Other information about different types of diseases starting with the letter “V”: Vegetative state, Ventricular, Vestibular ataxia, Vestibular neuronitis, Vibration disease, Viral meningitis, Viral encephalitis, Temporal lobe epilepsy, Intracerebral hematoma, Intracranial tumors of the cerebral hemispheres, Intracranial hypertension, Inflammatory myopathy, Inflammatory polyneuropathy, Congenital myopathy, Congenital paramyotonia, Secondary parkinsonism
Intracerebral hematoma: concept
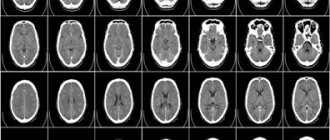
Intracerebral hematoma is a painful condition of the body, characterized by the accumulation of blood cells in the structures of the main organ, which causes compression, displacement and various types of damage to nearby tissue. The presented disease has such symptoms as: general cerebral and focal lesions that develop from the location of the injury and its size. To obtain detailed and detailed data about the disease being described, doctors resort to the use of computer equipment, magnetic resonance imaging and angiographic examination of cerebral vessels. A small hematoma can be treated conservatively, but in other situations, when the damage becomes significantly larger in diameter, this issue can only be resolved through surgery, by removal or aspiration.
Symptoms of a cerebral hematoma
Epidural hemorrhage has a light period, during which loss of consciousness is possible for a short time. The patient experiences severe headache, dizziness, and general weakness. Amnesia and anisoreflexia are possible.
On examination, mild meningeal signs are determined. Subsequently, the clinical picture worsens and the symptoms increase. The headache intensifies and is accompanied by severe vomiting. Consciousness is impaired to the point of stupor and coma. Heart contractions slow down, blood pressure rises, and mydriasis is observed on the side of the hemorrhage. It is possible to develop focal brain symptoms that indicate compression of the brain.
Subdural hematoma forms in 40% of intracranial hemorrhages. The patient has impaired consciousness, mental disorder, headache, and vomiting. The patient initially loses consciousness, then a light period occurs, and then a repeated loss of consciousness, up to coma. Amnesia, delirium syndrome, euphoric state, agitation, severe headache, and increased sensitivity to light are noted. On the affected side, the pupil is dilated.
Intracerebral bleeding compresses the surrounding brain tissue, which causes neuronal necrosis. Pressure increases inside the skull and swelling develops. Large volume hemorrhage causes displacement of the midline areas of the brain. The area of necrosis increases due to extensive spasm of the vessels surrounding the hematoma. Hemorrhage into the ventricular cavity occurs in 15% of cases.
Among the clinical symptoms, three phases with the presence or absence of a light period stand out. The patient's consciousness is impaired and psychomotor agitation is noted. Clinical symptoms depend on the location of the hemorrhage. One-sided muscle paresis, aphasia, pathology of the symmetry of tendon reactions, different pupil reactions, and epileptic seizures are recorded.
Useful facts
An intracerebral bruise may have a liquid texture or consist of coagulated blood. In certain situations, in addition, detritus may be present in the bruise in much smaller quantities. The total volume of liquid can reach 100 ml. The increase in the diameter of the hematoma continues for several hours after the onset of hemorrhage, and during a failure of the coagulation function much longer. After the formation of the lesion, the process of compression of adjacent tissues begins, which subsequently leads to necrosis.
In addition, the occurrence of such a phenomenon affects the increase in the level of intracranial pressure and becomes a source of swelling. It can cause displacement of certain structures and the formation of dislocation syndrome if the bruise is large. Bleeding can lead to a reflex spasm and the onset of ischemia, first affecting the nearby cavities. Ischemia is considered an additional damaging cause, which shapes the progression of abnormal deformations far beyond the boundaries of the formation. According to average statistical information, in almost 14% of cases there is a breakthrough into the ventricles and hemorrhage.
Magnetic resonance imaging (MRI) in St. Petersburg
MRI of the brain. T1-weighted axial MRI. Subdural hematoma. Color processing of the image.
