Intercostal neuralgia is a disease in which irritation or compression of the intercostal nerves occurs. This can happen for various reasons. The disease is relatively rare, its main manifestation is pain along the affected nerve.
Our expert in this field:
Lashch Natalia Yurievna
Neurologist of the highest category, candidate of medical sciences, associate professor. Laureate of the Moscow City Prize in the field of medicine.
Call the doctor Reviews about the doctor
How are intercostal nerves arranged? What functions do they perform?
Two nerve roots emerge from the spinal cord: the anterior one is formed by the processes of motor nerve cells, the posterior one - by sensory ones. Then, while still inside the spinal canal of the spine, these roots are connected to form the spinal ganglion. Two spinal nerves depart from it: anterior and posterior.
In the thoracic spinal cord, the anterior branches of the spinal nerves pass into the intercostal nerves. They pass in the spaces between the ribs - each of them is located along the lower edge of the corresponding rib - and, unlike the anterior spinal roots, are mixed, that is, they are responsible for both movement and sensitivity:
- provide movement of the chest muscles involved in the breathing process;
- provide sensitivity to the skin of the chest and upper abdomen.
Spinal nerves
The number of pairs of spinal nerves and their location correspond to the segments of the spinal cord: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1 coccygeal pair. They all arise from the spinal cord via the posterior sensory and anterior motor roots. The roots unite into one trunk and exit the spinal canal through the intervertebral foramen. In the area of the intervertebral foramen there are spinal nodes (ganglion spinale), which are a cluster of sensitive cells and are part of the dorsal roots. Sensitive fibers begin from the cells of the spinal ganglion, and motor fibers begin from the cells of the anterior horn. When united, the nerves become mixed. After leaving the intervertebral foramen, the spinal nerves are divided into posterior and anterior mixed branches. The posterior ones are directed to the muscles and skin of the posterior parts of the body, and the anterior ones innervate the muscles of the anterior part of the body and limbs. Uniting with each other in other sections, the nerves form the cervical, brachial, lumbar and sacral plexuses.
The cervical plexus (plexus cervicalis) (Fig. 267, 268, 269, 270, 277) is formed as a result of the union of the branches of the four upper cervical nerves and is located on the deep muscles of the neck. Coming from under the posterior edge of the sternocleidomastoid muscle, the branches of the cervical plexus are divided into sensory, motor and mixed.
Sensitive branches include: - small occipital nerve (n. occipitalis minor) (Fig. 267, 268, 270), heading to the skin of the back of the head; - large auricular nerve (n. auricularis magnus) (Fig. 268, 270), which innervates the skin of the earlobe and the convex side of the auricle; - transverse nerve of the neck (n. transversus colli), heading to the skin of the neck; - supraclavicular nerves (nn. supraclaviculares) (Fig. 267, 268, 273), passing under the collarbone and above the deltoid muscle. The motor branches go to the deep muscles of the neck and the muscles located below the hyoid bone, and also innervate the sternocleidomastoid and trapezius muscles. The mixed branch of the cervical plexus is the phrenic nerve (n. phrenicus) (Fig. 266, 268, 269, 271). The motor fibers of the phrenic nerve are directed to the diaphragm, and the sensory fibers innervate the pleura and pericardium (Fig. 266).
| Rice. 268. Scheme of spinal nerves 1 - great auricular nerve; 2 - lesser occipital nerve; 3 - supraclavicular nerves; 4 - nerves of the cervical plexus; 5 - subclavian nerve; 6 - suprascapular nerve; 7 - brachial plexus; 8 - phrenic nerve; 9 - subscapular nerve; 10 - median nerve; 11 - musculocutaneous nerve; 12 - thoracodorsal nerve; 13 - axillary nerve; 14 - long thoracic nerve; 15 - medial cutaneous nerve of the shoulder; 16 - great splanchnic nerve; 17 - radial nerve; 18 - ulnar nerve; 19 - medial cutaneous nerve of the forearm; 20 - intercostal nerves; 21 - small splanchnic nerve; 22 - nerves of the lumbar plexus; 23 - iliohypogastric nerve; 24 - ilioinguinal nerve; 25 - nerves of the sacral plexus; 26 - genital-femoral nerve; 27 - superior gluteal nerve; 28 - lower gluteal nerve; 29 - posterior cutaneous nerve of the thigh; 30 - obturator nerve; 31 - sciatic nerve |
The brachial plexus (plexus brachialis) (Fig. 268, 273, 277) is formed by the branches of the four lower cervical nerves and the anterior branch of the 1st thoracic nerve. The branches of the plexus extend to the neck between the anterior and middle scalene muscles and are directed to the axillary region. The plexus consists of a supraclavicular section, formed by short branches heading to the shoulder girdle, chest and back, and a subclavian section, which includes long branches innervating the skin and muscles of the free part of the upper limb (with the exception of the axillary nerve (n. axillaris) (Fig. . 268, 272, 273), going to the shoulder girdle).
