Cephalohematoma on the head of a newborn
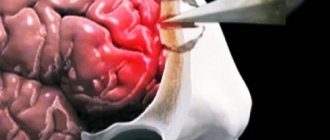
Cephalohematoma is a birth injury in newborns when hemorrhage occurs in the periosteum of the skull on one or both sides.
As a result, a lump is formed on the head, the diameter of which, depending on the degree of injury, can reach from several centimeters to twenty. Often the diagnosis is not made immediately, since in many babies a birth tumor can be observed at birth; passing through the birth canal, the baby’s head experiences pressure, resulting in swelling that subsides after 1-2 days.
But cephalohematoma in newborns does not go away in two days, but, on the contrary, can even increase in size, since during this period of life the blood is not yet able to clot quickly and continues to flow into the periosteum, the swelling grows. It is also distinguished from a generic tumor by clear boundaries - the hemorrhage is localized strictly within the affected bones of the skull.
Reasons for appearance
The formation of cephalohematoma in a newborn child is facilitated by many provocative factors:
- Large child size;
- Severe complications causing post-term pregnancy;
- Incorrect position of the child in the womb of the mother - longitudinal oblique or transverse;
- Hydrocephalic shape of the fetal head, outstripping its growth, in infectious pathologies;
- Deviations in fetal development caused by multisystem, endocrine and metabolic dysfunctions;
- Entwining the baby with the umbilical cord, which can cause hypoxia and will not allow the fetus to pass freely through the birth canal.
The cause of hemorrhages in a baby can be anomalies in the structure of the mother's pelvis - narrow or flat, the presence of bone or cartilaginous growths on the pelvic bones. The age of a woman is also of great importance, since in adulthood there is often incomplete divergence of the pelvic bones, which creates an obstacle to the free exit of the fetus.
There may also be weakness in labor - weakened uterine muscles and weakness of their contractile functions will not be able to help the child to the proper extent.
The formation of hemorrhage can also be provoked by the rapid progress of labor. The rapid pushing of the fetus out not only leads to a sharp drop in pressure (barotrauma effect), which can affect the blood vessels, but also provoke injury to the baby’s head, causing vascular damage.
Causes of intracranial hematomas in newborns
Numerous studies in the field of child neurology and pediatrics have shown that the main cause of the development of intracerebral hematomas in newborns is intrauterine hypoxia and asphyxia during childbirth. It has been proven that numerous hemorrhages in the brain can occur in the absence of any mechanical damage to the head; the presence of hypoxia is sufficient for extensive damage to the fetal vasculature. When there is a lack of oxygen in the baby’s body, serious disturbances in metabolic processes occur, leading to swelling of the brain, changes in the level of intracranial pressure and increased permeability of the vascular wall, which leads to the occurrence of multiple small hemorrhages. When larger vessels are damaged, an intracerebral hematoma is formed.
Additional causes of intracranial hemorrhage are mechanical effects on the fetal head during birth. This phenomenon often occurs in the following cases:
- Discrepancy between the size of the baby's head and the mother's pelvis.
- Pulling the fetus from the birth canal, using traumatic auxiliary devices for this.
- Incorrect insertion of the head into the pelvis.
- Prolonged labor.
- Rapid labor, strong labor activity.
One of the causes of intracerebral hemorrhage in a newborn is rapid labor
The likelihood of a cerebral hematoma in a newborn increases if the child has anatomical and physiological features predisposing to this - thin cranial bones, weak vascular walls, widened sutures between the cranial bones, impaired regulation of vascular tone, an immature blood coagulation system (vitamin K deficiency, hypoprothrombinemia) .
Various intrauterine infections affecting the liver, vascular system and brain of the fetus have a significant impact. Mycoplasma infections are especially dangerous in this regard. An iatrogenic factor (arising as a result of medical intervention) cannot be excluded - improper care of the baby and irrational drug therapy can contribute to the development of a cerebral hematoma.
