Metastasis is the migration of carcinogenic cells from the primary tumor to other organs, which is typical for most cancer tumors. This leads to the formation of secondary lesions in other tissues. Different types of cancer are characterized by different intensity of the metastatic process, which depends on the degree of malignancy and characteristics of the primary tumor. The more intense the spread, the more aggressive the cancer. For example, with skin melanoma, metastases to the brain occur frequently, unlike basal cell carcinoma. The metastatic process begins, as a rule, at the third stage of carcinogenesis, and at the fourth stage it already manifests itself quite strongly. There are two ways for cancer cells to migrate: through the blood and lymph. The appearance of metastatic tumors will be identical to the appearance of the cells of the primary tumor. When neoplasias are detected in the brain, it is important to ensure that these are secondary tumors. For this purpose, a complete examination of the body is carried out. In the presence of metastases in the brain, the prognosis worsens, life expectancy is estimated at months, in some cases weeks.
Metastasis formation
Metastases form after the development of a primary malignant neoplasm in other organs. The latter are formed as a result of mutagenesis or errors in the genetic material of somatic cells. At the initial stages, there is no metastatic process, but as it progresses, the tissues of the primary tumor grow into nearby organs. In the future, the disease worsens, cancer cells begin to break away from the primary focus and migrate through the blood or lymphatic channels (the integrity of the blood vessels is damaged). A metastatic cell attaches itself to an organ, germinates, and gives rise to a new lesion—a secondary tumor.
Important. In different individuals, the nature, timing and intensity of the formation of secondary metastatic foci are different, which is explained by the level of antitumor immunity.
Features of metastasis
The intensity of the metastatic process, the degree of malignancy, the formation of relapses, the treatment of brain metastases and the aggressiveness of cancer are influenced by the following circumstances:
- Stage of carcinogenesis. The life prognosis directly depends on the stage at which the cancer was discovered and surgically removed. The most successful will be removal of cancer at the first stage, however, this cannot guarantee a complete cure, so the patient must be constantly monitored.
- The location of the primary tumor largely determines the nature of the metastatic behavior of cancer and damage to other organs.
- The histological structure and form of cancer also influence the reasons for the spread of metastases. The most dangerous are poorly differentiated forms. Different types of carcinogenesis are characterized by different features of cancer cell migration. If the tumor is dense and slowly growing, for example, cylindroma, then metastases to the brain are rare and, as a rule, only in the terminal stages. In other cases, even with good antitumor immunity, metastases form in the brain, for example, with the development of melanoma.
- Features of anticancer therapy. If it is possible to completely remove the primary tumor in the initial stages, with the administration of radiotherapy and chemotherapy, then in this case the treatment gives the most acceptable result.
- The older the patient, the more difficult the cancer is to treat.
Tumor metastases - symptoms and treatment
Tumor metastases are cancer cells that have spread throughout the body and become established in one or more internal organs. In 90% of cases, it is metastases that cause the death of a cancer patient [1][2]. Any malignant tumor can metastasize; this is one of the properties that distinguishes them from benign tumors.
It is now known that metastasis is a complex, dynamic process. It plays a role in the mutational load of the tumor (the number of mutations in the genetic code of cancer cells), the interaction between cancer and normal cells, and signaling molecules that are located in the intercellular substance (they interact with cells and control their growth and reproduction).
Probability of developing metastases
Whether metastases occur or not depends on several factors:
- Type of cancer. For example, basal cell carcinoma metastasizes extremely rapidly, and melanoma is a highly aggressive neoplasm in which metastases develop very quickly.
- Molecular genetic features of cancer. For example, triple negative breast cancer is more likely to metastasize than tumors that have estrogen receptors, progesterone receptors, or those associated with overexpression of the HER2 protein.
- The degree of malignancy of the tumor. The higher it is, the more aggressive the cancer and the higher the likelihood of it metastasizing.
- Features of localization. For example, breast cancer in the inner quadrant of the breast metastasizes more often than tumors in the lateral quadrants.
- Features of growth. Tumors with infiltrative growth metastasize more often and faster than tumors growing superficially. For example, fungal tumors of the colon and stomach are less malignant than infiltrative forms of cancer of these organs.