| Rice. 269. Plexus of spinal nerves, front view 1 - cervical plexus; 2 - phrenic nerve; 3 - sympathetic trunk; 4 - median nerve; 5 - intercostal nerves; 6 - medial cutaneous nerve of the shoulder; 7 - conus medullaris; 8 - ilioinguinal nerve; 9 - lumbar plexus; 10 - lateral cutaneous nerve of the thigh; 11 - sacral plexus; 12 - femoral nerve; 13 - obturator nerve; 14 - anterior cutaneous branches of the femoral nerve | |
| Rice. 270. Plexus of spinal nerves, posterior view 1 - greater occipital nerve; 2 - lesser occipital nerve; 3 - great auricular nerve; 4 - nerves of the cervical plexus; 5 - lateral cutaneous nerve of the shoulder; 6 - posterior cutaneous branches of the thoracic nerves; 7 - nerves of the lumbar plexus; 8 - nerves of the sacral plexus | |
| Rice. 271. Nerves of the diaphragm 1 - muscle that lifts the spine; 2 - external oblique abdominal muscle; 3 - internal oblique abdominal muscle; 4 - thoracic aorta; 5 - esophagus; 6 - right phrenic nerve; 7 - inferior vena cava; 8 - left phrenic nerve |
The supraclavicular section includes: - the dorsal nerve of the scapula (n. dorsalis scapulae), which goes to the rhomboid muscle and the levator scapulae muscle; - long thoracic nerve (n. thoracicus longus) (Fig. 267, 268), innervating the serratus anterior muscle; - medial and lateral pectoral nerves (nn. pectorales medialis et lateralis) (Fig. 267, 272), going to the pectoralis major and minor muscles; - subclavian nerve (n. subclavius) (Fig. 268), which innervates the subclavian muscle; - suprascapular nerve (n. suprascapularis) (Fig. 268), next to the supraspinatus and infraspinatus muscles; - subscapularis nerve (n. subscapularis) (Fig. 268, 272), heading to the subscapularis muscle and the teres major muscle; - thoracodorsal nerve (n. thoracodorsalis) (Fig. 268, 272), which is a branch of the subscapular nerve and innervates the latissimus dorsi muscle. The subclavian region is located in the axillary region and consists of three bundles: medial, lateral and posterior. The trunks of these bundles innervate the axillary artery and are the beginning of long branches. The medial trunk includes: - the medial cutaneous nerve of the shoulder (n. cutaneus brachii medialis) (Fig. 268, 269, 272, 273), heading to the skin of the medial surface of the shoulder; - medial cutaneous nerve of the forearm (n. cutaneus antebrachii medialis) (Fig. 268, 272, 273), innervating the skin of the medial surface of the forearm; - ulnar nerve (n. ulnaris) (Fig. 268, 272, 273, 274), which is mixed. Its sensory fibers are directed to the skin of the medial parts of the hand. On the palmar surface they innervate the skin of the fifth finger and the ulnar side of the fourth finger, on the dorsal surface - the skin of the fourth and fifth fingers and the ulnar side of the third finger. Motor fibers in the forearm are directed to the flexor carpi ulnaris and the medial division of the flexor digitorum profundus. On the hand, they innervate the adductor pollicis muscle, the eminence muscles of the little finger, and the 3rd-4th lumbrical muscles.
| Rice. 272. Nerves of the shoulder girdle 1 - lateral pectoral nerve; 2 - subscapular nerve; 3 - axillary nerve; 4 - thoracodorsal nerve; 5 - musculocutaneous nerve; 6 - medial cutaneous nerve of the shoulder; 7 - radial nerve; 8 - median nerve; 9 - medial cutaneous nerve of the forearm; 10 - ulnar nerve; 11 - lateral cutaneous nerve of the forearm |
The lateral trunk includes: - the median nerve (n. medianus) (Fig. 268, 269, 272, 273, 274), which is also classified as mixed. It emerges from the lateral and medial trunks. Sensitive fibers are directed to the skin of the lateral part of the palmar surface and the skin of the 1st, 2nd and 3rd fingers, as well as to the radial side of the 4th finger and partly to the dorsum of these fingers. Motor fibers in the forearm innervate the flexors of the forearm, with the exception of the flexor carpi ulnaris and flexor digitorum profundus, and are also directed to the pronator quadratus and teres muscles. On the hand, the motor part innervates the muscles of the eminence of the thumb; - musculocutaneous nerve (n. musculocutaneus) (Fig. 268, 272, 273), which is mixed. Its branches are directed to the flexors of the anterior surface of the shoulder; - lateral cutaneous nerve of the forearm (n. cutaneus anterbrachii lateralis) (Fig. 272, 273), which is the terminal branch of the previous nerve and innervates the forearm area. The posterior trunk includes: - the radial nerve (n. radialis) (Fig. 268, 272, 273), which is mixed. Sensitive fibers are directed to the skin of the lateral parts of the dorsum of the hand and the 1st and 2nd fingers, as well as the radial side of the 3rd finger. Motor fibers innervate the extensors of the shoulder and forearm; - posterior cutaneous nerve of the shoulder (n. cutaneus brachii posterior), which is a sensitive branch of the radial nerve and is directed to the skin of the posterior surface of the shoulder; - posterior cutaneous nerve of the forearm (n. cutaneus anterbrachii posterior), which is also a sensitive branch of the radial nerve and innervates the skin of the posterior surface of the forearm. The anterior branches of the thoracic nerves do not form plexuses. Intercostal nerves (nn. intercostales) (Fig. 268, 269, 275, 277) are mixed and arise from the posterior branches. Their sensory fibers are directed to the skin of the chest and abdomen, and motor fibers are directed to the intercostal muscles, levator ribs, serratus posterior muscles, transverse thoracic muscles, as well as to the transverse and rectus abdominis muscles, external and internal oblique abdominal muscles.