Classification
Based on the combination of cephalohematoma with other possible injuries, the following are distinguished:
- cephalohematoma with skull fracture;
- cephalohematoma with brain damage (epidural hematoma, cerebral edema, or cerebral hemorrhage);
- combination of cephalohematoma with neurological manifestations (focal and general brain symptoms).
Based on the size of the subperiosteal hemorrhage, three degrees of cephalohematoma are distinguished:
- 1st degree – hemorrhage diameter is 4 cm or less;
- 2nd degree – diameter of cephalohematoma 4.1 – 8 cm;
- Grade 3 – the diameter of the hemorrhage is more than 8 cm (in the case of multiple cephalohematomas, the total area of hemorrhage is assessed).
Based on the location of the hemorrhage, cephalohematomas are distinguished: parietal (most common), frontal, occipital (less common) and temporal bone (very rare localization).
Symptoms of cephalohematoma
The first symptoms of cephalohematoma (see photo) become noticeable on days 2–3, when the birth tumor subsides.
The size of the hemorrhage tends to increase from the first day of birth, due to a deficiency of coagulation factors in the newborn’s blood - the blood remains liquid for a long time, so it is not possible to clot damaged vessels with blood clots.
The cephalohematoma is elastic to the touch; when you press on the area of hemorrhage, you can feel the movement of fluid. If the cephalohematoma is small in size, it begins to shrink on the 7th – 8th day and disappears without a trace. If the hemorrhage is significant, the process of its resorption may take several months. Often, a bone fracture (crack) is observed in the area where the cephalohematoma is located.
Cephalohematoma always has clear boundaries in the form of a compacted ridge around the circumference of the hemorrhage. The delimitation of the cephalohematoma is associated with the tight fusion of the periosteum with the bones of the skull in the area of the sutures, so the hemorrhage is located in the area of one bone.
Psychoneurological disorders in the long-term period of traumatic brain injury in children and adolescents
- brain concussion;
diffuse axonal damage;
When assessing the severity of TBI and predicting its course, the following indicators are taken into account:
- duration of loss of consciousness in the acute period of injury;
- Glasgow Coma Scale (GCS) score;
- duration of post-traumatic amnesia;
- assessment of the state of vital functions, focal symptoms in the area of the primary lesion and dislocation - according to the scale of the Research Institute of Neurosurgery named after N. N. Burdenko A. N. Konovalov, L. B. Likhterman, A. A. Potapov et al., 1998).
Depending on the severity of TBI, the following duration of loss of consciousness may be noted in the acute period of injury (R. Appleton, T. Baldwin, 1998):
- mild - duration of loss of consciousness less than 20 minutes;
- moderate - from 20 minutes to 6 hours;
- severe - from 6 to 48 hours;
- extremely severe - more than 48 hours.
Meanwhile, in children, especially younger age groups, loss of consciousness during TBI is not always observed and may even be absent in severe trauma.
To assess the condition of patients with closed TBI, GCS is widely used (B. Jennett, G. Teasdale, 1981), which allows one to judge not only the severity, but also make a prognosis for TBI. The overall GCS score is calculated by adding the scores for each of the three groups of reactions: eye opening, vocalization (or speech activity), motor activity. To increase the sensitivity and prognostic significance of the traditional scale in pediatric practice, age-specific modifications of the GCS have been proposed for children under 1 year of age and for children from 1 to 5 years of age; for children 6–15 years old, the same version of the scale is used as for adult patients (A. S. Iova et al., 1999). The overall GCS score can vary from 15 to 3 points. The severity of TBI according to the GCS is determined as follows (B. Jennett, G. Teasdale, 1981; KM Yorkston, 1997):
- easy: initial score 13-15 points;
- moderate: (1) initial score - 9-12 points or (2) initial score - 13-15 points, but after 3 days the score does not reach 15 points;
- severe: initial score - 3-8 points.