All cerebral hemorrhages can be divided into the following types:
- intraparenchymal
- subarachnoid
- subdural
- epidural
- intraventricular
- intratumoral
Intraparenchymal hemorrhages are a consequence of hypertension and manifest themselves in the form of hemorrhages in the brain (hemorrhagic stroke) and hypertensive syndromes. Hemorrhagic stroke occurs due to the rupture of altered (hyalinosis, microaneurysms) vessels with increased blood pressure. The incidence of hemorrhagic stroke is about 9 cases per 100 thousand population. This is 10-18% of all deaths. In relation to all acute cerebrovascular accidents (ACVA), hemorrhagic stroke accounts for 10-20%. In addition, secondary diapidal hemorrhages are also observed in the ischemic type of stroke. Hemorrhages are also typical for venous infarctions. Patients are usually over 45 years of age. The localization of a hemorrhagic stroke can be almost any, but most often it is the basal ganglia, thalamus, and cerebellum.
Diagnosis consists of performing an MRI of the brain. The display of blood on MRI depends on the timing.
MRI of the brain. Axial T2-weighted MRI. Hemorrhage into the cerebellum.
MRI of the brain. T1-weighted coronal MRI. Mixed ischemic stroke. Early subacute stage.
Subarachnoid hemorrhage (SAH) is a hemorrhage between the arachnoid and pia mater. The epidemiology of SAH differs in different countries; in Russia it is about 6 per 100 thousand population. The most common cause of SAH is trauma, followed by rupture of a saccular aneurysm (85% of non-traumatic spontaneous hemorrhages). The remaining 15% of non-traumatic hemorrhages include benign perimesencephalic hemorrhage of unknown etiology and venous rupture. The mortality rate from SAH is very high and depends on the size and location of the hemorrhage.
Clinical manifestations consist of:
- Unexpected attack of severe headache
- Photophobia, nausea, vomiting
Neurological examination reveals meningeal signs, often the only sign of SAH. CSF xanthochromia appears 12 or more hours after SAH and can only be a method of late confirmation. Various approaches to radiological diagnosis of SAH have been proposed. On the first day, MRI is preferable, since blood may already be visible on T2-MRI gradient type or FLAIR. At a later date, up to 3-5 days, CT is preferable. Then again MRI, which is more sensitive than CT in the subacute and chronic phases of hemorrhage. The amount of blood is assessed using the Fisher scale. She divides hemorrhage into 4 groups:
- Blood is not visualized
- Diffuse SAH with a thickness of up to 1 mm, without clots
- Blood clots and/or SAH thickness greater than 1 mm
- Intracerebral or intraventricular hemorrhage in combination with SAH
MRI of the brain. Axial MRI type FLAIR. Aneurysm and SAH, intraventricular hemorrhage.
Subarachnoid hemorrhage is dangerous due to vasospasm, which is observed on days 5-7. The spasm itself is well determined by duplex scanning. MRI of the brain can detect early signs of ischemic stroke.
MRI of the brain. Diffusion-weighted MRI sequence. ACVA in the acute stage due to vasospasm.
A subdural hematoma usually occurs due to rupture of veins. The causes of subdural hematoma are trauma, anticoagulant therapy, sudden decompression during ventricular bypass surgery for hydrocephalus. Subdural hematomas are very rare when aneurysms and AVMs rupture. Clinical manifestations are associated with the mass effect. The incidence of subdural hematomas is about 1 case per 10 thousand population. Subdural hematomas are located along the convexital surface, occasionally, along the interhemispheric fissure and tentorium, in the region of the posterior cranial fossa. There may be a combination of subdural hematoma with hemorrhage in adjacent areas of the brain. the prognosis in these cases is unfavorable. The appearance of a hematoma on CT and MRI depends on how old it is. Subdural hematomas have a sickle shape.
MRI of the brain. Axial T2-weighted MRI. Subacute subdural hematoma.
Epidural hematoma (extradural hematoma) is of traumatic origin. This is an accumulation of blood inside the bone plate and dura mater. Usually the hematoma is located under the area of the skull fracture. The cause of hemorrhage is a rupture of the enclosed artery. Epidural hematomas are half as common as subdural hematomas. The hematoma is biconvex in shape. It is most often diagnosed in an emergency using CT. MRI is commonly used for spinal epidural hematomas.
CT. Epidural hematoma.
Intraventricular hemorrhages are primary and secondary. Primary hemorrhages are observed with intraventricular tumors, some aneurysms (posterior inferior cerebellar with accumulation of blood in the 4th ventricle) and subependymal cavernous angiomas. Secondary hemorrhages occur as a consequence of blood breaking into the ventricles during intraparenchymal hemorrhages and SAH.
