secondly, before prescribing vasodilators to improve cerebral circulation, it is advisable to make sure that the reserve of cerebrovascular reactivity is not exhausted [4,5]. Are atherosclerotic arteries able to respond to vasodilatory stimuli? If they are not able to, then the only way to improve cerebral blood flow is associated with the restoration of microcirculation.
Correction of microcirculatory disorders
Microcirculatory block is a common and most significant cause of DE. Microcirculation disorders in the elderly are associated both with the state of blood vessels (endothelial dysfunction) and with changes in the blood [5]. Hypercoagulation is typical for patients with arterial hypertension combined with atherosclerosis. Hypercoagulation in the elderly can be due to various reasons, the most significant of which are: decreased fibrinolytic properties of the blood, increased platelet aggregation, endogenous intoxication. In some cases, intravascular coagulation is caused by high homocysteine levels [6]. In recent years, convincing data have been obtained on the participation of blood hyperviscosity in the process of systemic microcirculation disorders in patients with cerebrovascular diseases. An increase in blood viscosity is associated with an increase in plasma viscosity (hyperglycemia, hyperfibrinogenemia, hypercholesterolemia) or an increase in the number and aggregation of blood cells (usually red blood cells). Erythrocytosis is characteristic of chronic lung diseases, heart failure, and is usually found in smokers. Erythrocyte microcirculatory block is caused not only by an increase in the number of red blood cells, but also by a violation of their deformability and a change in the properties of erythrocyte membranes. Modern therapy for microcirculatory disorders is based on the results of laboratory studies of hemostasis and blood rheology. If microcirculatory disorders are caused by intravascular thrombus formation, antiplatelet agents are used for treatment. Hyperviscosity of blood plasma is compensated by reducing glucose levels and administering polyunsaturated fatty acids
(Omega-3, Omega-6) or statins for hypercholesterolemia. Erythrocyte microcirculatory block is eliminated by xanthine derivatives or ortho-taurine. To some extent, microcirculatory disorders are eliminated by nicotinic acid preparations due to their effect on the activation of fibrinolysis.
Metabolic therapy
The influence on metabolic processes of ischemic brain tissue is one of the leading directions of therapeutic tactics for DE [7,8]. The possibility of influencing such important processes as oxidative damage to cells, membrane permeability, and restoration of energy capabilities looks extremely attractive. It is only necessary to remember that the implementation of therapeutic efforts aimed at restoring the metabolism of nervous tissue is possible only with the restoration of central hemodynamics and the elimination of microcirculatory disorders.
Metabolic therapy for DE can have different application points. have found widespread use in practice :
vitamins A, E, C in various combinations or in a complex, solcoseryl, etc. An indispensable condition for successful treatment of DE should be considered the inclusion of phospholipid complexes in treatment programs.
Phospholipids are necessary for the construction of cell membranes and myelin. Traditional “activators” of nervous tissue metabolism such as piracetam and others demonstrate high efficiency [9]. In recent years combination drugs
, constituting an optimal combination of components that affect the metabolism of neurons, of which
Fezam
. This is a combination drug containing 400 mg of piracetam and 25 mg of cinnarizine. The combination of two components enhances the antihypoxic effect and reduces the tone of the smooth muscles of cerebral vessels. The drug has moderate antiplatelet activity, stimulates metabolic processes in the central nervous system, and increases the integrative abilities of the brain. Phezam has significantly fewer side effects than its individual components and is ideal in cases where the use of piracetam alone causes tension and insomnia in the patient, and cinnarizine causes drowsiness. In this regard, it can be recommended to a working group of patients, since when treated with Phezam, driving vehicles and working with machinery are allowed.
A promising area of metabolic therapy is associated with the use of neurospecific peptides
. Low molecular weight peptides (cerebrolysin, cytamines) obtained from brain tissue have multidirectional effects in conditions of chronic cerebral ischemia. They help restore interneuronal connections, exhibit a stimulating effect, and contribute to the restoration of lost functions. Activation of disrupted interneuronal connections is promoted by memantine, used for various types of dementia. Restoration of movement disorders - pronoran. The use of regulatory peptides for DE should be considered quite justified. Of the regulatory peptides already used in clinical practice, melatonin should be mentioned. Melatonin is a low molecular weight peptide secreted by the pineal gland. The biological effects of melatonin go far beyond the “regulation of the day-night cycle” [10]. It influences the circadian rhythms of blood pressure and takes part in the adaptation of the neuroendocrine system to changing environmental conditions.