Since its development in 1974, the GCS has been widely used to determine the severity of TBI. It has been proven that as the total GCS score decreases, the likelihood of adverse outcomes increases. When analyzing the prognostic significance of the age factor, it was found that it significantly affects both mortality and disability in TBI. Despite some inconsistencies in the literature, outcomes are found to be better in children than in adults.
The uniqueness of the clinical course and outcomes of TBI in children is due to the fact that mechanical energy affects the brain, the growth and development of which is not yet complete. Due to the high plasticity of the developing brain, children are more likely to have a favorable outcome than adults, including after severe clinical variants of TBI. Meanwhile, even mild TBI in childhood does not always go away without leaving a trace. Thus, it has been shown that in the long-term period after a concussion (in the range from 6 months to 3 years), at least 30% of pediatric patients develop a complex of disorders referred to as post-concussion syndrome.
The main manifestations of post-concussion syndrome:
- cerebrasthenic symptoms - fatigue, emotional lability, anxiety, irritability, difficulty falling asleep;
- headaches, dizziness, periodically accompanied by nausea;
- moderately severe disturbances in coordination of movements when examining the neurological status;
- cognitive impairment (attention, memory), accompanied by difficulties associated with learning at school.
There is no doubt that moderate and severe TBIs lead to more serious consequences. It is necessary to keep in mind that the consequences of TBI may not appear immediately, but may be delayed. If TBI affects the normal course of brain development, then as a result it affects the formation of the child’s personality, his cognitive and emotional development, school learning, and the formation of social skills. The severity of psychoneurological disorders in the long-term period of TBI is largely determined by the initial severity of the injury.
Clinical manifestations of the consequences of TBI
Previously, it was believed that restoration of impaired functions after a TBI in children and adolescents occurs more fully than in adults. It was also believed that the younger the age at which the TBI occurred, the greater the likelihood of complete regression of neurological disorders. However, the results of targeted studies were not so optimistic (JR Christensen, 1996). Survival after severe TBI among pediatric patients is indeed higher than among adults, but there is a possibility of delayed clinical symptoms. Indeed, it gradually became obvious that in the long-term period of moderate and severe TBI, many children retained residual neurological disorders.
Moderate TBI is usually accompanied by transient neurological disorders, only in some cases they are persistent (JR Christensen, 1996). The outcomes of severe TBI, according to the literature, vary quite widely.
JD Brink. (1980) and co-authors studied the consequences of severe and extremely severe TBI in 345 children and adolescents under the age of 18 years. The duration of coma in the acute period of TBI was more than 24 hours with a median of 5–6 weeks. In the long-term period of TBI, 73% of patients moved independently and completely took care of themselves, 10% had restrictions in movement and remained partially dependent on care, 9% recovered consciousness, but remained completely dependent on others. The work of JF Kraus et al (1987) showed that with a GCS score of 3–4 points in the acute period of TBI, 100% of children develop at least moderate disability; with scores in the range of 5–8 points, 65% of those examined.
Movement disorders
Paresis or plegia of the limbs in the long-term period of TBI in children is quite rare. Often, when muscle strength is preserved, examination reveals a decrease in the speed of movement (D. Chaplin et al., 1993). In contrast, motor coordination disorders are observed in many children who have suffered a TBI (JR Christensen, 1996).
Although the restoration of motor functions in the long-term period of closed TBI in children is in many cases satisfactory, during a neurological examination even minor motor impairments are considered pathological. Residual movement disorders affect not only general motor activity and success in physical education and sports, but also the attitude of peers towards the child. With a negative attitude from peers, a child who has suffered a TBI develops social adaptation disorders.
