Brain tumors are defined by pathological formations that arise against the background of impaired growth and differentiation of certain cells in its tissues. This process is caused by changes in the genetic apparatus of mutation cells. Such neoplasms are called tumors.
Pathological neoplasms are primary and secondary. The growth of a primary tumor occurs exclusively due to the own cells of the organ where it originated. If chemoradiotherapy does not produce a definite result during the treatment process, then rapid growth of metastases is possible. This education is secondary. The reverse process is also possible, when a secondary tumor arose in other organs, but spread to parts of the central nervous system.
There are two types of tumors: benign and malignant.
Benign neoplasms grow slowly and locally, and metastases are often absent. Despite being fairly stable, they are potentially dangerous. An increase in tumor size increases pressure on neighboring areas of the brain. This in turn leads to disruption of the vital functions of the body. Sometimes they can be qualitatively reborn. For a long time, such formations may not manifest themselves. The most common benign tumors of the central nervous system are:
- Neuroma - occurs due to damage to nerve endings;
- Glioma - develops as a result of hemorrhage in neurogic tissue;
- Neuroma - localized in the peripheral parts, forms nodules in the roots of the spinal cord;
- Paraganglioma - forms in any tissue where there are chromaffin cells, the cause of its occurrence is a genetic predisposition;
- Meningioma is the most common, metastases are possible. Occurs in the tissues of the meningeal membrane. The group at greatest risk for this neoplasm includes middle-aged women (from 30 to 40 years), including pregnant women.
- Schwannoma is a subtype of meningioma that affects nerve cells in the part of the brain that controls the auditory and vestibular systems.
- A cyst is characterized by clear boundaries and is a cavity in the tissues filled with fluid.
- Pituitary adenoma - excessive growth of abnormal pituitary cells leads to disruption of the hormonal system, and visual function also suffers, since the tumor compresses the optic nerves located nearby.
- Craniopharyngioma - develops in tissues located near the pituitary gland.
Malignant tumors are characterized by rapid growth of carcinogenic cells. They damage and compress surrounding tissues, which leads to disruption of many functions in the body. Cancer cells form metastases, spreading to distant organs. The body loses its ability to cope with the excessive production of toxins, which leads to a sharp deterioration in the patient’s condition.
The most common types of malignant cancers are:
- Glioma is one of the most common primary neoplasms that arises from brain parenchyma tissue.
- Sarcoma - a tumor is formed by modifying the connective tissue of different organs. It is distinguished by very fast growth. Relapses often occur during treatment.
- Teratoma is a fairly rare type of tumor, typical for the age group from 10 to 20 years. Both a malignant tumor and a benign one can develop. Scientists believe that the cause of the appearance of this type of neoplasm is a disturbance in the process of human embryonic development. This neoplasm can appear in areas with a predominance of germ cells - ovaries in women, testicles in men, sections of the sacrum, pituitary gland.
Initial signs of brain cancer
There are several main symptoms that indicate that medical attention should not be neglected. Initial signs of brain cancer may include:
- Prolonged headache, intensifying at a certain period of the day, as well as due to nervous exhaustion, excessive physical exertion;
- A sharp deterioration in vision;
- Continuous nausea and vomiting (it is important to distinguish it from the feeling of nausea during poisoning), anxiety, increasing depression and frequent mood swings, prolonged dizziness;
- Unusual sensations in the body such as weakness on only one side;
- Involuntary body movements, sharp and sudden convulsions, paralysis, epileptic attacks, hallucinations;
- Changes in the control of facial expressions, difficulty swallowing, disturbances in speech, attention, memory, and confusion occurs.
- The general hormonal balance is disrupted.
Symptoms and signs of brain cancer
Many other diseases have similar symptoms to the signs listed above. The initial stage of development of brain cancer in a patient is indicated by the combination of these signs. It is at this stage that the disease is easiest to overcome. But most do not pay attention to the primary symptoms, and the disease begins to progress.
The patient's intracranial pressure gradually increases, and the growth of pathological tissue increases the impact on the lining of the brain. The second stage of cancer development begins. Changes in tissues have already occurred, but the pathology can still be treated quite successfully. During the second stage of the disease, the patient may experience muscle weakness on one side of the body, sudden dizziness, severe fatigue, loss of sensation in the limbs, and blurred vision (double vision).
However, all these symptoms are similar to those of epilepsy, hypotension and neuropathy. Only by conducting appropriate examinations can an accurate diagnosis and the reason provoking the patient’s state of health be established.