| Rice. 273. Scheme of nerves of the upper limb 1 - supraclavicular nerve; 2 - brachial plexus; 3 - musculocutaneous nerve; 4 - axillary nerve; 5 - medial cutaneous nerve of the shoulder; 6 - lateral cutaneous nerve of the shoulder; 7 - ulnar nerve; 8 - median nerve; 9 - radial nerve; 10 - lateral cutaneous nerve of the forearm; 11 - medial cutaneous nerve of the forearm; 12 - superficial branch of the ulnar nerve; 13 - deep branch of the ulnar nerve; 14 - common palmar digital nerves; 15 - own palmar digital nerves |
The lumbar plexus (plexus lumbalis) (Fig. 268, 269, 270, 277) is formed by the branches of the 12th thoracic nerve and the 1st-4th lumbar nerves and lies behind and partially in the thickness of the psoas major muscle, from under the lateral edge of which they emerge branches of the lumbar plexus:
- iliohypogastric nerve (n. iliohypogastricus) (Fig. 268, 276), which is classified as mixed. Its sensory fibers go to the skin over the tensor fascia lata and the gluteus medius muscle, as well as to the skin of the suprapubic region. Motor fibers are directed to the external and internal oblique and rectus abdominis muscles; - ilioinguinal nerve (n. ilioinguinalis) (Fig. 268, 269, 276), which is also mixed, the sensory fibers of which innervate the skin of the scrotum in men and the labia in women, and the motor fibers are directed to the iliacus muscle and the quadratus lumborum muscle; - genitofemoral nerve (n. genitofemoralis) (Fig. 268, 276), which is mixed, consists of two branches. The branches of the genital branch (r. genitalis) innervate the fleshy shell of the scrotum and the muscle that lifts the testicle. The femoral branch (r. femoralis) goes to the skin below the inguinal ligament; - lateral cutaneous nerve of the thigh (n. cutaneus femoris la-teralis) (Fig. 269, 276), which is sensitive and innervates the skin of the lateral surface of the thigh; - obturator nerve (n. obturatorius) (Fig. 268, 269, 276), which is mixed. Its sensory fibers go to the skin of the lower medial surface of the thigh, and motor fibers go to the muscles of the medial thigh; - femoral nerve (n. femoralis) (Fig. 269, 276), which belongs to the mixed nerve and is the largest nerve of the lumbar plexus. The anterior cutaneous branches (rr. cutanei anteriores) (Fig. 276) are sensitive and are directed to the skin of the anterior surface of the thigh. The saphenous nerve (n. saphenus) (Fig. 276) - the longest branch of the femoral nerve - runs along the great saphenous vein and gives off many branches going to the skin of the anteromedial part of the leg and the medial parts of the dorsum of the foot. The muscular branches (rr. musculares) of the femoral nerve are directed to the psoas major muscle, iliacus muscle, quadriceps and sartorius muscles of the thigh.
| Rice. 274. Nerves of the hand 1 - ulnar nerve; 2 - median nerve; 3 - superficial branches of the ulnar nerve; 4 - common palmar digital nerves; 5 - own palmar digital nerves | |
| Rice. 275. Intercostal nerves 1 - spinal cord; 2 - spinal nerve; 3 - central intercostal nerves; 4 - thoracic aorta; 5 - lateral cutaneous thoracic branch; 6 - external intercostal muscle; 7 - anterior cutaneous thoracic branch; 8 - internal intercostal muscle |
The sacral plexus (plexus sacralis) (Fig. 268, 269, 270, 277) is formed by the anterior branches of the 4th-5th lumbar nerves, the anterior branches of the sacral nerves and the coccygeal nerve. The branches are divided into short and long and are directed to the greater sciatic foramen, forming a triangular plate located on the anterior surface of the piriformis muscle.