Cognitive impairment
The severity of cognitive impairment in the long-term period of TBI is also determined by the initial degree of its severity. A number of disorders of higher mental functions are caused by the specific localization of lesions, in particular the predominant lesion in brain contusions of the frontal and temporal lobes. Cognitive disorders in patients who have suffered a TBI often affect such areas of mental activity as memory, attention, speed of processing incoming information, as well as executive functions provided by the prefrontal parts of the cerebral hemispheres (planning, organization, decision making). However, in many cases, residual disorders are formed due to diffuse involvement of the cortex and damage to the axial structures of the brain, which modulate the functional activity of the cortex. It is the combined damage to local zones of the cerebral cortex, axial and subcortical formations that leads to the development of disorders of memory, attention, regulation of the level of mental activity, emotions and motivation.
Speech disorders
Immediately after closed TBI, children often experience speech and motor impairments, which largely regress over time. Dysarthria (bulbar or pseudobulbar) is quite common; in some cases, motor aphasia is observed, as well as respiratory control disorders, accompanied by transient stuttering, whispered or monotonous speech. Among the features of speech in the long-term period of TBI, there may be a slow pace, difficulties in choosing words, a poverty of active vocabulary with the addition of one’s own speech with facial expressions and gestures, and in some cases, difficulties associated with understanding long and complex statements.
Difficulties in school
Traumatic damage to certain cortical centers can lead to specific difficulties associated with the formation of reading (dyslexia), writing (dysgraphia) or counting skills (dyscalculia), but such cases are not so common. In most children, the school skills acquired before TBI are retained or acquired again. Nevertheless, in many cases, the formation of school maladjustment is possible, caused by cognitive and speech disorders arising from TBI, as well as emotional and behavioral difficulties. Many children and adolescents in the long-term period of TBI experience the following difficulties associated with learning at school:
- The acquired knowledge is heterogeneous and fragmentary.
- During lessons at school, the child has difficulty getting involved in completing assignments and copes poorly with them.
- There are disturbances of attention during classes, difficulties associated with memorization are noted.
- The child is sloppy, does not finish what he starts, and is not organized.
- The child cannot effectively use the help of others in order to complete a task or work.
- The child experiences difficulties when it comes to applying information and skills, as well as in formulating conclusions and generalizations.
Emotional and behavioral disorders in children and adolescents in the late period of TBI are difficult to distinguish, since they are closely related to each other. Traumatic cerebrovascular disease is characterized by a predominance in the clinical picture of severe fatigue and irritability, sometimes reaching affective explosiveness; against this background, hysterical, neurasthenic, hypochondriacal or depressive symptoms often arise. Motor disinhibition, impulsiveness, inability to adhere to instructions and cope with certain tasks, and refusal to complete them are often noted. When a child or adolescent finds himself in difficult life circumstances, residual effects after traumatic brain lesions serve as a predisposing factor to the emergence of psychogenic or neurotic disorders and are a favorable basis for the pathological formation of personality. Emotional and behavioral disturbances in the long-term period of TBI make social adaptation difficult.
Behavioral disorders in the long-term period of TBI:
- outbursts of irritation, episodes of aggressive behavior;
- impulsiveness; motor disinhibition may be observed;
- emotional lability, mood swings;
- loss of motivation and interest in achieving good results when performing certain tasks and activities;
- isolation, indecisiveness, unsociability;
- dependence on others: the child cannot stand up for himself;
- inability to fully evaluate the results of one’s actions and correct one’s behavior;
- insufficient self-control and incorrect self-esteem, which entails difficulties when communicating with others.
Post-traumatic epilepsy is one of the most serious consequences of TBI suffered in childhood and adolescence. Post-traumatic epilepsy develops after open TBI - 50% of cases. Among them, in 2/3 of patients the onset of epilepsy is observed within the first year after TBI, in 90% - within 5 years after injury (including the first year of life), in another 7% of patients epilepsy develops 10-15 years after TBI. The maximum risk of developing post-traumatic epilepsy was observed in patients with focal neurological symptoms and massive damage to the central nervous system as a result of severe TBI.
In 70–80% of cases, the first epileptic seizures are accompanied by generalized convulsions (GM Fenichel, 1997).