MRI of the brain. Axial T2-weighted MRI FLAIR type. Intraventricular hemorrhage.
Intratumoral hemorrhages are rare. usually they are not extensive, as, for example, with apoplexy of pituitary adenomas. Apoplexy is an acute disruption of the blood supply to the pituitary gland with necrosis or hemorrhage. The incidence is about 10% of cases of macroadenomas. Clinically, apoplexy appears with headaches, vomiting and visual disturbances. Rarely, extensive hemorrhages are observed in metastases.
MRI of the brain. Coronal T1-weighted MRI. Apoplexy of pituitary macroadenoma with hemorrhage.
Intracerebral hemorrhage of any type is considered an emergency and an MRI in St. Petersburg is usually performed in the emergency room of a hospital, or an urgent CT scan is performed. In the subacute stage, the capabilities of MRI in St. Petersburg allow the study to be performed in stationary conditions and in a chronic setting using open MRI.
Leave feedback.
MRI in St. Petersburg USA
Mechanism of occurrence
The described disease can manifest itself due to the following factors:
Rupture of vascular walls due to injury (for example, head injury, concussion, etc.).- Post-traumatic diapedesis at the point of contusion.
- Deformation of an aneurysm or arterial-venous malformation due to tumor formation (stroke, hypertension, atherosclerosis, etc.).
- Changes in the rheological functions of blood vessels during hemophilia, leukemia, painful conditions of the liver and others.
What does blood look like on MRI?
In medical practice, the following types of intracranial hemorrhages occur:
- intraparenchymal hematoma - the formation is caused by rupture of blood vessels due to hemorrhagic stroke (most often due to high blood pressure), traumatic destruction of the artery, inflammatory destruction of the vascular wall, etc. In the images, the hemorrhage is locally located among the white matter of the brain, without connection with damage to the bone structures of the skull, even if the pathology occurred after a head blow;
Intracerebral hematoma due to hemorrhagic stroke (indicated by arrows)
- subarachnoid hemorrhage (SAH) - occurs as a result of a violation of the integrity of a vessel located on the surface of the brain in the subarachnoid space (for example, when a saccular aneurysm ruptures). The main pathological symptoms are considered to be a sudden severe headache, nausea with vomiting and photophobia, depression of consciousness up to coma. This type of hemorrhage provokes vasospasm. In the images, the SAH is located on the surface of the brain;
- subdural hematoma is localized under the dura mater. It differs in the shape of the sickle when visualized on magnetic resonance or computed tomography. Occurs as a result of rupture of veins after injuries, taking anticoagulants, ventricular bypass, and is characterized by a high percentage of deaths. Causes severe displacement of the brain due to intracranial pressure;
- epidural hematoma - usually determined after traumatic injuries. It is localized under the fracture area, between the bones of the skull and the dura mater of the brain. Visually it looks like a biconvex lens;
- intraventricular hemorrhage - primary (formed by a tumor, aneurysm, angioma, etc.) and secondary (as a consequence of the breakthrough of blood from the area of hematoma formation into the ventricular cavity with a large volume of the first);
Types of intracerebral hematoma
In modern medicine, in particular in the field of neurology, several forms of the present disease are used, which can give an idea of its different characteristics. According to location, there are the following types: central, subcortical, cortico-subcortical, and formation of damage in the cerebellum. In addition, there are such types as:
- Lobar.
- Medial.
- Lateral.
- Mixed.
With different volumes of pathology, the following differences are present:
- Small bruise - the size does not exceed three centimeters.
- Medium - reaches 4.5 cm.
- Large - more than 4.5 cm.
The classification of such injuries due to the phenomenon can be:
- Post-traumatic form.
- Hypertensive.
- Aneurysmal.
- Tumor, etc.
| To main |
(Radiation News 1998 4: 26-28)
Beginning. Read the continuation
in issue 5 for 1998.
RCT and MRI diagnostics of complications and consequences of traumatic brain injuries.
Bulaev I. V., Korytko S. S.
Clinic of the Research Institute of Radiation Medicine.
Traumatic brain injury is damage to the skull and brain resulting from mechanical impact. TBIs account for 30-40% of the overall structure of injuries, while among combined injuries they account for about 80%.
Mechanisms of traumatic brain injury.
1. Direct hit
- this is an effect on the motionless brain. Localization - frontal and temporal lobes (usually bilateral), often combined with acute subdural hematoma.