What affects the rate of spread of metastases?
The rate of spread of metastases also depends on the type of cancer, the degree of malignancy of the tumor and its molecular genetic characteristics. For example, high levels of TGF beta protein may increase the rate of metastasis.
However, more often in clinical practice, the rate of spread of metastases throughout the body is associated with the type of cancer and its location. For example, poorly differentiated tumors metastasize earlier than highly differentiated ones, and lung cancer, due to its good blood supply, spreads much faster than prostate cancer.
Once metastasis has occurred, it becomes very difficult to fight a malignant tumor; this is the last stage of cancer development . From this point on, treatment is palliative in nature: it helps to slow down the progression of cancer, prolong life and improve the condition, but not cure the patient [3].
Most often, malignant tumors metastasize to the bones, lungs, liver and brain. In some types of cancer, tumor cells spread along the surface of the peritoneum.
The complex chain of events, as a result of which a malignant cell breaks away from the mother tumor, migrates in the body and forms a secondary focus in another organ, is not fully understood, and work in this direction continues [1]. Some theories attempt to explain the causes of metastasis .
One of them says that due to accumulated mutations, an epithelial-mesenchymal transition : tumor cells begin to resemble those found in the body of the embryo and are involved in wound healing. They are irregular in shape, do not stay in place and can migrate in the body.
According to another theory, metastases occur from stem cells , which normally should replace cells that die as a result of damage or naturally. This theory is supported by the fact that tumor and stem cells have a number of common features in structure and biochemical processes.
It is believed that macrophages (“eater cells”), which normally should eliminate foreign particles, help spread metastases of a malignant tumor. In cancer, they support inflammation and angiogenesis (the process of forming new blood vessels). This promotes the migration of tumor cells.
In cancer patients, millions of cancer cells enter the bloodstream every day. But only a few of them can give rise to metastases. This depends on the histological type of the tumor (from which tissue it originated), the degree of aggressiveness of the tumor (stage of cancer), and cell differentiation (how much they have lost their normal features).
Metastases to the brain
Lead to the formation of secondary tumors in various parts of the brain. This almost always causes death. In general, any type of cancer can lead to this, but there are tumors that metastasize more often than other types of cancer:
- Metastases to the brain in skin cancer (melanoma) are more common than in other types. Approximately 50-73% of patients face this problem. In 10-45% of cases (at the time of diagnosis), melanoma is at stage 4, when there are already metastatic lesions. At the same time, every third patient exhibits neurological manifestations. In this case, a condition similar to a stroke often develops, because a hemorrhage forms in the pathological neoplasm. Treatment of brain metastases in melanoma is complicated by the fact that they are poorly sensitive to radiotherapy.
- Metastases in lung cancer form in 35-60% of cases. In this case, how long people live with brain metastases is determined by many factors (age, type of cancer, intensity of carcinogenesis, presence of metastatic lesions in other organs, and so on). According to statistics, such metastases in lung cancer are the most dangerous in terms of mortality. Most often they are characteristic of the fourth stage of pathogenesis. Only in 5% of cases will the patient live 2-3 years. As a rule, at this time there are already multiple neoplasms in the lymph nodes and other organs. The patient receives palliative treatment.
- In breast cancer in women, metastases to the brain are recorded in 20-30% of cases. At later stages, metastases are diagnosed in the brain and many other organs. Treatment is carried out with radiochemotherapy and hormone therapy. The quality of life deteriorates significantly, stroke, mental disorders, vertebral fractures due to brittle bones, cough due to lung damage, and so on are possible.
- Brain metastases in kidney cancer are characteristic of stage 4. In this case, there are secondary lesions in other organs (second kidney, lungs, other organs and multiple lymph nodes). The prognosis is unfavorable: only 8% of patients will live for about two years. Kidney cancer has a high risk of recurrence.
- Metastases from bladder cancer can be at the fourth stage. The prognosis is negative due to the presence of secondary tumors in other organs; most patients will not live more than a year. Removing the cancer is almost impossible; supportive treatment is prescribed.
- Brain metastases in intestinal and esophageal cancer are observed at stage 4. If they are present in other organs, the prognosis is negative - only 6% of patients will live more than a year.