After closed TBI, post-traumatic epilepsy is less common (GM Fenichel, 1997). Within 5 years, epilepsy develops in 11.5% of patients after severe TBI (brain contusion, intracranial hemorrhage) and in 1.6% after moderate TBI.
According to the results of a survey (N.N. Zavadenko, A.I. Kemalov, 2003) of 283 children and adolescents aged 6 to 14 years, in the long-term period of closed TBI (moderate and severe), the development of epilepsy was noted in 18 people. Among them: in 16 children, the occurrence of seizures (of the secondary generalized type) was noted in a period of 4 to 12 months after suffering a closed head injury; in two cases at the same time, closed TBI provoked the debut of idiopathic (hereditarily determined) forms of epilepsy - childhood absence epilepsy (in a 7-year-old boy) and idiopathic epilepsy with isolated generalized convulsive seizures (in a 10-year-old boy).
Thus, post-traumatic epilepsy refers to symptomatic forms of epilepsy. It is characterized by the same features as the group of symptomatic epilepsies as a whole (A. S. Petrukhin, K. Yu. Mukhin, 2000), namely:
- wide age range of onset of the disease;
- presence of changes in neurological status;
- frequent decline in cognitive function;
- identification of regional patterns on EEG;
- structural changes in the brain during neuroimaging;
- frequent resistance to antiepileptic therapy, which necessitates the use of valproic acid derivatives in the treatment of many patients.
Treatment of psychoneurological disorders in the long-term period of TBI in children and adolescents
Therapeutic and rehabilitation measures in the long-term period of TBI in children and adolescents should be intensively carried out both in the first 12 months after TBI, when it is reasonable to expect the most significant results from their use, and in the future, taking into account the ongoing processes of morphofunctional maturation of the central nervous system and the high plasticity of the developing brain . These activities should be comprehensive and include methods of psychological, pedagogical, speech therapy correction, psychotherapy, physical therapy, as well as drug treatment. To overcome cognitive and speech disorders, nootropic drugs are used. For post-traumatic epilepsy, long-term use of anticonvulsants is indicated. In order to prevent headaches, depending on the leading mechanisms of their pathogenesis, courses of vascular, dehydration drugs or anticonvulsants are recommended. For affective disorders and behavioral disorders, antidepressants and antipsychotics are prescribed, but anticonvulsants, especially valproates (drugs of valproic acid and sodium valproate), also have high therapeutic effectiveness in these conditions. In particular, valproates reduce aggressiveness and irritability, have a normothimic effect, and smooth out the severity of affective fluctuations.
The positive effect of nootropic drugs in the long-term period of TBI in children and adolescents is manifested in an improvement in general well-being, regression of headaches, and cerebrasthenic manifestations. In the neurological status, there is a decrease in the severity of motor disorders, especially in the coordination area; during a psychological examination, there is an improvement in memory, attention, and other higher mental functions. The duration of nootropic treatment courses in patients of this group should be at least 3–4 weeks. These drugs are prescribed in the first half of the day, which is associated with their psychostimulating effect. In the first days of use, a gradual increase in dose is recommended. In the presence of liquorodynamic disorders, nootropic therapy is supplemented with the prescription of dehydration agents. In patients with post-traumatic epilepsy, before using nootropics, it is necessary to achieve complete control of seizures for 4–6 months (at least) while taking anticonvulsants continuously.
In the treatment of post-traumatic epilepsy, valproates (Convulex, Depakine, Convulsofin) are among the basic antiepileptic drugs. Their long-term administration in stable therapeutic doses is aimed at preventing neuronal damage associated with repeated epileptic seizures. The development of neuronal damage will be indicated by: repeated epileptic seizures, decreased cognitive functions, behavioral disorders in the patient, the presence of abnormalities in the electroencephalogram and structural changes in neuroimaging. Therefore, an important direction in the treatment of psychoneurological disorders in the long-term period of TBI is neuroprotection, which implies anti-epileptic therapy in combination with functional and metabolic protection of the brain. The neuroprotective properties of valproates are confirmed by the following features of action:
- wide spectrum of antiepileptic activity (compared to other anticonvulsants);
- maintaining effectiveness during therapy with maintenance doses (often relatively low);
- the use of valproate does not lead to an increase in attacks;
- the use of valproate does not provoke new clinical manifestations of attacks;
- absence of specific cognitive impairments during therapy;
- no side effects in the emotional sphere;
- normalization of electrical activity of the brain;
- improving the quality of life of patients.