Thus, an analysis of modern treatment options for DE shows that in most cases these opportunities are not fully used. Simplified, standardized prescription of “vasodilator” drugs and nootropics in most cases does not lead to a sustainable improvement in the condition of patients. At the same time, the abundance of drugs of various groups that are potentially useful in the treatment of DE should not push the doctor to polypharmacy. It is advisable to divide the entire treatment cycle into three periods:
1) stabilization of central, cerebral hemodynamics and microcirculation;
2) the use of antioxidants, vitamins, phospholipid and peptide complexes;
3) the use of regulatory peptides and nootropics.
Effective treatment of DE can only be with long-term use of complex regimens that take into account data from additional studies, including indicators of central and cerebral hemodynamics, laboratory tests reflecting the state of lipid metabolism and hemostasis.
Literature:
1. Gusev E.I., Skvortsova V.I. Cerebral ischemia. M.: Medicine. 2000. –328 p.
2. Yakhno N.N., Damulin I.V. Dyscirculatory encephalopathy in the elderly // Breast cancer. 1997; 5:20.
3. Simonenko V.B., Shirokov E.A. Fundamentals of cardioneurology: A guide for doctors. 2nd ed. M.: Medicine, 2001.–240 p.
4. Bokarev I.N. Atherosclerosis is a modern problem. Thrombosis, hemostasis and rheology. –2000; 1:6–7.
5. Hankey GJ, Warlow CP Treatment and secondary prevention of stroke: evidence, costs, and effects on individuals and populations/ The Lancet. 1999; 354:1457–63.
6. Shirokov E.A., Leonova S.F. Disturbances of hemostasis and rheological properties of blood in patients with a high risk of stroke / Journal of Neurology and Psychiatry named after. S.S. Korsakova. Stroke: supplement to the journal. Vol. 9. 2003. –S. 140.
7. Perry IJ Homocysteine and risk of stroke//J. Cardiovascular risk. 1999; 6(4): 235–40
8. Shirokov E.A., Frolova O.P. Pycnogenol and coenzyme Q–10 in the complex therapy of dyscirculatory encephalopathy/New methods of diagnosis and treatment in military and clinical medicine. –M., 1998. –S. 283.
9. Shirokov E.A. New opportunities in the treatment of diseases of the nervous system//Medicina altera (Journal of the International Academy of Sciences of Nature and Society). –July/September 1999. –p. 26 – 29.
10. Zaslavskaya R.M. Chronodiagnosis and chronotherapy of diseases of the cardiovascular system. –M.: medicine. –1991.–320 p.
Symptoms
Signs of encephaloptia depend on the location of the source of destruction, as well as the degree of development of the disease. Most often, patients and their relatives experience the following symptoms:
- headache: can involve the entire head or concentrate in certain areas; the intensity depends on the degree of damage and gradually increases; pain is poorly relieved by taking analgesics;
- dizziness: occurs sporadically, accompanied by loss of orientation in space; Often a person is forced to wait out this condition in bed, since the slightest movement worsens the symptom; the condition is often accompanied by constant nausea and vomiting;
- impairment of cognitive functions: a gradual decrease in the ability to think adequately is a characteristic sign of encephalopathy; a person gradually becomes forgetful, absent-minded, has trouble concentrating on a specific process and has difficulty switching between different activities;
- emotional and behavioral disorders: a person has difficulty controlling his emotions, becomes irritable, whiny, gets excited quickly; as the disease progresses, apathy, depression and complete reluctance to do anything arise;
- increase or decrease in muscle tone; often accompanied by hyperkinesis (trembling in the limbs, obsessive movements, etc.);
- decreased vision and hearing;
- increased weather sensitivity.
In some patients, behavioral disorders predominate, others cease to have normal control of their body; in others, it is mainly the sense organs that are affected. In severe cases, a person requires constant care and supervision of others.
Early symptoms
DEP begins unnoticeably and develops quite slowly. First of all, problems in the emotional sphere are noted. About 65% of patients suffer from depression, which, unlike depressive neurosis, occurs against the background of minor traumatic situations, while patients are not inclined to note depression and low mood. They are fixed on various somatic disorders, like patients with hypochondriacal neurosis. Complaints may include:
- Arthralgia;
- Back pain;
- Neuralgia;
- Noise in the head;
- Tinnitus;
- Pain of various localizations.