| Rice. 276. Scheme of nerves of the lower limb 1 - iliohypogastric nerve; 2 - obturator nerve; 3 - ilioinguinal nerve; 4 - femoral nerve; 5 - genital-femoral nerve; 6 - lateral cutaneous nerve of the thigh; 7 - sciatic nerve; 8 - posterior cutaneous nerve of the thigh; 9 - common peroneal nerve; 10 - tibial nerve; 11 - medial cutaneous nerve of the calf; 12 - deep peroneal nerve; 13 - saphenous nerve; 14 - superficial peroneal nerve; 15 - lateral cutaneous nerve of the calf; 16 - sural nerve; 17 - medial and lateral plantar branches |
Short branches include: - muscular branches (rr. musculares), innervating the quadratus femoris, superior and inferior gemellus muscles, piriformis and obturator internus muscles; - superior gluteal nerve (n. gluteus superior) (Fig. 268), which innervates the tensor fascia lata, the gluteus medius and minimus muscles; - lower gluteal nerve (n. gluteus inferior) (Fig. 268), heading to the gluteus maximus muscle; - the genital nerve (n. genitalis) is classified as mixed. Sensory fibers innervate the skin of the perineum and external genitalia, and motor fibers innervate the muscles of the perineum. Long branches include: - posterior cutaneous nerve of the thigh (n. cutaneus femoris posterior) (Fig. 268, 276), which is sensitive and goes to the skin of the posterior surface of the thigh; - sciatic nerve (n. ischiadicus) (Fig. 268, 276), which belongs to the mixed nerve and is the largest nerve in the human body. Many branches extend from it, heading to the muscles of the posterior thigh. The nerve itself descends to the upper part of the popliteal fossa, where it divides into the tibial and peroneal nerves. The tibial nerve (n. tibialis) (Fig. 276) runs along the posterior tibial artery between the deep and superficial flexors of the tibia and behind the medial malleolus of the tibia it enters the plantar surface of the foot. In the area of the popliteal fossa, the tibial nerve gives off the following branches: - the medial cutaneous nerve of the calf (n. cutaneus surae medialis) (Fig. 276) is directed to the skin of the posteromedial surface of the leg. In the lower part of the leg it unites with the lateral cutaneous nerve of the calf. Together they form the sural nerve (n. suralis) (Fig. 276), passing behind the lateral malleolus and innervating the lateral parts of the dorsum of the foot; — muscular branches (rr. musculares) innervate the muscles of the posterior surface of the lower leg.
| Rice. 277. Projection of nerve plexuses onto the spinal column 1 - cervical plexus; 2 - brachial plexus; 3 - intercostal nerves; 4 - lumbar plexus; 5 - sacral plexus |
On the lower leg, the tibial nerve gives off the following branches: - medial calcaneal branches (rr. calcanei medialis) are directed to the skin of the medial parts of the heel; — muscular branches (rr. musculares) innervate the deep layer of the posterior group of muscles of the lower leg. On the surface of the foot, the tibial nerve is divided into medial and lateral plantar branches (rr. plantares medialis et lateralis) (Fig. 276), which are mixed and follow in the same direction as the plantar arteries. Sensitive fibers of the medial plantar nerve are directed to the skin of the medial part of the sole of the foot and to the skin of the I, II, III, IV fingers. Motor fibers are directed to the flexor digitorum brevis muscle, the abductor hallucis muscle and the 1st-2nd lumbrical muscles. The motor fibers of the lateral plantar nerve innervate the flexor of the little toe brevis, the abductor of the little toe, the adductor hallucis muscle, the quadratus plantae muscle, the interosseous muscles and the 3-4th lumbrical muscles. The common peroneal nerve (n. fibularis communis) (Fig. 276) is a mixed nerve and in the lateral part of the popliteal fossa is divided into the superficial and deep peroneal nerves. The main branches of the common peroneal nerve are: - the lateral cutaneous nerve of the calf (n. cutaneus surae late-ralis) (Fig. 276), heading to the skin of the posterolateral parts of the leg and uniting with the medial cutaneous nerve of the calf; - superficial peroneal nerve (n. fibularis superficialis) (Fig. 276), which is mixed. Its sensory fibers innervate most of the skin on the dorsum of the foot, and motor fibers innervate the long and short peroneal muscles; - deep peroneal nerve (n. fibularis profundus) (Fig. 276), following along the tibial artery. Its sensitive branch gives off many branches into the skin of the dorsum of the foot in the area of the first interdigital space. Motor fibers innervate the anterior group of muscles of the lower leg and the muscles of the dorsum of the foot.