Approximate daily doses for valproate therapy are 15–45 mg/kg. Special forms, convenient for use in the treatment of children and adolescents, have been developed for the drug Convulex (Table 2). Thus, young children are prescribed drops for oral administration (containing 10 mg of sodium valproate in one drop) or syrup (containing 50 mg of sodium valproate in 1 ml).
Reducing the number of drug doses to 1–2 times a day can be achieved by using extended-release tablets containing 300 and 500 mg of sodium valproate.
Timely contact with a neurologist and rational drug therapy can achieve a significant improvement in the condition of children and adolescents in the long-term period of TBI. However, drug therapy alone is not enough to overcome the consequences of TBI. All children who have suffered a TBI need to be examined by a psychologist to identify possible disorders of higher mental functions. Often these violations are not severe, but even in these cases they can have a negative impact on the success of school and the child’s behavior. Therefore, assistance to children who have suffered a TBI should always be comprehensive.
Literature
- Zavadenko N. N., Kemalov A. I. Peptidergic nootropic drugs in the treatment of the consequences of closed traumatic brain injury in children // Bulletin of Practical Neurology. - 2003. - No. 7. - P. 44 - 50.
- Iova A. S., Garmashov Yu. A., Shchugareva L. M., Pautnitskaya T. S. Features of neuromonitoring in comatose states in children (Glasgow Coma Scale - St. Petersburg and its age-related features). Radiation diagnostics at the turn of the century. - St. Petersburg, 1999. - pp. 45-48.
- Konovalov A. N., Likhterman L. B., Potapov A. A. et al. Clinical guidelines for traumatic brain injury. - M., 1998. - T. 1. - 549 p.
- Petrukhin A. S., Mukhin K. Yu. Epileptology of childhood. - M., 2003. - 624 p.
- Appleton R., Baldwin T. Management of brain-injured children. New York, Oxford University Press. 1998: 257.
- Brink JD, Imbus C., Woo-Sam J. Physical recovery after severe closed head trauma in children and adolescents // J. Pediatrics. 1980; 97: 721-727.
- Chaplin D., Deitz J., Jaffe KM Motor performance in children after traumatic brain injury. Archives of Physical Medicine and Rehabilitation. 1993; 74:161 - 164.
- Christensen JR Pediatric Traumatic Brain Injury. In: Developmental Disabilities in Infancy and Childhood. 2nd ed. Eds. A. J. Capute, P. J. Accardo, Baltimore. 1996: 245 - 260.
- Fenichel GM Clinical Pediatric Neurology. A signs and symptoms approach. 3rd ed. Philadelphia, B. Saunders Company. 1997: 407.
- Jennett B., Teasdale G. Management of head injuries. Philadelphia, FA Davis Co. 1981: 258 - 263.
- Kraus JF, Fide D., Conroy C. Pediatric brain injuries: the nature, clinical course and early outcomes in a defined United States' population. Pediatrics. 1987; 79: 501 - 507.
N. N. Zavadenko, Doctor of Medical Sciences, Professor A. I. Kemalov, L. S. Guzilova V. E. Popov, Candidate of Medical Sciences M. I. Livshits, Candidate of Medical Sciences E. V. Andreeva, Candidate of Medical Sciences
RGMU, Moscow Morozov Children's Clinical Hospital, Moscow
Treatment of cephalohematoma in newborns
The disease is treated by a neonatologist and, according to indications, a pediatric surgeon. Therapy for cephalohematoma involves:
- Feeding the baby with donor or expressed breast milk for 4 to 6 days.