2. Anti-shock
- this is a contusion of the brain on bone and meningeal intracranial formations, due to its displacement in the cranial cavity in the direction opposite to the place of application of force. Localization - more often in the frontal, especially supraorbital areas, temporal, occipital areas at the upper edges of the cerebral gyri with varying degrees of spread into the projection of the underlying white matter.
3. Damage to deep structures (white matter)
- due to rotational and axial displacement of the brain in the cranial cavity, which causes ruptures of blood vessels and damage to various areas of the brain as a result of its bruises on bone and meningeal intracranial structures.
Localization: corpus callosum, internal capsule, basal ganglia, thalamus optic, upper parts of the brainstem, cerebellar peduncles, cortical-subcortical areas.
4. Hydrodynamic shock
- associated with the movement of cerebrospinal fluid in the ventricles of the brain, cerebrospinal fluid tracts and subarachnoid spaces.
Consequences of traumatic brain injuries.
1. Post-traumatic hydrocephalus
— obstruction of the cerebrospinal fluid pathways due to intraventricular hemorrhages; usually develops within 3 months (1/3 of cases).
2. Diffuse brain atrophy
- develops as a result of ischemia and hypoxia of the brain substance (1/3 of cases).
3. Encephalomalacia
- the presence of foci of low density in the substance of the brain (the density of the foci is usually higher than that of the cerebrospinal fluid).
4. Pseudoporencephaly
— the presence of liquor-containing spaces connecting the subarachnoid space and the ventricular system of the brain.
5. Subdural hygroma
- limited accumulation of cerebrospinal fluid in the subdural space.
6. Leptomeningeal cyst
is a progressive protrusion of the membranes through a traumatic defect of the convexital surface of the skull.
7. Liquorrhea
- leakage of cerebrospinal fluid through a defect (rupture) of the dura mater and skull bones (rhinorrhea, otorrhea).
8. Carotid-cavernous anastomosis.
9. Traumatic pseudoaneurysm
- most often localized in the projection of the branches of the anterior and middle cerebral arteries, the intracavernous part of the internal carotid artery, as well as the posterior communicating artery.
10. Post-traumatic abscesses.
11. Compression of blood vessels
— the posterior communicating artery in the projection of the tentorium cerebellum is most often subject to compression with the development of an infarction in the area of the blood supply.
Classification of traumatic brain injuries (according to J. Petit).
A. Concussion. B. Bruises. B. Compression of the brain. D. 1. Intracerebral hemorrhages: a) Hematoma. b) Bruise. 2. Extracerebral hemorrhages: a) Subdural hematoma. b) Epidural hematoma. c) Subarachnoid hemorrhage. 3. Other post-traumatic foci: a) Pneumocephalus. b) Foreign bodies.
Intracranial hematomas
(
Table 1
)
.
Intracerebral hemorrhages (
Table 2
,
Fig. 1, 2
)
.
The organization of hematomas occurs from the periphery to the center and the timing of organization depends on the size of the hematoma (usually from 1 to 6 weeks).
Negative CT images can be observed with: a) blood clotting disorders; b) anemia; c) iso- and hypodense stages of hematoma organization.
Tab. 1.
Characteristics of post-traumatic intracranial hematomas depending on the stage of their organization.