| Rice. 278. Area of innervation of the trunk, front view I - cutaneous branches of the cervical plexus; II - supraclavicular nerves; III - lateral cutaneous nerve of the forearm; IV - medial cutaneous nerve of the shoulder; V - anterior cutaneous branches of the intercostal nerves; VI - lateral cutaneous branches of intercostal nerves; VII - lateral cutaneous branch of the iliohypogastric nerve; VIII - anterior cutaneous branches of the iliohypogastric nerve; IX - ilioinguinal nerve; X - lateral cutaneous nerve of the thigh; XI - branches of the genital-femoral nerve; XII - branches of the sacral plexus; XIII - anterior cutaneous branches of the femoral nerve; XIV - cutaneous branch of the obturator nerve | |
| Rice. 279. Areas of innervation of the body, rear view I - suprascapular nerve; II - lateral cutaneous nerve of the forearm; III - lateral cutaneous branches of the thoracic nerves; IV - medial cutaneous nerve of the shoulder; V - posterior cutaneous nerve of the shoulder; VI - lateral cutaneous branches of intercostal nerves; VII - medial cutaneous branches of the thoracic nerves; VIII - branches of the lumbar nerves; IX - medial cutaneous branches of the sacral nerves; X - lateral cutaneous branch of the iliohypogastric nerve; XI - lateral cutaneous nerve of the thigh; XII - branches of the posterior cutaneous nerve of the thigh | |
| Rice. 280. Areas of innervation of the upper limb A - palmar surface; B - dorsal surface: I - transverse nerve of the neck; II - subclavian nerves; III - lateral cutaneous nerve of the forearm; IV - branches of the thoracic nerves; V - medial cutaneous nerve of the shoulder; VI - posterior cutaneous nerve of the shoulder; VII - lateral cutaneous nerve of the forearm; VIII - medial cutaneous nerve of the forearm; IX - branches of the median nerve; X - branches of the ulnar nerve; XI - branches of the radial nerve; XII - deep branches of the median nerve; XIII - deep branches of the ulnar nerve; XIV - branches of intercostal nerves; XV - posterior cutaneous nerve of the forearm; XVI - deep branches of the radial nerve | |
| Rice. 281. Areas of innervation of the lower limb A - anterior surface; B - posterior surface: I - lateral cutaneous branch of the iliohypogastric nerve; II - branches of the genital-femoral nerve; III - ilioinguinal nerve; IV - lateral cutaneous nerve of the thigh; V - cutaneous branch of the obturator nerve; VI - anterior cutaneous nerve of the thigh; VII - branches of the saphenous nerve; VIII - branches of the common peroneal nerve; IX - branches of the superficial peroneal nerve; X - branches of the sural nerve; XI - branches of the deep peroneal nerve; XII - branches of the lumbar nerves; XIII - medial cutaneous branches of the sacral nerves; XIV - posterior cutaneous nerve of the thigh; XV - branches of the tibial nerve | |
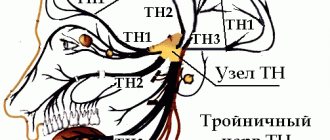
| Rice. 282. Areas of innervation of the head and neck I - branches of the frontal, orbital and trigeminal nerves; II - branches of the zygomatic, infraorbital, maxillary and trigeminal nerves; III - branches of the greater occipital nerve; IV - branches of the auriculo-occipital, mental, mandibular and trigeminal nerves; V - branches of the lesser occipital nerve; VI - branches of the greater auricular nerve; VII - subcutaneous branches of the dorsal nerve of the scapula; VIII - transverse nerve of the neck; IX - supraclavicular nerves |
Treatment of intercostal neuralgia
How to treat intercostal neuralgia? Therapy is carried out in two directions:
- It is necessary to alleviate the main symptom of the disease - chest pain.
- At the same time, it is necessary to identify the cause - the disease that led to compression or irritation of the nerve - and treat it.
In the acute stage of the disease, the doctor prescribes bed rest and recommends sleeping on a flat and firm bed. To combat pain, non-steroidal anti-inflammatory drugs are used, and various ointments help. In case of severe pain, a novocaine blockade is performed: the place where the affected nerve is located is injected with an anesthetic solution. There are also special patches with anesthetics.
Vitamins are prescribed to improve the condition of nervous tissue, muscle relaxants to relieve muscle spasms. Prolonged pain leads to a person becoming overly excitable and nervous, in which case sedatives are prescribed. Physiotherapy procedures help: Sollux, electrophoresis, UHF. A neurologist can prescribe massage and acupuncture sessions.
Is it possible to cope with the disease on your own? Over-the-counter pain medications and folk remedies can help relieve pain for a while. But in order to prescribe truly effective treatment for intercostal neuralgia on the right or left, you need to understand what causes it. Improper self-medication can be harmful.
We will call you back
Message sent!
expect a call, we will contact you shortly
The main symptom of intercostal neuralgia is pain. It spreads along the rib, as if encircling the right or left half of the chest, and can be sharp, stabbing, burning, or dull, aching. The pain intensifies during inhalation, because of this the person cannot breathe deeply. Movements, changes in body position, coughing, and sneezing also lead to aggravation.