In addition to these types of cancer, metastatic brain lesions can also form in other malignant neoplasms, for example, in the terminal stages of laryngeal or thyroid cancer, when the tumor grows into large main arteries.
Treatment of metastases
Without treatment, the life expectancy of a patient from the moment a metastatic lesion of the brain is detected hardly exceeds a month, but this is on average. Only the addition of high doses of hormones can double life expectancy and slightly improve its quality, but again only temporarily, while chemoradiotherapy can give up to six months of life.
Treatment tactics depend on several factors:
- Number, size and location of metastases;
- Possibility to remove lesions surgically;
- Sensitivity of the primary tumor to chemotherapy and radiation therapy;
- General condition of the patient;
- The presence of other metastases, the ability to fight them.
Prognostically unfavorable is the localization of the tumor in the posterior cranial fossa, inaccessible for manipulation, impaired circulation of cerebrospinal fluid and the likelihood of tumor wedging into natural cranial foramina. There is no doubt that only surgery, coupled with additional drug and radiation treatment, gives great hope. But neurosurgical intervention is possible with one or single tumor nodes, and, of course, technically accessible ones. Palliative surgery is performed when there is a threatening increase in pressure and bleeding, when the removal of even one of many nodes can radically improve the clinical picture in order to add conservative treatment in the future. There are different options for removing tumor nodes.
For types of cancer that are technically unremovable and sensitive to antitumor drugs, such as breast, small cell lung cancer and germ cell tumors of the testicle, chemotherapy is used at the first stage, which is then followed by irradiation of the entire brain. For radiosensitive tumors, treatment can begin with total brain irradiation. For tumors no larger than 3.5 cm and less than four nodes, stereotactic radiosurgery is effective as the only method. Several beams of radio waves are applied to the tumor from different sides; they intersect in one place - where the metastasis is located. As a result, cancer cells are destroyed, and surrounding healthy tissues receive the minimum safe dose. In combination with brain irradiation and chemotherapy, the result is better.
Radiation therapy is always accompanied by an increase in swelling of the brain tissue, so irradiation is always carried out against the background of dehydration - symptomatic therapy that relieves excess fluid. Therefore, the radiologist may refuse treatment to a patient who is resistant to diuretics, as well as with an already displaced brain, since further displacement can be fatal for the patient. They will not accept irradiation for a seriously ill patient with severe clinical manifestations, especially with convulsions or cloudy consciousness. After just one or two sessions of irradiation, the existing high intracranial pressure will be joined by radiation-induced tissue edema, and the patient’s already very unimportant condition will worsen.
Contact your doctor
Variants of sequences and combinations of methods are possible, both for newly detected brain metastases and for relapse after treatment. In any case, if active tactics are impossible and the process progresses, clinical guidelines recommend resorting to chemotherapy along with the best supportive symptomatic therapy (steroids, painkillers, anticonvulsants, etc.). The regimen is determined by the primary tumor, that is, some drugs help with lung cancer, and others with kidney cancer. Chemotherapy is carried out until signs of tumor progression are detected.
Treatment of metastases of malignant tumors in the brain is not the work of single enthusiasts, it is the work of a team of oncologists, neurosurgeons, radiologists, chemotherapists and resuscitators, armed with knowledge and excellent equipment for diagnosis and treatment, as in Euroonco clinics.
Symptoms and signs
As cancer progresses, it enters later stages (3 and 4). In this case, metastases form in the brain, so characteristic clinical signs begin to appear. Manifestations will depend on the area of the brain affected. In many cases, the signs are mirrored, i.e. if the tumor is in the right hemisphere, then the clinic will appear on the left side and vice versa.
Main features:
- dizziness, headache due to increased pressure inside the skull, while negative symptoms are not relieved by medications;
- dyspeptic symptoms, nausea and vomiting (vomiting does not bring relief), which is not associated with poisoning;
- various disorders of brain activity: confusion, memory impairment, speech impairment, epileptic seizures, hallucinations, etc.;
- vision, hearing, and smell suffer;
- the mental and emotional background changes, the person becomes rude, aggressive, overly irritable;
- the formation of epileptiform seizures with brain damage is more typical for the elderly;
- motor activity is impaired, coordination and fine motor skills suffer, it is difficult for the patient to maintain balance, gait is impaired, the ability to write, and so on.