| Period | RKT | MRI |
| Acute period (up to 24 hours) | Non-contrast CT: - a homogeneous high-density focus with irregular, fairly clear contours, increasing in density during the first 3 days (the density of the hematoma depends on the hemoglobin concentration and the degree of clot retraction); - usually the lesion is surrounded by a low-density zone (edema, softening), which appears after 24-48 hours: - irregularly shaped in case of injury, - spherical and uniform in case of spontaneous hemorrhage, - small mass effect compared to the tumor. | Non-contrast MRI: - the center of the hematoma is isointense on T1W and clearly hypointense on T2W (deoxygenation of the clot - paramagnetic deoxyhemoglobin is formed); - adjacent areas of the medulla are isointense on T1W, hyperintense on T2W (edema). |
| Subacute period (from several days to 1 month) | Non-contrast CT: - increase in the size of the hemorrhage area over days and weeks; - high-density lesion for 1 week, often with dissection; - gradual decrease in density from the periphery (by 1-2 units per day) over 2-3 weeks; - the focus of hemorrhage becomes isodense from 3 to 10 weeks with the presence of a hypodense zone around it (edema zone). Post-contrast RCT: - peripheral enhancement ring at the internal border (1-6 weeks after hemorrhage) in 80% of cases (due to disruption of the BBB, increased perfusion and the formation of well-vascularized granulation tissue); - the ring-shaped area of edema around the lesion decreases after the administration of corticosteroids. | Non-contrast MRI: - the center of the hematoma is isointense on T1W and moderately hypointense on T2W; -peripheral areas are hyperintense on T1W and hyperintense on T2W (conversion of deoxyhemoglobin to methemoglobin after 3-4 days); — ring-shaped areas that are isointense on T1W and clearly hypointense on T2W (paramagnetic hemosiderin appears within the 2nd week); - the area of edema surrounding the lesion is isointense on T1W and hyperintense on T2W. |
| Chronic stage (from 1 month to several years) | Non-contrast X-ray CT: - hypodense phase (4-6 weeks); - progressive decrease in density (3-6 months). | Non-contrast MRI: - central areas are hyperintense in T-1 and T-2 modes (extracellular lysed methemoglobin from erythrocytes - from several months to 1 year); - peripheral areas are hyperintense in T-1 and T-2 modes; — annular zone isointense in T-1 and hypointense in T-2 (gradually increases in thickness and fills the entire hematoma zone with hemosiderin). |
Table 2.
Characteristics of intracerebral hemorrhages depending on the stage of organization.
| RKT | MRI |
| Sensitive for hemorrhages in the acute stage. | More sensitive for detecting foci of hemorrhage in the subacute and chronic stages. |
| - focal or multiple (in 29%) poorly contoured areas with unclear contours + inhomogeneous increase in density + adjacent area of edema; - foci of hemorrhage become isodense after 2-3 weeks; - small degree of post-contrast enhancement; - areas of mildly reduced density + mass effect (diffuse petechial hemorrhages) associated with delayed hematoma formation; - diffuse swelling of the brain substance without signs of hemorrhage in the early post-traumatic period (often in children), due to hyperemia or ischemic edema. | - first, a zone of decreased signal intensity (deoxyhemoglobin in the acute stage) - surrounded by a hyperintense zone of edema (in T-2 mode); - the same zone becomes hyperintense in both modes in the subacute stage (methemoglobin); - in T-2 mode in the chronic stage there is either a hyperintense signal (areas of gliosis) or a hypointense signal (hemosiderin). |
| Rice. 1. Intracerebral hematoma of the left occipital lobe. Acute stage. (Left) T1 mode. (Right) T2 mode. | Brain contusions. They are characterized by the presence of foci of destruction in the substance of the brain, symptoms of focal brain damage, subarachnoid hemorrhage and, in some cases, fractures (cracks) of the skull bones. Frequency - occurs in 21% of all TBIs.
|
What is the manifestation of an intracerebral hematoma?
Typically, the described illness occurs with fairly pronounced symptoms of a general cerebral nature. When visiting the office of a specialist in the field of neurology, patients report dizziness, painful sensations of acute heaviness in the head area, attacks of nausea and gag reflexes. Almost 50% of cases manifest with disturbances of consciousness from stupor to coma. At some points, a sharp change in mood occurs and instead of a depressed state, a person begins to experience psychomotor activity. The formation of a hematoma can occur with the presence of an erased light space. Further patient complaints are directly dependent on the size and location.
Doctors list the following symptoms as the most common problems:
Disturbances in the functioning of the speech apparatus.- Malfunctions in the operation of numeric parameters.
- Asymmetry of tendon movements of both limbs.
- Seizures of a convulsive and epileptic nature.
- Anisocoria.
- Loss of vision.
- Memory disorders and behavioral problems.
- Dislocation syndrome.
- Displacement of brain areas.
- Uncontrolled eye orbital movement activity.
- Difficulty with the breathing device.
- Hearing loss.
- Vestibular ataxia.
- Strabismus.
- Increased pressure and others.
Age of hematoma on MRI
The blood signal on MRI is variable and changes depending on the age of the hemorrhage.
MR signal intensity from the hemorrhage focus – T2-VI mode):
< 1 day – the most acute stage
- intracellular oxyhemoglobin.
- isointense on T1
- isointense to hyperintense on T2
1 – 2 days – acute stage
- intracellular deoxyhemoglobin.