Their distinctive feature is that they do not fit into the clinical picture of supposed somatic pathologies. Depression in DEP is difficult to respond to psychocorrection and treatment with antidepressants.
The initial stage of DEP often manifests itself in increased emotional lability, which includes:
- Sudden mood swings;
- Cases of uncontrollable crying for minor reasons;
- Irritability;
- Attacks of aggressive behavior towards others.
In addition, sleep disturbances, fatigue, headaches, and absent-mindedness are noted. The symptomatic picture is similar to neurasthenia, but with dyscirculatory encephalopathy the symptoms are combined with cognitive impairment.
Moreover, in 90% of patients, cognitive impairment occurs at the initial stage of the disease. These include:
- Decreased concentration;
- Memory impairment;
- Reduced speed of thinking;
- Difficulties in planning activities;
- Fatigue with mental effort;
- Problems with speech reproduction of information while maintaining memory.
Movement disturbances, such as dizziness and unsteadiness when walking, may also occur. DEP must be differentiated from vestibular ataxia, since nausea and vomiting may be present, but only during walking.
Complications
Complications of encephalopathy are associated with severe and irreversible damage to the brain and represent the extreme extent of the symptoms observed:
- loss of self-care ability due to motor or cognitive impairment;
- dementia: loss of knowledge and skills up to complete collapse of personality;
- loss of vision and hearing;
- severe mental disorders;
- convulsions;
- disturbances of consciousness: stupor, coma;
- death.
Symptoms of encephalopathy
Symptoms characteristic of encephalopathy:
- memory impairment;
- pain and noise in the head;
- absent-mindedness;
- dizziness;
- depression to the point of wanting to die;
- high fatigue;
- irritability for no apparent reason;
- physical weakness even after proper rest.
The symptoms are quite common and may not only relate to encephalopathy. Only a complete examination prescribed by a doctor can clarify the real picture.
A medical examination of the patient reveals an apathetic state, confusion in thoughts and reasoning, speech problems (difficulty pronouncing words). Patients have severe daytime sleepiness and a significant narrowing of the range of interests in everyday life.
Various diagnostic methods are used to confirm the diagnosis.
Diagnostics
A neurologist is involved in the diagnosis and treatment of encephalopathy. Patient examination includes:
- survey: collection of complaints and anamnesis; it is mandatory to clarify information about previous diseases, injuries, risk factors, the time of the first violations, the rate of development, etc.;
- neurological examination: assessment of reflexes, sensitivity, muscle strength, motor function;
- electroencephalography (EEG): assessment of electrical impulses arising during brain function; allows you to identify signs of epilepsy, inflammation, the presence of tumors, etc.;
- Doppler ultrasound of the vessels of the brain and neck: assesses the quality of blood flow in large vessels, identifies areas of narrowing, assesses the volume of incoming blood;
- rheoencephalography: complements ultrasound, allows you to assess the tone and elasticity of blood vessels, detect blood clots;
- angiography: X-ray examination of blood vessels by introducing a contrast agent into them;
- CT and MRI: allow you to detect foci of sclerosis, tumors, inflammatory foci, consequences of stroke and other structural changes;
- blood tests (general, biochemical): make it possible to evaluate the functioning of the kidneys, liver, pancreas, and identify toxins that can affect the condition of the brain.
If necessary, other tests and examinations may be prescribed, as well as specialist consultations to accurately determine the cause of encephalopathy.
Make an appointment
What is cerebral encephalopathy?
Encephalopathy is a group of brain diseases of a non-inflammatory nature. The disease can manifest itself in people of different age categories, with corresponding distinctive features. Treatment of encephalopathy involves a comprehensive diagnosis. Starting from identifying the causes of the disease, ending with courses of medication, manual and physical therapy. A general classification divides encephalopathic pathology into perinatal and acquired.
The congenital form of encephalopathy is a consequence of negative intrauterine effects on the fetus, genetic inheritance or birth trauma. This type, although rare, is the most severe in its manifestations and often leads to disability.
The acquired form of cerebral encephalopathy is more common. Acts as a consequence of severe systemic diseases of the body, injuries, exposure to harmful external factors. In medicine, there are several stages of encephalopathy:
- Subjective neurological symptoms; mild neuropsychiatric disorders.
- Clinically defined neurological syndrome; significant neuropsychic disorders.