Metastatic brain tumors
Patients are prescribed anticonvulsants, steroids, painkillers and psychotropic drugs. The main treatment method for metastatic brain tumors is usually radiotherapy, which is used alone, in combination with chemotherapy or surgery. The indication for surgical treatment is the presence of an operable solitary metastasis (a secondary lesion with an undetectable primary process) or a single metastasis with a controlled primary tumor.
Typically, operations are performed for metastatic brain tumors located in the cerebellum, temporal and frontal lobes, that is, in areas with a relatively low surgical risk. After surgery, radiotherapy or chemotherapy is prescribed. Sometimes the goal of surgical treatment is not to remove a metastatic brain tumor, but to urgently reduce life-threatening intracranial pressure. If necessary, such interventions can be carried out repeatedly.
Chemotherapy is usually ineffective. The exception is situations when the primary tumor responds well to cytostatics, for example, in breast cancer, small cell lung cancer or lymphoma. Patients with metastatic brain tumors that are sensitive to chemotherapy are prescribed drugs that can cross the blood-brain barrier. Chemotherapy must be supplemented with other treatment methods (usually radiotherapy).
A promising modern method for treating metastatic brain tumors is 3D conformal radiation therapy - irradiation with thin beams of radiation aimed at the tumor. This technique allows for maximum impact on the tumor with minimal radiation exposure to healthy tissue. The procedure is carried out under MRI or CT control. The method has a number of advantages over traditional operations (painlessness, non-invasiveness, absence of anesthesia and postoperative period). Indicated for multiple metastatic brain tumors and high surgical risk due to the location of the metastasis.
For secondary lesions in the spinal cord, the same methods are used as for brain damage. The use of corticosteroids can reduce pain in 85% of patients, and radiotherapy in 70% of patients. Half of the patients experience improvement in motor functions during radiotherapy. Surgical interventions are performed when metastatic brain tumors are insensitive to radiotherapy, when neurological disorders progress, or when nerve tissue is compressed by a bone fragment. Anterior decompression or laminectomy is performed. After surgery, local radiotherapy is prescribed (with the exception of tumors that are insensitive to radiation therapy).
Diagnostics
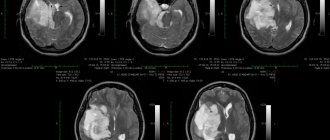
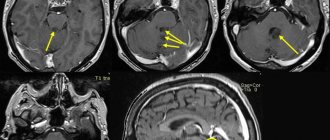
Since the formation of secondary tumors in the brain causes the death of the patient, it is important to identify the presence of a pathological formation as early as possible. If cancer is present, the patient must be diagnosed continuously to monitor the situation and timely identify secondary tumors in the brain. If the tumor in the head is small, it usually already has a pronounced clinical picture, however, it can be diagnosed at the earliest stages using computed tomography (CT) or magnetic resonance imaging (MRI). A biopsy is important to establish the metastatic process and clarify all the nuances of pathogenesis. The presence of metastases can be suspected even with a biochemical blood test.
Prognosis and prevention
In the absence of adequate therapy, the life expectancy of patients with cancer metastases to the brain does not exceed one month.
Corticosteroid therapy prolongs life by two to three months. With the help of radiation therapy, the life of patients is increased to six months. Oncologists at the Yusupov Hospital use innovative methods of treating cancer patients using ultra-modern medical equipment. This allows patients to live for several years longer. The only effective method for preventing cancer metastases in the brain is timely diagnosis and adequate therapy of primary tumors. To save your life, if early signs of a tumor process appear, contact the oncology clinic of the Yusupov Hospital. Make an appointment with an oncologist online or call the contact center at any time of the day or night, regardless of the day of the week.