Since each area of the brain is responsible for its own functions, the symptoms of the disease can be focal. Thus, it is possible to determine the location of the pathological neoplasm already at the initial stages:
| Damage area | Focal symptoms |
| Occipital lobe | Visual impairment in one eye, blindness, blurred vision or double vision. |
| Frontal and temporal lobes | Sleep is disturbed, anxiety, depression, aggression occurs, memory deteriorates, consciousness is confused, hallucinations, antisocial behavior, euphoria, and sudden loss of consciousness may appear. |
| Cerebellum | Constant feeling of nausea, vomiting, loss of ability to control the movement of certain parts of the body, muscle weakness. |
| Parietal lobe | Sensory disorders appear. The patient loses the ability to understand speech, is unable to pronounce words clearly, and coordination of movements is impaired. The skills of habitual actions are lost, their sequence is confused. |
| Brain stem | Paresis of the facial nerve occurs, which manifests itself in facial asymmetry, strabismus, tremors in the limbs, difficulty swallowing, hearing loss, staggering when walking, and inability to coordinate movements. |
What can help?
Eat small meals. 6-8 times a day. Portions should be small and food should not be hot.
Do not allow long breaks without food. Always have something on hand to snack on.
Don't eat useless, empty food. Every piece should be beneficial. Choose high-calorie foods rich in protein.
Switch to soft or crushed foods. You can use a blender yourself.
Don’t despair if your favorite dish is no longer tasty, look for alternative options. This is a temporary phenomenon; after treatment, the taste of food will gradually return.
Drink enough fluids.
Monitor your weight: weigh yourself every two days.
Do not drink alcohol, it irritates and additionally dries out the oral mucosa. Alcohol has a general toxic effect on the body.
Every day you need to watch yourself. If there comes a time when the amount of food and liquid consumed has noticeably decreased, and the above tips do not help, there is no need to hide this from your doctor.
In this case, he will prescribe additional specialized nutrition and infusion therapy.
In some situations, the attending physician decides to install a nasogastric tube, and then nutrition occurs through it, and the oral cavity is isolated from contact with food, this makes it possible to maintain the integrity of the mucous membranes in the oral cavity, and there is no trauma to burned tissues. Many patients are afraid and avoid this procedure in every possible way, but, according to reviews from those who have had to deal with this, the probe is a salvation. How, what and in what mode to feed through a tube is taught by a nurse at the hospital where the patient is being treated.
In some situations, patients are advised to form a gastrostomy: when the tumor is widespread in the neck, when it is impossible to eat, when food does not pass through at all. Gastrostomy is most often installed endoscopically, which allows you to avoid trauma and start nutrition in a timely manner.
Causes of brain cancer
The process of tumor formation in the human brain is still poorly understood. There are several main reasons that can lead to the growth of pathological cells in tissues, causing brain cancer:
- Genetic predisposition;
- Radiation exposure;
- Consequence of working in an industry harmful to human health (nuclear industry, formaldehyde, vinyl chloride, acrylonitrile);
- Consequences of hormonal therapy;
- Weak immunity.
Brain cancer is not an infectious disease, so it is impossible to get infected from another person. It is external adverse influences that place the potential victim at risk. Men are most at risk of developing cancer. However, meningiomas are twice as common in women.
Studies have shown that people of color are much less likely to suffer from brain cancer. This is associated with stronger immunity. There is also an age connection - most often brain tumors are found in elderly people over 70 years of age. A large percentage of children aged 8 years are at risk of developing leukemia.
There is an opinion that mobile phones may also be one of the causes of the formation of cancerous tumors in the brain. However, studies have not proven this fact. The same goes for head injuries. Many people constantly live at risk, however, they do not develop tumors. Conversely, people suffer from brain cancer who have almost never been exposed to any of the above unfavorable factors.
Reasons for development
As with cancer cells, the reasons for the development of benign tumors are not fully understood. Predisposing factors are:
- genetic failures in tissues and cells;
- external damaging factors - temperature, radiation;
- exposure to chemicals;
- hypoxia.
However, despite similar risk factors, the mechanism of pathogenesis and growth of benign and malignant tumors is very different, which is the reason for such a large difference in the risk of diseases.
In cancer, tumor growth is invasive, or invading other tissues (spreading). In the case of a benign neoplasm, the growth will be expansive (swollen). If we draw an analogy, in the first case the process is similar to the infection of surrounding tissues by atypical cells, and in the second, it is similar to a local process within the primary tissue.
At the cellular level, malignant tumors have a more atypical structure; the cells are not differentiated and lose their antigens on the membrane. In a benign process, the cells may have a normal appearance, characteristic of the tissue, and grow slowly.
The classification of benign tumors is entirely based on their location - depending on where the tumor is located. Let's look at the most common organs in which tumors can develop.