- Calcium preparations (Calcium gluconate) for a course of 3 - 5 days.
- Vitamin K course 3-5 days.
In case of suppuration of hemorrhage or large size (more than 8 cm) of the tumor, puncture of the cephalohematoma in the newborn is indicated. Also, a puncture is performed if the tumor does not shrink within 10 days.
The operation can be performed from the 10th day of the child’s life. At the site of the hematoma, hair is removed, the area is treated with an antiseptic and a puncture is performed. Then apply a tight bandage for 3 hours. If the operation is performed in case of suppuration of the hematoma, the contents are drained, followed by the application of an antiseptic bandage (with antibacterial drugs).
In case of ossification of the hematoma, to correct the deformation of the skull, resection of the periosteum to the native bone is performed.
Consequences of cephalohematoma
Why is this hemorrhage dangerous? Most often nothing. In the vast majority of cases, there are no consequences of cephalohematoma in a newborn, and at an older age it is impossible to say that the child had this complication of childbirth in the past.
However, with cephalohematoma, the following complications may occur:
- Anemia - develops with severe blood loss;
- Jaundice - due to the breakdown of hemoglobin with the formation of bilirubin;
- Suppuration - when bacteria enter the tumor through damaged skin;
- Ossification (ossification) of cephalohematoma - due to the deposition of calcium salts in the cavity.
Since blood accumulates above the bones of the child's skull, it cannot damage his brain and other parts of the nervous system. A festering hematoma, with timely and adequate treatment, will also not affect the condition of the body. The only consequence of cephalohematoma in the future can be detected when it is organized. If the blood is not absorbed, but is replaced by connective tissue, bone deformation occurs. However, with a small volume of hemorrhage (up to 70 ml), detecting this defect in the form of a small protrusion will be extremely difficult at an older age. As a rule, it does not have much cosmetic significance.
Let us emphasize once again that mental retardation, speech impairment, paralysis and other neurological diseases do not occur after cephalohematoma. A cephalohematoma is just a collection of blood that is located above the bone. The brain is located inside the cranium. The blood clot cannot deform the bone so much that it damages the organs contained in the baby's skull.
It is quite easy to recognize this pathology - there are characteristic external signs for this, so instrumental and laboratory diagnostics do not have any significance. Treatment for cephalohematoma is chosen by the doctor together with the child’s mother. Regardless of the tactics (surgical or conservative), hemorrhage is successfully treated and, most often, does not leave any consequences for the child.
Diagnosis and treatment of cerebral hematomas
The diagnosis of cerebral hematoma is made after a thorough examination of the condition of the newborn child. His obstetric history is clarified, and an examination is carried out by a neonatologist, neurologist, ophthalmologist and neurosurgeon. In young children, hematoma can be diagnosed using neurosonography - ultrasound examination of the brain through open fontanelles. In addition, a CT or MRI of the head may be prescribed.
Treatment of cerebral hematoma in most cases is carried out surgically - emergency removal of accumulated blood. Depending on the situation, aspiration, puncture, endoscopic or open extraction of the hematoma is performed. Treatment without surgery is possible only in the absence of any neurological symptoms, subject to careful monitoring of the child's condition. After the main treatment, a rehabilitation period begins - exercise therapy and massage are recommended for children.
Prevention
Periosteal hemorrhage can be avoided if the following conditions are met:
- the expectant mother should lead a healthy lifestyle and not take medications without consulting a doctor;
- The doctor and midwife must conduct the birth carefully, choose the method of delivery correctly and quickly.
To prevent recurrent hemorrhage, mothers should not rock the baby until 6 months of age. You cannot refuse surgical treatment of a hematoma. If your doctor recommends a cesarean section, it is best to choose this method of delivery. If these recommendations are followed, the child will quickly recover from the injury.
A cephalohematoma on the head of a newborn noticed in time, the treatment of which is quite easy, does not pose a threat to the child’s life.