Painful sensations occur if you press on certain points between two adjacent ribs along their course. This symptom is checked by a neurologist during an examination.
Other possible symptoms of intercostal neuralgia on the right and left (as well as pain, occur in the area of the affected nerve):
- twitching of the chest muscles;
- increased sweating;
- redness or paleness of the skin;
- numbness.
With intercostal neuralgia on the left, a person may complain that his heart and stomach hurt. Pain may radiate under the shoulder blade, to the collarbone area.
Similar chest pains can occur with diseases of the heart, lungs, pleura, and spine. An incorrect diagnosis and lost time can lead to serious consequences.
content .. 180 181 182 183 184 185 186 187 188 189 ..Intercostal nerves (human anatomy)
Intercostal nerves
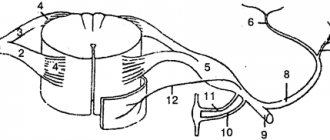
, nn. intercostales, are the abdominal branches of the I - XII thoracic spinal nerves. Upon departure from nn. spinales intercostal nerves enter the intercostal spaces and extend ventrally between the internal and external intercostal muscles to the sternum. On their way, the intercostal nerves give off cutaneous branches: lateral, rami cutanei laterales, on the side wall of the body and anterior, rami cutanei anteriores, at the sternum. According to the position of the nerves, the cutaneous branches are called thoracic or abdominal. Each lateral branch is divided into anterior and posterior branches, and the anterior branch is divided into medial and lateral branches. The upper 6 intercostal nerves are located throughout the intercostal spaces, and the lower 6 extend onto the anterior abdominal wall (Fig. 223).
Rice. 223. Diagram of the structure of intercostal nerves
The intercostal nerves innervate the intercostal muscles, the transverse thoracic muscle, the muscles of the anterior abdominal wall and some back muscles: mm-serrati posteriores superiores et inferiores, levatores costarum. In addition, they participate in the innervation of the pleura and peritoneum.
Cutaneous nerves innervate the skin of the body, maintaining a clear segmentation of the innervation territories, which look like horizontal stripes. The territory of innervation of the cutaneous branches of the V intercostal nerve corresponds to the level of the nipple, VII - the xiphoid process, X - the umbilicus, XII - the supra-inguinal zone. The division of the zones of innervation of the anterior and lateral branches occurs somewhat laterally from the lateral edge of the rectus abdominis muscles. Cutaneous nerves give branches to the mammary gland.
Lumbosacral plexus nevus (human anatomy)
The pelvic girdle and lower limb are innervated by the most powerful nerve plexus - the lumbosacral, plexus lumbosacralis, which consists of two plexuses - the lumbar, plexus lumbalis, and the sacral, plexus sacralis, connected through the lumbosacral trunk, truncus lumbosacralis.
Lumbar plexus of nerves (human anatomy)
Lumbar plexus
, plexus lumbalis, consists of the abdominal branches of the I, II, III and partially IV lumbar spinal nerves (Fig. 224).
Rice. 224. Lumbar plexus. 1 - quadratus lumborum muscle; 2 - XII intercostal nerve; 3 - iliohypogastric and ilioinguinal nerves; 4 - lateral cutaneous nerve of the thigh; 5 - femoral nerve; 6 - lateral cutaneous nerve of the thigh (in the thigh area); 7 - anterior cutaneous branch of the femoral nerve; 8 - femoral branch of the genital-femoral nerve; 9 - sacral plexus; 10, 11 — lumbosacral trunk; 12 - lumbar node of the sympathetic trunk; 13 - anterior branch of the II lumbar nerve
The abdominal branches that form the plexus are connected to each other by loop-like connections and run anterior to the transverse processes of the lumbar vertebrae between the two initial parts of m. psoas major, where the plexus gives off its branches.
1. Iliohypogastric nerve
, n. iliohypogastrics (from LI), comes out of m. psoas major on the anterior surface of the quadratus lumborum muscle, pierces the tendon stretch of the m. transversus abdominis and runs anteriorly above the iliac crest between the transverse and internal oblique abdominal muscles, giving them muscle branches. With its lateral cutaneous branch, ramus cutaneus lateralis, it innervates the skin above the greater trochanter of the femur, and the final one, the anterior cutaneous branch, ramus cutaneus anterior, innervates the skin in the area of the superficial ring of the inguinal canal.
2. Ilioinguinal nerve
, n. ilioinguinalis, starts from the abdominal branch of the first lumbar spinal cord or from the iliohypogastric nerve and goes below the latter into the inguinal canal, appearing in the subcutaneous tissue at its superficial ring. Along its length, the nerve sends branches to the muscles of the abdominal wall.
The terminal section of the nerve is divided into the lateral cutaneous branch, ramus cutaneus lateralis, which innervates the skin of the medial inguinal region, and the anterior scrotal branch, nn. scrotales anter lores, - in men and anterior labial nerves, nn. labiates anteriores, - in women, innervating the skin of the scrotum or labia majora.
