Perinatal encephalopathy of newborns is an unclassified non-inflammatory disorder of the nervous system observed during pregnancy or immediately after birth.
The disease is called unclassifiable because encephalopathy is not detected by traditional tests. Even high-tech research does not provide a complete objective picture.
The concept of perinatal encephalopathy (PE) is excluded from the International Classification. Today, encephalopathy is defined as the consequences of damage to the fetal brain. If we adhere to the accuracy of terminology, then encephalopathy can be called a consequence of destructive manifestations that destroy the cerebral cortex.
Causes of perinatal encephalopathy.
Signs of pathology are often vague. To identify the problem, dynamic observation over a long period of time is sometimes required. There is evidence that at the initial appointment with a neurologist, up to 80% of children receive a diagnosis of PPE or “unspecified perinatal encephalopathy.” It is reassuring to know that by the age of one year, most children are cleared of their diagnosis. This can be explained by the lack of clear diagnostic criteria and the mobility of the infant’s neuropsychological structure. Perinatal encephalopathy is an organic and functional disorder of the brain in children during the days of intrauterine development and the first hours of life. The time limits are determined as follows: from the 28th week of pregnancy to the 7th day after birth. In premature babies, the period is extended to 28 days.
The seriousness of the disease and the difficulty of diagnosis are not a death sentence. The main factors that cause the disease still exist:
- Hypoxia is a lack of oxygen and is ischemic in nature. When oxygen supply stops, the blood stops supplying food and fills with carbon dioxide. This compound provokes cell oxidation. As a result, acidosis appears (body oxidation syndrome) - a disorder of the acid-base balance. Its most dangerous consequence is swelling.
Hypoxia can have both destructive and restorative effects. Immediately after the baby leaves the womb, acidosis acts as a means of adaptation to changes in its environment. When its form is prolonged, encephalopathy of newborns manifests itself.
With a complicated birth, asphyxia occurs - oxygen starvation of the children's brain. Then uncompensated acidosis may occur. As a result of a disruption in the blood supply to the brain, the acid-base balance changes (it is measured by pH). If the baby has uncompensated acidosis, the indicator drops below 7.1, which requires immediate resuscitation measures.
- Cranial trauma. It entails post-traumatic encephalopathy. As a result of a difficult birth, the child experiences mental and physical disorders. Depending on the severity of the injury, neonatal encephalopathy can be expressed in different forms.
- Damage to the frontal or temporal lobes of the brain at the time of birth;
- Swelling of the brain, disruption of the blood supply to cells by connecting material: this causes adhesions and scars;
- Autoneurosensitization is a conflict of the immune system: it mistakenly begins to react to its own cells as a foreign object.
- Toxic-metabolic syndrome is the result of the toxic effects of the metabolic activity of unhealthy kidneys and biliary tract in children. Bilirubin encephalopathy (jaundice of newborns), i.e. bilirubin intoxication, is quite widespread. Bilirubin is a neurotoxic poison that leads to damage to the cerebral cortex and subcortical nuclei. Depending on the causes, there are several types of jaundice in newborns: conjugative (low binding capacity of the liver), hemolytic (caused by hemolysis - destruction of red blood cells), obstructive (problems with the outflow of bile), parenchymal.
- Intrauterine infections infect the newborn and provoke inflammatory processes. Infection of the fetus can lead to serious pathology of the nervous system, perinatal encephalopathy, premature birth and even the death of the child.
- Disruption of uteroplacental blood flow (fetoplacental insufficiency) is a failure of blood circulation in the placenta in the late period of gestation. Through this protective shell the fetus is nourished, supplied with oxygen, and hormonal exchange occurs. When the dysfunction is insignificant, the danger is minimal, but with severe fetoplacental insufficiency, hypoxia occurs, followed by encephalopathy.
- Severe chronic or acute illness of the mother also negatively affects the child. Preeclampsia is a complication of the late period of pregnancy, it is called late toxicosis. As a result of the disease, the internal structures of the mother (kidneys, liver, blood circulation) are damaged.
- The threat of termination of pregnancy is fraught with many negative side effects, including the above factors.
What are the risk factors and causes of hypoxic-ischemic encephalopathy?
Asphyxia is the most significant risk factor for HIE. The degree and duration of oxygen starvation determines whether hypoxic-ischemic encephalopathy will develop or not, and how serious the consequences will be. Factors that can lead to asphyxia:
- Acute maternal hypotension
- Blood containing less oxygen due to poorly functioning lungs
- Heart complications
- Injuries from a clinically narrow pelvis
- Injuries from complications of the umbilical cord
- Poor blood supply to the brain during childbirth
- Respiratory arrest or hypoxia
- Bleeding during childbirth
- Medical negligence
- Umbilical cord prolapse
- Placental abruption
- Pressure on the skull with changes in its shape, resulting in bleeding or ischemia
- Low placenta previa
- Stress during childbirth
- Injury
- Uterine rupture
Fetal stroke also increases the likelihood of developing hypoxia-ischemic encephalopathy. Factors that can lead to fetal stroke include:
- Blood clotting disorders
- Impaired blood flow in the placenta
- Abnormal blood vessels that can rupture
- High or low blood pressure in mother
- Infections in the mother, especially pelvic inflammatory disease
Diagnosis of encephalopathy.