Make an appointment
Treatment
What to do in case of metastases in the brain is decided by a council of doctors based on the diagnosis and medical history of the patient. Treatment of metastases in the head is very difficult, which is due to the inaccessibility of the location of secondary lesions in the brain, the presence of multiple tumors in other organs, the patient’s condition in the later stages, age and a number of other factors. Today, in the presence of secondary tumors in the head, stereotactic radiosurgical techniques are used, which stop or slow down the growth of pathological tissue. The best result is achieved when tumors are removed surgically, but at these stages treatment is always difficult. The method of treatment will depend on the location of the tumor, the intensity of damage to other organs and the general condition of the patient.
Main types of treatment
- Surgical treatment is possible only in cases where there is access to tumors in the brain. As a rule, in the terminal stages many other organs are already affected, so surgical treatment is carried out mainly for palliative purposes, to eliminate negative signs and alleviate the patient’s condition. In some cases, it is possible to remove a few tumors or metastases are removed en bloc (when they are located nearby). If there are many lesions in the brain, then surgical treatment is not advisable.
- Treatment with radiotherapy is more preferable in this case. For deep, hard-to-reach locations of secondary tumors in the brain, this type of treatment is the main one. For a few tumors, stereotactic proton therapy (irradiation of an organ from several sides) will be an effective method.
- Chemotherapy and drug treatment for brain metastases are not effective. Drugs are prescribed to relieve negative symptoms and reduce side effects. Thus, drug therapy is palliative.
Causes
Metastases in the brain are formed during the migration of atypical cells from malignant tumors of the following localizations:
- Nasopharyngeal region;
- Spinal column;
- Cervix;
- Ovaries;
- Bladder.
Doctors often detect brain metastases in patients suffering from abdominal lymphoma, choriocarcinoma.
The histological structure of the metastatic lesion is similar to the structure of the primary neoplasm. The group at increased risk of developing brain metastases includes cancer patients over 50 years of age, women with breast cancer, and men diagnosed with lung cancer.
Make an appointment
To which organs does breast cancer metastasize?
Most often, breast cancer spreads to the bones, lungs, liver, brain, and lymph nodes. Secondary lesions in other organs are less common.
Treatment of bone metastases in breast cancer
Metastases in the bones manifest themselves in the form of pain and swelling. The tumor destroys bone tissue, which threatens pathological fractures - they arise from a small mechanical load. In order to strengthen bone tissue, treatment for breast cancer metastases to the bones includes the use of a special group of drugs - bisphosphonates. In pathological fractures, bones are strengthened with screws, plates and other structures.
Treatment of lung metastases in breast cancer
With metastases in the lungs, the patient is bothered by a persistent chronic cough and chest pain. The sputum that comes out during a cough may contain blood. For single secondary lesions, surgical treatment of lung metastases from breast cancer can be performed.
Brain metastases in breast cancer
Metastases in the brain from breast cancer lead to headaches, which become more severe, persistent, and painful over time. Other possible symptoms: convulsions, blurred vision, nausea and vomiting, changes in personality and behavior.
Liver metastases in breast cancer
Secondary lesions in the liver disrupt its functioning and the outflow of bile. Jaundice, skin itching, abdominal pain, digestive and bowel problems occur. The biochemical blood test showed elevated levels of liver enzymes. Ascites, an accumulation of fluid in the abdominal cavity, may develop. Treatment of liver metastases from breast cancer may include methods such as:
- Radiofrequency ablation: a needle-shaped electrode is inserted into the tumor site and a high-frequency current is applied to it. Intra-arterial chemotherapy is the administration of chemotherapy drugs into the hepatic artery. Chemoembolization is the introduction of a chemotherapy drug into the vessel feeding the tumor in combination with emboli - particles that block the blood flow. Laparocentesis is puncture and removal of fluid from the abdominal cavity in case of ascites. Sometimes surgical treatment is indicated.
Metastases in lymph nodes in breast cancer
Most often, with breast cancer, metastases are found in the axillary lymph nodes. At the same time, the lymph nodes enlarge and become noticeable, they can be felt. Swelling and swelling occurs in the arm (lymphedema). If the cancer has spread to nearby (regional) lymph nodes, it can often still be treated with surgery.
Metastases of breast cancer in the thyroid gland
Metastasis of breast cancer to the thyroid gland is rare. In this case, the prognosis becomes much worse. Sometimes removal of the thyroid gland (thyroidectomy) is indicated to prevent and control complications.