3. Genitofemoral nerve
, n. genitofemoralis (from LI-LII) pierces the psoas major muscle and runs down its anterior surface, dividing here into two terminal branches: 1) the genital, ramus genitalis, which joins the spermatic cord in the inguinal canal, the formation of which and the shell of the testicle it innervates; 2) femoral, ramus femoralis, innervating the skin of the thigh below the inguinal fold.
4. Lateral cutaneous nerve of the thigh
, n. cutaneus femoris lateralis (from LII-LIII), emerges from m. psoas major at its lateral edge on the anterior surface of the iliacus muscle. Then it descends downwards and outwards, passes through the anterior abdominal wall medial to the anterior superior iliac spine and on the thigh, penetrating through the fascia lata, branches into the skin of the lateral surface of the thigh.
5. Femoral nerve
, n. femoralis (from LI-LIV), formed on the anterior internal surface of m. psoas major, then crosses it and goes between it and m. iliacus in the lacuna musculorum on the anterior surface of the thigh, separating from the femoral artery fascia iliopectinea. On the thigh it branches, giving: 1) muscular branches, rami musculares, to mm. quadriceps, restineus and sartorius; 2) anterior cutaneous branches, rami cutanei anteriores, innervating the skin of the anteromedial surface of the thigh. One of the cutaneous branches is the hidden nerve, n. saphenus, goes along with the femoral artery to the canalis adductorius, exits through its anterior opening with a. genus descendens, descending under the sartorius muscle to the medial surface of the tibia, where it spreads down near the v. saphena magna, innervating the skin of the medial surface of the leg (rami cutanei mediales). It gives off the infrapatellar branch, ramus infrapatellaris, which innervates the skin of the knee joint area below the patella.
6. Obturator nerve
, n. obturatorius (from LI-LIV), located initially behind and inwardly m. psoas major, medial to the femoral nerve, then goes to the pelvis, where it passes near the insertion of m. levator ani to the obturator canal, through which it enters the medial osteofascial space of the thigh, dividing into anterior and posterior branches. The posterior branch, ramus posterior, innervates mm. obturatorius externus, adductor magnus and gives branches to the hip-femoral joint. The anterior branch, ramus anterior, supplies nerves mm. pectineus, adductor brevis et longus, gracilis. In addition, it gives off a cutaneous branch, ramus cutaneus, to the skin of the medial surface of the thigh.
content .. 180 181 182 183 184 185 186 187 188 189 ..
How to distinguish the signs of intercostal neuralgia from the symptoms of other diseases?
It is especially important to distinguish in time between irritation of the intercostal nerves and angina pectoris, a condition in which the heart muscle does not receive enough oxygen-rich blood. Main differences:
- With intercostal neuralgia, pain persists for a long time. With angina pectoris, they last about 5 minutes and go away if you take nitroglycerin.
- With neuralgia, pain intensifies during deep inspiration, movements, sneezing and coughing, but with angina pectoris this does not happen.
Other dangerous conditions that need to be distinguished from intercostal neuralgia are myocardial infarction and PE ( pulmonary embolism) . Typically, a heart attack occurs after physical exertion or after a person becomes very nervous. The pain is accompanied by signs of dysfunction of the cardiovascular system:
- The man turns pale. Fingertips, nose, lips may become bluish.
- Sticky cold sweat appears.
- Shortness of breath that persists even when the person is resting - lying or sitting.
- Blood pressure drops.
- The fear of death arises.
You should not engage in self-diagnosis - erroneous conclusions are fraught with serious consequences. See your doctor. Get examined at the clinic. In any case where there is a suspicion of a heart attack, it is better to play it safe and immediately call an ambulance.
Treatment of symptoms of intercostal neuralgia on the right and left
The leading symptom of the disease – pain – is helped by painkillers (non-steroidal anti-inflammatory drugs), anesthetic patches, novocaine blockades, and physiotherapy.
But coping with the symptoms does not mean curing the disease. Therefore, treatment should also be aimed at the cause. A thorough diagnosis must first be carried out - this is only possible in a clinical setting.
Take care of yourself, book a consultation now
Message sent!
expect a call, we will contact you shortly
“Intercostal neuralgia” is not one specific diagnosis, but a collective term. It refers to different conditions that lead to damage to the intercostal nerves and, as a result, to chest pain.
Why is it important to understand the cause of this condition in each specific case? This will allow you to prescribe effective treatment that will help you recover or keep your chronic disease under control.
The main causes of intercostal neuralgia
Most often, the following reasons lead to compression and irritation of the intercostal nerves:
- Osteochondrosis. A degenerative disease that primarily affects the intervertebral discs. Their height decreases - the distance between adjacent vertebrae decreases, this leads to compression of the nerve roots.
- Hypothermia, exposure to drafts.