Symptoms in children do not appear immediately. Immediately establishing the level and nature of the problem in the first days after birth can be difficult.
Sometimes natural manifestations of the nervous organization of a newborn are mistaken for symptoms of encephalopathy, in other cases the disease goes unnoticed. Objective conclusions can often be drawn only after six months. According to the rules, a child is examined by a doctor every month in the first half of his life. The doctor examines the baby’s reflexes and determines the quality of his physical development. In a fairly short period of time, it is possible not only to diagnose an anomaly, but also to successfully correct it. Long-term follow-up may be required so that the diagnosis does not give rise to doubts, and the development of a treatment regimen for the disease becomes possible.
The depth of damage to a child’s brain varies. Depending on the severity of the disease, 3 levels of brain destruction with long-term consequences have been established:
- The initial stage of the disease is characterized by a slight slowdown in the motor development of children for more than 2 weeks. In the first degree, fortunately, the brain substances are not affected.
- Deviations of moderate severity are determined by the presence of convulsions when crying, the baby’s motor skills are 8 weeks behind, hyperexcitability, cyanosis with short crying, “marbling” of the skin, twitching of the arms and legs. Muscle hypertonicity develops, adaptation syndromes are revealed. A year later, the disease “offers” new symptoms (when trying to walk, the child leans on his toe). Lack of treatment in the future threatens serious deviations.
- Deep brain damage results in cerebral palsy (CP) and autism. The help of restorative medicine should be resorted to as early as possible.
Degrees of severity and characteristic symptoms
Hypoxic-ischemic encephalopathy has 3 degrees of severity, which are characterized by their own manifestations. Using them, doctors often give a preliminary description of brain damage and an approximate prognosis.
Mild degree
With this degree the patient will have:
- the pupil is dilated and the eyelids are wide open;
- lack of concentration;
- impaired coordination of movements, wandering behavior;
- either drowsiness or hyperexcitability was detected;
- high degree of irritability;
- lack of appetite;
- cerebral circulation is impaired.
Average degree
Neurology with it will be more pronounced, since the disturbance in oxygen saturation of the brain is longer lasting:
- the baby has spontaneous cries for no reason;
- the protective and support reflex is either weakened or absent altogether;
- signs of muscle weakness;
- drooping upper eyelid;
- increased cerebrospinal fluid pressure;
- metabolic acidosis of the blood;
- neuralgic attacks;
- failure in the swallowing process.
Severe degree
The damage in such cases is more severe, which manifests itself in:
- convulsions;
- bluish skin;
- loss of consciousness;
- hypertension;
- lack of motor abilities;
- strabismus;
- coma or precoma;
- lack of pupil reaction to light;
- failure of the respiratory process with severe arrhythmia;
- tachycardia.
PEP is a type of hypoxic-ischemic encephalopathy in young children. It is diagnosed both immediately after birth and in the first year of life. PEP develops both in utero, during labor, and in the first 10 days from birth.
It can be of three degrees of severity with characteristic symptoms and occur in an acute form - up to a month, with early restoration of functions - up to 4 months, with late recovery - up to 2 years.
What should alert parents?
The peculiarity of encephalopathy is the need for the earliest possible start of stabilization and elimination of neurological defects of the fetus.
Emerging syndromes can be stopped and corrected during pregnancy and infancy, but qualified assistance from a neurologist is required.
Particular responsibility falls on parents. One of the features of the child’s behavior or well-being should cause concern:
- sleep disorders;
- muscle hypertonicity;
- poor coordination;
- lethargy of the hands;
- does not turn over;
- legs are not involved in crawling;
- does not sit down or stand up;
- improper crawling;
- increased excitability to various stimuli (frequently cries);
- depressed appearance in the waking phase;
- delayed motor development syndrome (cannot pick up a toy);
- can only do pull-ups with his right arm;
- spitting up like a fountain after eating;
- tremor – fine muscle trembling;
- body weight slowly increases;
Such symptoms force you to go to the clinic. Important preventive measures should not be neglected, even if the child seems to be healthy.
What is important to do in time:
- Thorough examination by a neurologist at the age of 4 weeks.
- Regular monthly examination by a pediatrician, and if necessary, treatment of the disease.