- Several syndromes; dementia is a severe neuropsychiatric disorder.
Where does this unpleasant, dangerous disease come from?
Treatment
The sooner treatment for encephalopathy is started, the greater the chance of stopping the progression of the pathology and restoring full brain function.
First of all, it is necessary to eliminate the cause of neuronal damage:
- adjust blood sugar levels;
- stabilize blood pressure;
- restore the functioning of the liver, kidneys, pancreas;
- reduce blood cholesterol levels;
- remove toxins;
- normalize hormone levels, etc.
Direct treatment of encephalopathy requires the prescription of drugs that improve blood flow in the vessels of the brain and metabolism within the cell. Depending on the cause and extent of the lesion, doctors may prescribe:
- nootropics (Cerebrolysin, piracetam): aimed at enhancing metabolism;
- blood thinners (aspirin, pentoxifylline, etc.): help accelerate blood flow, prevent the formation of blood clots;
- antioxidants: neutralize toxins;
- angioprotectors (Cavinton, nicotinic acid and others): necessary to accelerate blood circulation and metabolism;
- vitamin-mineral complexes, amino acids;
- symptomatic drugs: sedatives, anticonvulsants, etc.
For encephalopathy, courses of treatment are carried out regularly, at least 2 times a year. This allows you to keep the disease under control. The selection of specific drugs and determination of dosage is carried out only by a doctor. There is no single treatment regimen for all patients.
To enhance the effect of drugs, non-drug treatment methods are used:
- physiotherapy (reflexotherapy, electrophoresis, magnetic therapy, laser therapy);
- physical therapy to improve muscle condition and facilitate control over them;
- massage to relax and improve blood circulation;
- acupuncture.
In some cases (with the vascular nature of encephalopathy), it is necessary to resort to surgical treatment:
- elimination of a blood clot from the lumen of blood vessels;
- expansion of narrowed sections of the artery with the installation of a stent that supports the walls in the correct position;
- bypass: restoration of blood flow by creating an alternative path that bypasses the affected area.
Methods for diagnosing DEP
It is very important to make a diagnosis as early as possible in order to promptly begin vascular therapy to compensate for neurological disorders. Therefore, all patients at risk for discirculatory encephalopathy must be regularly examined by a neurologist. The risk group includes:
- People suffering from atherosclerosis;
- Diabetics;
- Hypertensive patients;
- Aged people.
To identify cognitive impairment, special tests are required. Tasks may include the need to remember and repeat a list of words named by the doctor, draw a dial with a given time, or repeat certain words.
In addition, consultation with an ophthalmologist and ophthalmoscopy, determination of visual fields, will be required. The following hardware diagnostic methods are shown:
- Echo-EG;
- EEG;
- REG;
- ECG and daily ECG monitoring;
- Doppler ultrasound of head and neck vessels;
- MRA of cerebral vessels;
- Duplex scanning;
- MRI of the brain.
MRI of the brain will help distinguish DEP from other pathologies: Alzheimer's disease, Creutzfeldt-Jakob disease, disseminated encephalomyelitis. Magnetic resonance imaging makes it possible to visualize foci of silent infarctions, while areas of leukoaraiosis and cerebral atrophy also occur in other neurodegenerative pathologies.
To detect etiological factors, consultation with a cardiologist and nephrologist, blood pressure monitoring, a coagulogram, determination of lipoproteins and cholesterol in the blood, and a blood sugar test are required.
Prevention
Encephalopathy is a complex disease. There is no clear method to prevent its occurrence and eliminate all risk factors. Doctors recommend adhering to the following rules:
- provide yourself with a full daily routine with alternating work and rest, a full night’s sleep;
- minimize stress;
- eat properly and balanced, avoid overeating and excess body weight;
- ensure sufficient supply of vitamins and microelements;
- quit smoking, drugs, alcohol;
- exercise in moderation (not professionally);
- promptly identify and treat chronic diseases: hypertension, diabetes, atherosclerosis;
- consult a doctor at the first signs of trouble.