- T2 - signal intensity decreases (T2 shortening)
- T1 - an isointense signal remains on T1
3 – 7 days – early subacute stage
- intracellular methemoglobin
- the signal gradually increases (T1 shortening) and gradually becomes hyperintense.
- T2 is a hypointense signal.
7 - 14-28 days - late subacute stage
- extracellular hemoglobin.
- within two weeks, the cells are destroyed and due to the release of methemoglobin, the T2 signal increases.
More than 14-28 days - chronic stage
Peripheral part
.
- intracellular hemosiderin
- signal reduction on T1 and T2
Central part.
- extracellular hemichromat
- isointense signal on T1
- hypertensive on T2
Scheme
Use in practice.
It is not always possible to relate these data to extracranial hematomas.
The GRE mode is more sensitive to old hemorrhages.
Examples:
Acute on chronic. Subdural hemorrhage. Man 85 years old
(A-chronic B-acute).
A 69-year-old patient with subacute subdural hematoma.
The patient 4 years ago had a hemorrhage in the right parietal lobe as he was intensively treated for heart problems with coagulants.
1. Schaller B. State-of-the-art imaging in stroke. Nova Biomedical. (2007) ISBN:1600215009. Read it at Google Books — Find it at Amazon
2. Bradley WG. MR appearance of hemorrhage in the brain. Radiology. 1993;189(1):15-26. Radiology (abstract) - Pubmed citation
3. Grand DJ, Woodfield CA, Mayo-Smith WW. Practical Body MRI: Protocols, Applications and Image Interpretation (Cambridge Medicine). Cambridge University Press. ISBN:1107014042. Read it at Google Books — Find it at Amazon
4. Leyendecker JR, Brown JJ, Merkle EM. Practical Guide to Abdominal and Pelvic MRI. L.W.W. ISBN:1605471445. Read it at Google Books — Find it at Amazon
5. Linfante I, Llinas RH, Caplan LR et-al. MRI features of intracerebral hemorrhage within 2 hours from symptom onset. Stroke. 1999;30(11):2263-7. doi:10.1161/01.STR.30.11.2263 - Pubmed citation
6. https://radiopaedia.org/articles/ageing-blood-on-mri
Diagnostic options
With the help of new-fangled clinical devices, doctors have a large number of opportunities to conduct research on patients with the presenting disease. Thanks to such devices, doctors can study not only the formation itself, but also understand what causes the development. The main technology used by specialists in the capital’s medical institutions is computed tomography. Often, on the images obtained, experts see the pathology in the form of a round or oval lesion. If deviations from the norm occurred due to damage, then, as a rule, uneven boundaries are visible in photographs.
In case of diameter reduction, magnetic resonance scanning is used. In some situations, this examination may give erroneous readings, which is why doctors prefer to use two tests simultaneously. At certain points, angiographic examination or MR angiography is performed to determine vascular disorders and the formation of aneurysms.
Diagnostics
Patient examination plan
Clinical examination:
- time of onset of symptoms (or time the patient was last seen well);
- first symptoms and progression of the disease;
- standard risk factors for cardiovascular complications;
- medications taken;
- previous injuries and surgeries;
- alcohol and drug use;
- history of epilepsy and seizures;
- liver diseases;
- oncological and hematological diseases;
- cognitive status before stroke (history of dementia and psychotic disorders);
- MR - data on amyloid angiopathy based on the results of previous studies.
Laboratory and instrumental examination:
- complete blood count (erythrocytes, leukocytes and platelets);
- biochemical blood test (sodium, potassium, blood glucose, urea, creatinine, ALT and AST) and coagulogram (aPTT, INR and TV);
- electrocardiogram and chest x-ray;
- computed tomography (CT) and magnetic resonance imaging (MRI) are considered the “methods of choice” for identifying and assessing ICH in emergency care;
- CT angiography and other angiographic studies (MR angiography, catheter angiography), especially in patients with a SICH score > 2 points.
Determining the etiology of ICH may require more time than the length of the patient's hospitalization. Conditions for which a reliable diagnosis requires MRI or CT studies over time include cavernous malformations and dural fistulas.