- Do a neurosonography test - NSG (establishes movement disorder syndrome).
If the presence of cerebral palsy or epilepsy has already been established, it is necessary to begin treatment as quickly as possible to prevent further pathology.
Symptoms of hypoxic-ischemic damage to the central nervous system
Damage to the central nervous system in newborns is diagnosed in the first minutes of a baby’s life, and the symptoms depend on the severity and depth of the pathology.
I degree
In mild cases of HIE, the condition remains stable; the child’s Apgar score is no less than 6-7 points; cyanosis and decreased muscle tone are noticeable. Neurological manifestations of the first degree of hypoxic damage to the central nervous system:
- High neuro-reflex excitability;
- Sleep disorders, anxiety;
- Trembling of the limbs, chin;
- Possible regurgitation;
- Reflexes can be either increased or decreased.
The described symptoms usually disappear during the first week of life, the child becomes calmer, begins to gain weight, and severe neurological disorders do not develop.
II degree
With moderate brain hypoxia, signs of brain depression are more obvious, which is expressed in deeper disorders of brain function. Typically, the second degree of HIE accompanies combined forms of hypoxia, which is diagnosed both during the intrauterine growth stage and at the time of birth. In this case, muffled fetal heart sounds, increased rhythm or arrhythmia are recorded; the newborn scores no more than 5 points on the Apgar scale. Neurological symptoms include:
- Suppression of reflex activity, including sucking;
- A decrease or increase in muscle tone, spontaneous motor activity may not appear in the first days of life;
- Severe blueness of the skin;
- An increase in intracranial pressure;
- Autonomic dysfunction - respiratory arrest, increased heart rate or bradycardia, disturbances in intestinal motility and thermoregulation, tendency to constipation or diarrhea, regurgitation, slow weight gain.
intracranial hypertension accompanying severe forms of HIE
As intracranial pressure increases, the baby's anxiety increases, excessive sensitivity of the skin appears, sleep is disturbed, tremor of the chin, arms and legs increases, bulging of the fontanelles becomes noticeable, horizontal nystagmus and oculomotor disorders are characteristic. Signs of intracranial hypertension may include seizures.
By the end of the first week of life, the condition of a newborn with the second degree of HIE gradually stabilizes against the background of intensive treatment, but neurological changes do not disappear completely. Under unfavorable circumstances, the condition may worsen with brain depression, decreased muscle tone and motor activity, exhaustion of reflexes, and coma.
III degree
Perinatal damage to the central nervous system of severe hypoxic-ischemic origin usually develops with severe gestosis in the second half of pregnancy, accompanied by high hypertension in the pregnant woman, impaired renal function, and edema. Against this background, a newborn is already born with signs of malnutrition, intrauterine hypoxia, and developmental delay. The abnormal course of labor only aggravates the existing hypoxic damage to the central nervous system.
In the third degree of HIE, the newborn has signs of severe circulatory disorders, there is no breathing, tone and reflexes are sharply reduced. Without urgent cardiopulmonary resuscitation and restoration of vital functions, such an infant will not survive.
During the first hours after birth, a sharp depression of the brain occurs, a coma sets in, accompanied by atony, an almost complete absence of reflexes, dilated pupils with a reduced reaction to a light stimulus or its absence.
The inevitably developing cerebral edema is manifested by generalized convulsions, respiratory and cardiac arrest. Multiple organ failure is manifested by increased pressure in the pulmonary artery system, decreased urine filtration, hypotension, necrosis of the intestinal mucosa, liver failure, electrolyte disturbances, and blood coagulation disorders (DIC).
A manifestation of severe ischemic damage to the central nervous system is the so-called post-asphyxial syndrome - babies are inactive, do not cry, do not respond to pain and touch, their skin is pale bluish, and a general decrease in body temperature is characteristic. Important signs of severe brain hypoxia include swallowing and sucking disorders, which make natural feeding impossible. To save the life of such patients, intensive care in intensive care is necessary, but the unstable condition still persists until the 10th day of life, and the prognosis often remains poor.
A feature of the course of all forms of HIE is considered to be an increase in neurological deficit over time, even with intensive therapy. This phenomenon reflects the progressive death of neurons that have already been damaged during a lack of oxygen, and also determines the further development of the baby.
In general, ischemic-hypoxic damage to the central nervous system can occur in different ways:
- Favorable with rapid positive dynamics;
- Favorable course with rapid regression of neurological deficit, when by the time of discharge the changes either disappear or remain minimal;
- Unfavorable course with progression of neurological symptoms;
- Disability during the first month of life;
- Latent course, when after six months motor and cognitive disorders increase.
In the clinic, it is customary to distinguish several periods of ischemic encephalopathy of newborns:
- Acute - first month.
- Restorative - within one year.
- Period of long-term consequences.