Causes of the disease
Dyscirculatory encephalopathy in older people is formed against the background of existing chronic pathologies, which become more active against the background of physiological aging and provoke the occurrence of complications. Experts identify the following causes of the disease :
- Atherosclerosis. The deposition of atherosclerotic plaques on the walls of blood vessels leads to a slowdown in blood flow and can cause complete blockage of the vessel;
- Hypertension. Increased arterial and intracranial pressure has a negative effect on the condition of blood vessels. However, intermittent hypertension is especially dangerous;
- Osteochondrosis of the cervical spine. The disease causes displacement of the bones and processes of the spinal column, which provokes compression of the arteries that supply nutrients and oxygen to neurons;
- Traumatic brain injuries. Serious damage to brain structures can lead to impaired blood flow and hemorrhage;
- Obesity. The deposition of fatty tissue in the neck area provokes a change in its shape, as a result, the functioning of the neck vessels is disrupted;
- Smoking and drinking alcohol. This leads to disruption of the normal functioning of blood vessels, causing the death of brain neurons;
- Vegetative-vascular dystonia (VSD). The disease provokes an increase or decrease in pressure, which negatively affects the condition of blood vessels.
The listed pathologies can cause the development of encephalopathy in young patients, but in such cases the diseases develop much more slowly. In older people, the body's resistance and the intensity of recovery processes decrease, so rapid exhaustion is observed. As a result, dyscirculatory encephalopathy develops more intensively.
Treatment at the Energy of Health clinic
Doctors at the Health Energy Clinic are always ready to see patients of any age. We will conduct a thorough examination, identify possible causes of encephalopathy and take all measures to eliminate it:
- we will prescribe the most appropriate therapy, describe the course of treatment and the frequency of its repetition;
- We will carry out all the necessary manipulations (placement of a drip, intravenous and intramuscular injections) in the comfortable conditions of a day hospital and manipulation room;
- We will complement the therapy with modern physiotherapeutic procedures;
- We will conduct a massage course and prescribe exercise therapy for maximum effectiveness.
Our neurologists will monitor the patient’s condition and adjust treatment if necessary. Treatment of encephalopathy is a long and complex process, but we are ready to take on it.
Alcoholic encephalopathy
Alcoholic encephalopathy is a disease accompanied by the destruction of brain cells under the influence of alcohol.
The disease, as a rule, occurs shortly before the transition or after the transition from stage II of alcoholism to stage III. The duration of constant alcohol use before the onset of the first symptoms ranges from 7 to 20 years, but an earlier onset of the disease is possible. In some cases, symptoms may occur in the absence of alcoholism due to periodic alcohol consumption. Alcoholic encephalopathy is a serious disease and requires early, qualified treatment. The number of deaths from this pathology, according to various specialists in the field of addiction, is 30-70%. In other cases, the outcome, as a rule, is mental disorders of varying severity. The development of psychoorganic syndrome, pseudoparalytic syndrome or dementia is possible. Treatment of alcoholic encephalopathy is long-term and carried out in a narcological hospital.
Advantages of the clinic
If you require a full examination and high-quality treatment, welcome to the Health Energy clinic. Here you are waiting:
- experienced specialists who regularly improve their skills to keep abreast of all new trends in the world of medicine;
- modern diagnostic equipment;
- everything necessary for physiotherapy, massage, exercise therapy;
- own day hospital for slow drip administration of medications;
- affordable prices for all services.
If you or your relatives have signs of encephalopathy, do not delay contacting a doctor. The sooner treatment is started, the better the result. Sign up for the Health Energy clinic and let our doctors choose the optimal therapy.
Clinical picture
The symptoms of dyscirculatory encephalopathy in older people are determined by the area of the brain in which pathological processes develop and the stage of the pathological process. The following periods are distinguished in the pathogenesis of the disease:
- First stage characterized by the occurrence of symptoms, which are often attributed to the physiological process of aging. Patients report weakness, dizziness, sleep disturbances, headaches, and decreased performance. During dizziness, tinnitus may appear, hearing and visual acuity may decrease, and sensitivity on one side may be impaired. Patients become irritable, tearfulness and depression may appear.
- The second stage is characterized by an increase in neurological symptoms. Patients complain of frequent dizziness, headaches, decreased visual acuity, hearing, and sensitivity. Memory, intellectual abilities, and concentration often decrease. Against the background of impaired coordination of movements, patients move uncertainly and begin to shuffle. Sometimes the appearance of pathological reflexes and tics is diagnosed. Many patients experience speech disturbances, their voice becomes nasal, and insomnia occurs at night. Gradually, a person develops personality degradation. As a result, elderly patients develop anxiety, irritability, and aggressiveness.