CT scan of the brain
Non-contrast CT of the brain is the method most often used to detect acute ICH, the signs of which appear almost immediately after its development. CT scan can determine the size and location of hemorrhage. It also provides information about the spread of blood into the ventricular system, the presence of surrounding edema, and displacement of individual parts of the brain (herniation). Blood in the acute period forms areas of increased x-ray density, with the exception of patients suffering from anemia, in whom areas of hemorrhage may be isodense. After a few weeks, the blood becomes isodense. A ring-shaped increase in density around the lesion may form. In the chronic stage, the focus of hemorrhage has a reduced x-ray density.
MRI of the brain
Parenchymal hemorrhage in the most acute stage is detected with high accuracy on MRI in T2 modes, such as gradient echo (GRE). These sequences are highly sensitive to non-uniform static magnetic fields generated by molecules with paramagnetic properties, such as deoxyhemoglobin. This property of paramagnetic molecules determines the effect of magnetic susceptibility, which leads to rapid phase relaxation of proton spins. This results in signal loss (darkening or hypointensity), which is more noticeable on T2*-weighted images. Signs of hemorrhage according to computed tomography and magnetic resonance imaging at various stages are presented in Table 1.
Table 1. Signs of hemorrhage according to computed tomography and magnetic resonance imaging at various stages.
| Stages | CT | T1-weighted MRI | T2-weighted MRI | gradient echo MRI |
| Acute (<12 hours) | High density (hyperdense focus) | Isointense or slightly hyperintense | Hyperintense | Hypointense rim |
| Acute (12 hours - 2 days) | High density | Iso-or hypointense | Hypointense | Hypointense rim, increasing in intensity towards the center |
| Early subacute (2–7 days) | High density | Hyperintense | Hypointense | Hypointense |
| Late subacute (8 days - 1 month) | Density similar to surrounding brain tissue (isodense lesion) | Hyperintense | Hyperintense with low intensity rim | Hyperintense with low intensity rim |
| Chronic (>1 month) | Low density (hypodense lesion) | Hypointense | Hypointense | Slit-shaped hyperintense or isointense core surrounded by a hypointense rim |
Determination of the volume of hemorrhage
Figure 1. Typical locations of intracerebral hematomas
Putamen (A), thalamus (B), subcortical white matter (C), pons (D), and cerebellum (E).
Thalamic and subcortical hemorrhages are often accompanied by blood escaping into the cerebral ventricles (B and C). Cerebral amyloid angiopathy, drug use, and vascular abnormalities often lead to the development of lobar hemorrhages (F).
Dastur CK, Yu W. Current management of spontaneous intracerebral haemorrhage. Stroke Vasc Neurol 2017; 2(1): 21–29. Copyright © 2017 BMJ Publishing Group Ltd.
Figure 2. Method for assessing the volume of intracerebral hemorrhage using the ABC/2 formula
Using the ABC/2 method to assess acute hemorrhage in the left subcortical nuclei: A = 6 cm, B = 4 cm and C = 3 cm (hematoma is determined on 12 sections 0.25 cm thick). The volume of the hematoma is 36 cm³ ((6×4×3)/2).
Thabet AM, Kottapally M, Hemphill JC 3rd. Management of intracerebral hemorrhage.
A - the largest diameter of hemorrhage on a CT slice with the largest area of hemorrhage, shown in Figure 2 (sample section).
B is the largest diameter in a plane located at an angle of 90 degrees to cut A (Fig. 2).
C is the approximate number of CT slices that have hemorrhage multiplied by the thickness of the slices in centimeters. In order to calculate C, each CT slice that shows signs of hemorrhage is visually compared with a reference slice. Each section on which there are signs of hemorrhage is counted as one if the area of hemorrhage is > 75% of the area on the section with the maximum size of hemorrhage. A section is counted as 1/2 if the hemorrhage area is between 25 and 75 percent of the area on the section with the largest hemorrhage size. If the area of the hemorrhage is <25% of the area on the largest section, the section is not taken into account in the calculation. ABC/2 allows you to obtain the volume of hemorrhage in cubic centimeters.
Comparison of the capabilities of neuroimaging of the VMG using CT and MRI methods
Figure 3. Comparative characteristics of CT and MRI
Signs of risk of hematoma enlargement
Among patients who undergo a CT scan of the brain within the first three hours from the onset of the disease, the proportion of those who subsequently experience hematoma growth is 28–38%. An increase in cerebral hematoma is considered to be an increase in its volume by more than 6 ml or an increase in relative size by more than 33%.