Stages of brain cancer
Brain cancer is characterized by 4 stages of development. Let's look at each of them:
- First stage. The tumor has already formed, but its size is still small. Symptoms indicating the onset of the disease do not appear or are completely insignificant. At this stage, only the appearance of a headache is possible, which intensifies in the evening. The tissues that surround the tumor are not yet affected.
- Second stage. The brain tumor gradually increases in size and begins to put pressure on neighboring organs. As a result of this exposure, some important body functions are disrupted. It is already possible to identify focal symptoms. At this stage, surgery for a brain tumor is expected. If the cancerous tumor does not exceed 3 cm in size, then it is removed using radiosurgery (Cyber legs and others). This method of treatment is the most gentle and effective for the patient - there is no need to perform craniotomy and additional incisions. To exclude the occurrence of relapse and eliminate the remaining single cancer cells, chemotherapy is carried out.
- Third stage. The brain tumor has already grown quite strongly and metastases have appeared. In addition to focal symptoms, there are also general cerebral symptoms. The growth of cancer cells accelerates. Radical treatment methods are still possible, but achieving a positive effect will be quite difficult.
- Fourth stage (final). A cancerous tumor manifests itself as clearly and aggressively as possible. Metastases are found in the organs most distant from the source of the disease, in bone tissue. Since radical treatment methods did not have a positive effect, it is time to use palliative methods. This means that it is no longer possible to completely eliminate the disease. Therefore, palliative therapy is aimed only at improving the patient’s quality of life, pain relief and relief of painful symptoms, regardless of how long he has left to live.
Benign breast tumors
The most common benign breast tumors are fibrocystic mastopathy and fibroadenoma.
Fibroadenoma looks like a small nodule, which a woman usually feels in her chest. The size usually ranges from 5 millimeters to 2-3 centimeters. The tumor originates from the glandular and connective tissue of the mammary gland. Risk factors for the development of pathology are uncontrolled use of hormonal contraceptives, lack of pregnancy and breastfeeding, late childbirth, smoking, promiscuous sex life.
Fibroadenoma very rarely becomes malignant, with the exception of the leaf-shaped form of the tumor. It is found mainly in young women, up to 25-30 years old.
Fibrocystic mastopathy is characterized by the same symptoms as fibroadenoma, but pathology of the thoracic ducts, cyst formation in them, blockage, and so on can be added. This is fraught with complications - infectious, purulent, and the like.
Fibrocystic mastopathy is classified into a tumor with proliferation and atypia and without such signs. Accordingly, different degrees of danger of the tumor appear. The form with proliferation (cell multiplication) and atypia is essentially a precancer and often degenerates into breast cancer. Therefore, it requires immediate treatment. Mastopathy occurs mainly in middle-aged and elderly women (either 40-50 years old, or 65 and older).
Diagnosis of brain cancer
Cancerous tumors respond well to treatment if the diagnosis was made quickly, efficiently and in the early stages of the disease. Modern medicine uses a wide range of methods for diagnosing brain cancer, among which the most popular are the following:
- X-ray examinations, computed tomography (CT) with contrast, magnetic resonance imaging (MRI), positron emission tomography (PET), electroencephalography;
- Ultrasound (US), microwave depth radiometry;
- biopsy and cerebrospinal fluid analysis, laboratory diagnostics, medical history, genetic studies;
- histological, cytological and immunohistochemical studies;
- endoscopy, use of tumor markers.
Statistics say that every year in Russia alone more than 30,000 cases of brain cancer are detected. It is important to understand that the first signs of this disease are completely harmless. Many people prefer to deal with headaches, fatigue and depression on their own, or do not take into account the increasing symptoms at all. However, you should not neglect your health. In order not to miss the onset of the disease, it is recommended to do an MRI and undergo proper examination.
Treatment and removal of brain cancer
To treat brain cancer, radical therapy is mainly used - surgery. If the diagnosis was carried out on time and efficiently, then removal of brain cancer is successful in most cases. Relapses occur in rare cases. If metastasis growth is detected, repeat surgery is possible.
During surgical treatment, a laser and other special instruments are used. Cryocoagulation has shown the greatest effectiveness in the treatment of benign neoplasms on bone and soft tissues. During the procedure, the tumor is exposed to liquid nitrogen, argon or helium. Low temperatures instantly destroy cancer cells. The advantage of this treatment is the absence of side effects such as vomiting and nausea.
If the tumor is small, hormone replacement therapy is prescribed. This treatment of a brain tumor does not entail disruption of the patient’s hormonal levels and is quite easily tolerated. This method has proven itself to be especially effective in the treatment of pituitary adenomas. The drugs used during therapy are aimed at stabilizing the level of prolactin in the patient's body, which leads to a decrease in tumor size.