- At the last stage, patients lose the ability to self-care - they need constant help from loved ones or medical personnel. A person’s memory and intelligence sharply decrease, and dementia may develop. Patients become more aggressive, irritable, whiny, and conflictual. Elderly people note the appearance of intense headaches, tinnitus, the appearance of veils or dark spots before the eyes, and decreased hearing. It is possible to develop pseudobulbar syndrome, which leads to speech impairment, hoarseness, and the inability to swallow independently.
Diagnosis and treatment of alcoholic encephalopathy
The diagnosis is made on the basis of anamnesis and clinical symptoms; a differential diagnosis is made with other forms of psychosis, schizophrenia, malignant and benign brain tumors. Treatment involves the selection of a balanced menu high in proteins and vitamins. Patients are prescribed high doses of thiamine, nootropics, and drugs to improve cerebral circulation and activate metabolism in the brain. Concomitant somatic pathology is treated.
The most important role in the successful treatment of alcoholic encephalopathies, minimizing residual effects and preventing the transition of the acute form of the disease to chronic encephalopathy is played by complete abstinence from alcohol. The choice of tactics and methods of treating alcohol addiction is determined by a narcologist individually, depending on the specific case. It is possible to sew in an implant, use medicinal treatment methods, hypnosuggestive therapy or Dovzhenko coding. It is advisable to carry out comprehensive rehabilitation with subsequent supervision by a specialist, visits to a psychotherapist or support groups.
Acute alcoholic encephalopathies
First, symptoms and warning signs of the disease appear. Asthenia occurs in combination with sleep and appetite disorders. Patients feel an aversion to foods rich in fats and proteins and prefer foods high in carbohydrates, which worsens existing metabolic disorders. Sometimes anorexia develops. Disturbances in the gastrointestinal tract are detected. Nausea and vomiting often occur (especially in the morning). Abdominal pain, belching, heartburn and stool disorders are possible. The physical condition of patients quickly deteriorates, weight decreases, and exhaustion increases. Signs of alcoholic polyneuropathy may be detected.
Gaye-Wernicke encephalopathy in its classical form begins with delirium of moderate severity. Patients experience monotonous, fragmented visual illusions and hallucinations combined with complex, repetitive movements. Periods of agitation are followed by short episodes of immobility, and muscle tone remains elevated during such episodes. Patients mutter or shout something, and productive communication becomes impossible.
There is swelling of the face in combination with general exhaustion. Ataxia occurs, multiple neurological disorders are detected (nystagmus, different pupil sizes, mild paresis, etc.). Body temperature is elevated, pulse and respiration are rapid, and there is a tendency to decrease blood pressure as the general condition worsens. On the part of the digestive system, a change in the color of the tongue (crimson) and an enlargement of the liver are detected. Possible stool disturbances. As clinical symptoms worsen, progressive disturbances of consciousness arise - from mild stupor to stupor. In severe cases, coma develops.
Death can occur within 10-15 days from the onset of the first symptoms of delirium. The likelihood of death increases with the addition of intercurrent diseases - pneumonia, bedsores, etc. With favorable developments, delirium lasts from 3 weeks to 1.5 months. The outcome of the disease is a psychoorganic syndrome, expressed in mental helplessness, memory impairment and loss of the ability to adapt to normal everyday life. In patients, the volitional sphere suffers, the ability to work and the level of resistance to stress decreases. The transition of acute alcoholic encephalopathy to chronic is possible.
Mitigated acute encephalopathy begins with precursors in the form of asthenia, deterioration of mood, loss of appetite and sleep disorders. There is marked anxiety and a tendency towards hypochondria. Neurological disorders are represented by mildly expressed neuritis. The prodromal period lasts 1-2 months, then delirium develops. After recovery from psychosis, residual effects are observed in the form of asthenia and long-term memory disorders that are difficult to correct medically.
The hyperacute form of alcoholic encephalopathy is characterized by rapid development and an unfavorable course with frequent deaths. The duration of the precursor period is about 3 weeks. Then severe psychosis occurs, accompanied by severe neurological and somatic disorders. Body temperature rises to 40-41 degrees, progressive disturbances of consciousness are observed. Within a few days, coma occurs and then death. In surviving patients, after the end of delirium, a pseudoparalytic syndrome develops - carelessness, a feeling of complete satisfaction with oneself and others, combined with a lack of criticism, overestimation of one’s capabilities and ridiculous behavior.