The most important independent prognostic factors for cerebral hematoma enlargement are signs of blood extravasation on native CT and CT angiography images. In the multicenter PREDICT study, the presence of the blend sign described below was associated with a 2.3 (95% CI 1.6–3.1) fold risk of hematoma enlargement (see Figure 5).
Table 2. Indicators of the risk scale for hematoma progression
| Index | Points |
| Taking Warfarin | |
| No | 0 |
| Yes | 2 |
| Time until hematoma is detected on CT (hours) | |
| ≤6 | 2 |
| >6 | 0 |
| Initial hematoma volume (ml) | |
| <30 | 0 |
| 30–60 | 1 |
| >60 | 2 |
| Symptom of “blot” on CT angiography | |
| No | 0 |
| Eat | 3 |
| No data | 1 |
Table 2 presents a scale for assessing the risk of progression of ICH in patients on warfarin therapy. The absence of risk indicators on this scale is associated with a low risk of hematoma expansion with a probability of no more than 5.7%. A patient's score from 1 to 3 on this scale is associated with an average risk of hematoma expansion with a probability of 12.4%. With a probability of 36.4%, the risk of hematoma expansion will be high if the number of points on this scale is from 4 to 9 points.
Figure 4 shows the "whirlpool" sign, which demonstrates on non-contrast CT CT hypodense or isodense areas of round, linear, or irregular shape (compared to normal brain parenchyma) in an area of increased x-ray density consistent with hemorrhage. Limited data indicate that the whirlpool sign is associated with increased hemorrhage size, poor outcome, and increased mortality.
Figure 5 shows the “blob” symptom, a phenomenon detected in patients with intracerebral hemorrhage on cerebral CT angiography. Single or multiple foci of contrast enhancement are identified within acute primary intracerebral hemorrhage (ICH), located without direct contact with normal or pathologically altered blood vessels.
Whirlpool symptom
Lesions should not be detected until contrast is administered. They correspond to areas of ongoing bleeding. According to several studies, the “blob” symptom is associated with increased hemorrhage and poor prognosis. In a retrospective analysis of a group of 367 patients with acute ICH, the “blob” symptom was observed in 19% and was an independent risk factor for increased hemorrhage size. Similar results have been described in other retrospective series showing an association between these changes and patient mortality. Despite less study, small "blobs" of contrast material on MRI - the MRI "blob" symptom was also detected on T1 and dynamic T1-weighted images, especially if the study was performed within the first 6 hours after the development of ICH. Blotches on MRI may be associated with hematoma enlargement and worse clinical prognosis, but the exact significance of the symptom is not well understood. A number of studies have shown that the assessment of the “blot” symptom, taking into account the number of lesions, their maximum size and density, is a significant prognostic factor for increasing the size of the hematoma. The most significant predictor was the number of “blots”.
Figure 5. Symptom of “blot”
Risk factors for poor outcome
Risk factors for unfavorable outcome of ICH include:
- low Glasgow Coma Scale score;
- hemorrhage volume ≥30 cm³;
- ventricular hemorrhage;
- hemorrhage into infratentorial structures;
- age ≥80 years;
- widespread lesions of the subcortical white matter;
- low body weight on admission;
- chronic kidney disease (GFR <60 ml/min/m²).
What's the forecast?
The main reasons on which further prognosis of the patient’s condition depends include:
- Volume and localization.
- Age range of the patient.
- The presence of concomitant abnormalities (high body weight, hypertensive diseases, diabetes mellitus, etc.).
- Level and extent of disturbances of consciousness.
- Combination of intracerebral formations with trauma to the membranes.
- Timely seeking medical help.
- Adequacy and qualifications of the doctor.
The most negative prognosis can be made in the presence of a breakthrough form of the disease. The main factors of death are swelling and dislocation of the brain. According to average statistical data, more than 10% of cases end in death after recurrence of hemorrhage, and 70% of patients are diagnosed with a disabling neurological deficit.
1. Intracerebral hematoma and the causes of its occurrence
Intracerebral hematoma
- a serious threat to the life and health of the patient, since it compresses the brain tissue, disrupting the functioning of serious brain centers that ensure the normal functioning of human systems and organs.
Intracerebral hematomas can be either a consequence of traumatic brain injury or the result of cerebral vascular pathology due to an aneurysm, hypertensive crisis, or uncontrolled use of certain medications, in particular anticoagulants.
A must read! Help with treatment and hospitalization!