The acute period is manifested by the whole gamut of neurological disorders from barely noticeable to coma, atony, areflexia, etc. During the recovery period, the syndrome of excessive neuro-reflex excitability, convulsive syndrome, possible hydrocephalus, delayed intellectual and physical development come to the fore. As the child grows, the symptoms change, some symptoms disappear, others become more noticeable (speech disorders, for example).
Osteopathy in the correction of neonatal encephalopathy.
Organic disorders of brain development in infants must be identified and treated immediately.
Due to neural disorders, diseases of the child’s internal organs occur. The damaged network begins to control the entire body. The opposite effect also occurs: normalization of the kidneys, liver, and lungs affects neural connections. Therefore, when stabilizing the brain, it is necessary to take into account the overall picture of the body’s development and look for options for complex treatment.
Osteotherapy is one of the branches of restorative medicine. A person is considered as a single holistic scheme. The basic principles of the technique were proclaimed more than 30 years ago. Over several decades, new approaches have been developed, management methods have been found, and practical experience has been acquired. Medications are used with great caution or are not used at all. Treatment occurs through the mobilization of all elements included in recovery. The advantage of this area of medicine is that drugs are practically not used. The child activates his internal reserves. Complex treatment is the basis of the theory.
The following osteopathic directions have been identified:
craniosacral
structural
visceral
fascial
1. Craniosacral method of treatment.
The craniosacral (cranium-skull, sacrum-sacrum) pathway is based on the theory that the bones of the skull are movable (previously it was believed that only the lower jaw was movable). The dynamics of their movement are imperceptible and strictly obey the impulses of the brain. If the body as a whole and the main control center are functioning normally, then the rhythm of movement of the elements of the skull is clear and correct. Failure of brain impulses against the background of encephalopathy indicates deviations from the norm. The study of the rhythmic movement of children's cranial areas is used not only for diagnosing and identifying nervous destruction, but also for the reverse process. Through the systematization of impulses, it is possible to influence the damaged area. This method is especially effective in eliminating the consequences of encephalopathy.
Treatment of areas of the brain eliminates the symptoms of the disease, normalizes intracranial pressure in children and can lead to restoration of the affected areas.
2. Structural method.
The musculoskeletal system of the newborn was chosen as the object of structural impact.
Bone and cartilage substances influence the function of the spinal cord. Neuronal fibers and veins connected to the spine are also integrated into the overall circuit. Treatment of the limbs, neck, and spine helps to normalize certain damaged areas of the brain affected by pathology (perinatal encephalopathy).
The structural theory in encephalopathy operates on measures affecting the bones and is rarely used to get rid of problems of fetal formation and their influence.
3. Fascial method.
Fascial therapy examines soft tissues, mucous membranes, and bloodstreams. Treatment of encephalopathy is based on the development of neural connections between individual parts of the body. The fascial method eliminates vegetative-visceral disorders of the brain of children and their consequence - hyperexcitability. Treatment of encephalopathy with fascial techniques involves correcting muscle dystonia if there are signs of increased muscle tone.
4. Visceral method for the correction of encephalopathy.
Visceral therapy uses the ability of internal structures to interact and influence each other. Thus, bilirubin encephalopathy requires synchronization of liver function.
Cerebral ischemia syndrome associated with hypoxia manifests itself in abnormal activity of the heart and lungs. Treatment is complex (minimal use of drugs).
Diagnostics
Perinatal ischemia syndrome due to cerebral hypoxia begins to be diagnosed by performing a visual examination of the child. It's the same with adults. Despite all the advances in medicine, a unique test that can accurately identify DIE has not yet been invented. All laboratory techniques are aimed at identifying how badly the brain is damaged and the current state of the whole organism.
What kind of research will be done depends on the symptoms and how they developed. To decipher the tests, there are special biomarkers that give a complete picture of the degree of HIE. The patient's blood is needed for the study.
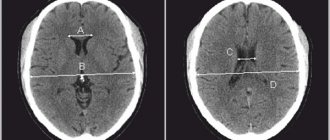
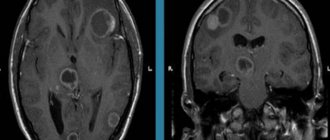
Neuroimaging is carried out using:
- neurosonography and/or MRI, a tomograph showing internal brain damage and changes in it;
- Doppler ultrasound, recording the functioning of cerebral blood flow;
- electroneuromyograph to determine the sensitivity of fibers of the periphery of the nervous system.
Additional can be used:
- electroencephalograph to detect developmental delay at an early stage and whether there is epilepsy;
- video monitoring to study the motor activity of children.
If necessary, the victim is examined by an ophthalmologist to determine the condition of the optic nerves and fundus of the eye, as well as the presence of genetic diseases in this area.