- Intense physical activity, sudden awkward movements.
- Working in an awkward position when your back is constantly under tension.
- Injuries to the chest and thoracic spine, previous surgeries.
- Frequent and severe stress.
- Viral infections. The most common cause is a cold, shingles.
- Chronic spasm of the back muscles. It promotes irritation of nerve receptors.
Most often, intercostal neuralgia occurs in older people, when the causes of the disease are layered with age-related changes in the spine and blood vessels.
Causes of the disease
At the level of the thoracic part of the spine, nerves emerge from the spinal cord symmetrically on both sides, following under each rib. They innervate the skin and muscles of the corresponding area, and have connections with nerves going to the internal organs.
Osteochondrosis is the most common cause of a pinched nerve in the chest. With this disease, the height of the intervertebral discs decreases, and the shock-absorbing properties of the cartilage are lost. There are often bone deformities that increase pressure on the nerve. Often the disease develops against the background of scoliosis – a sideways curvature of the spine.
Diabetes mellitus, atherosclerosis, arterial hypertension, chronic renal and endocrine diseases, age-related changes lead to damage to blood vessels and nerves. This also worsens the working conditions of the muscles, ligaments, discs, and joints of the spine.
Prolonged stay in a forced position, heavy lifting, uneven load on the back (carrying a heavy bag in one hand) provoke the appearance of pain. A pinched nerve in the thoracic region can be on the left, right, or both sides.
What other diseases lead to girdle pain in the chest?
Often people tend to dub “neuralgia” any girdle pain along the ribs. But this symptom may have other causes, including:
- Spondylosis is an inflammatory disease that causes damage to the vertebral bodies and deformation of the spinal column.
- Hormonal spondylopathy is a pathology that develops in older people, for example, in women after menopause. The spine is deformed, and disorders occur in the vessels that supply it.
- Malignant tumors - those that arise in the spine itself or metastases from other parts of the body.
- Ankylosing spondylitis is a chronic inflammatory process that leads to decreased mobility in the spinal column.
- Gastritis and other diseases of internal organs.
How does the treatment of intercostal neuralgia depend on the cause?
With intercostal neuralgia, it is not enough to eliminate the main symptom of the disease - pain. You should always look for and treat the underlying cause. The doctor prescribes therapy individually, depending on the pathological changes detected during examination and examination, and the final diagnosis.
Make an appointment at the Medica24 International Clinic - get a consultation with an experienced neurologist and undergo an examination using our modern equipment. This will help to quickly and accurately establish a diagnosis and prescribe the correct treatment in a timely manner.
Get a consultation with a doctor
Message sent!
expect a call, we will contact you shortly
The main manifestation of intercostal neuralgia – chest pain – can also occur with many other diseases. And figuring out the correct diagnosis is not always easy.
The diagnostic process begins with a visit to a neurologist. The doctor will ask you some questions:
- When did you first experience pain? How did this happen? What preceded this?
- What is the nature of the pain, when does it usually occur, how often, how long does it last?
- Do you have chronic lung or heart diseases? Are you monitoring your blood pressure?
- What infections have you had? Have you had any chest injuries or surgery?
- What other symptoms bother you?
You may be asked to complete a special “pain questionnaire”. The doctor will perform a complete neurological examination to rule out other neurological diseases. You will then be given an examination.
To understand the causes of irritation or compression of the intercostal nerve, the doctor may prescribe x-rays, CT, MRI, and, if necessary, other studies.
Clinical manifestations
A pinched nerve in the thoracic spine is accompanied by the following symptoms:
- Pain in the back, chest, which spreads between the ribs. It can radiate to the lower back, under the shoulder blade, or into the arm. It happens in the form of attacks, very strong, burning, stabbing or barely noticeable, aching, but is constantly present. The pain intensifies with movement, breathing, coughing, sneezing. Sometimes it is difficult for a person to raise his arms or bend over.
- Loss of sensitivity along the nerve. A person may feel numbness, a crawling sensation, or, conversely, hyperesthesia, that is, increased sensitivity of the skin. Any touch then causes discomfort or pain.
- Considering that movements are accompanied by pain, breathing becomes shallow, which can further lead to problems with the respiratory system.
- Severe constant pain exhausts a person, leads to fatigue, irritability, and a general decrease in tone and immunity.
Instrumental methods for diagnosing intercostal neuralgia
At the Medica24 International Clinic, you can undergo examination using our own diagnostic equipment, which meets the most modern standards. It will help diagnose the disease at an early stage and take timely measures.
First of all, it is important to carry out a differential diagnosis of intercostal neuralgia with certain diseases of the spine, cardiovascular system, and lungs. To do this, if necessary, the neurologist will refer you for a consultation with a cardiologist or pulmonologist.
You may be prescribed an ECG, Holter monitoring, cardiac ultrasound, X-ray, CT and MRI of the chest, biochemical blood test, and bacteriological studies.