Many severe cases of brain disease require a comprehensive approach. However, it is not always possible to undergo surgery. It all depends on what part of the brain the tumor occurs in. In this case, the removal of the cancerous tumor is carried out using modern ultrasound and laser methods.
Chemotherapy is indicated to reduce the size of the tumor. It can also be used to stop the growth of metastases. Taking into account the severity of the disease, stage of development and general condition of the patient, an individual course of treatment is drawn up.
Conservative (palliative) therapy is of an auxiliary nature. The goal of this method is to alleviate the patient’s general condition as much as possible. The patient is prescribed a course of pain medication (narcotic analgesics), antiemetics, sedatives and anti-inflammatory drugs, and glucocorticosteroids.
Meningioma
Meningiomas are predominantly benign neoplasms, accounting for approximately 20% of all primary brain tumors in men and up to 38% in women. The peak incidence is observed at the age of 55-64 years.
Typically, meningiomas are slow-growing, well-circumscribed tumors with a round shape. The starting point of growth is the mesodermal cells of the arachnoid membrane of the brain, located at the top of the so-called. pachyonic granulations, therefore most often meningiomas are located on the convexital and basal surface of the brain, in the interhemispheric fissure, along the tentorium of the cerebellum. However, there are also intraventricular and even intracerebral variants of meningiomas, the initial source of growth of which is perivascular arachnoid cells.
The loss of genetic material from the long arm of chromosome 22 is critical for the initial development of meningioma.
The most common is the 2010 World Health Organization classification, which divides meningiomas into three main groups: benign, atypical and malignant (anaplastic), based on the number of mitoses as the main difference between atypical and anaplastic forms.
Up to 60-70% of meningiomas develop along the falx (including parasagittal), along the sphenoid bone (tubercle, platform, inclined processes, greater and lesser wings), above the convexital surface of the cerebral hemispheres. Other localizations include the posterior surface of the pyramid of the temporal bone, Blumenbach's clivus, tentorium cerebellum and others. It should be noted that as they grow, meningiomas can involve several neighboring anatomical regions at once, for example, in the sphenopetroclival region: the wing of the sphenoid bone and the cavernous sinus (middle cranial fossa), the apex of the pyramid, the anterior parts of the cerebellopontine angle and the Blumenbach clivus (posterior cranial fossa) . In approximately 8% of cases, meningiomas can be multiple in nature (meningotheliomatosis), both as part of hereditary diseases (neurofibromatosis) and sporadically
DIAGNOSIS OF MENINGIOMA
PREREQUISITES FOR THE APPLICATION OF STEREOTAXIC RADIOSURGICAL IN THE TREATMENT OF INTRACRANIAL MENINGIOMA
Today, surgical removal of these tumors is the main method of treatment in the case of large and giant tumors that occur with signs of compression of the brain, visual pathways, brainstem, in the presence of clear cerebral and focal symptoms of damage to the cerebral hemispheres, brainstem, and cerebellum. To assess the degree of radicality of tumor removal, Simpson proposed a 5-point scale
In fact, complete removal of the tumor is only 1-2 degrees of radicality. Logically, only in this case can we expect no recurrence of the tumor in the future. In other cases, one or another volume of viable tumor tissue obviously remains, which will certainly increase further. However, as practice shows, the rate of recurrence of meningiomas, even with radical removal of Simpson I, during the first 5 years is about 8%, increasing over the next 5-10 years to 25%. With less radical removals (Simpson II and higher), the probability of tumor recurrence may exceed 50%
The probability of relapse depends not only on the time after surgery, but also on the degree of malignancy of the tumor, amounting to 38 and 78% for atypical and anaplastic variants, respectively
Relevant is the relatively high level of functional disorders associated with the removal of tumors located in functionally rich and hard-to-reach areas: the superior sagittal and cavernous sinuses, Blumenbach's clivus, cerebellar-pontine angle and other intracranial locations.
Difficulties in removal and a high level of functional complications traditionally dictate wait-and-see tactics for neurosurgeons, the so-called. “wait & see”, the meaning of which is to dynamically monitor the tumor and make a decision about surgery in a situation where the further development of the tumor begins to cause neurological symptoms and affects the patient’s quality of life.
However, as in the case of other tumors, the possible consequences of this tactic should be clearly understood, of which the patient must be fully informed in advance.
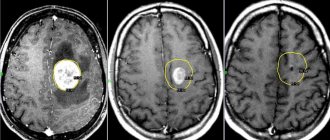
Below is an example of a patient who was observed in one of the leading neurosurgical institutions in the Russian Federation for 8 years. It is initially obvious that the tumor cannot be radically removed without the risk of severe neurological deficit, due to its inaccessible location and proximity to the vascular and neural structures of the base of the brain. During observation, the tumor grew significantly. And if at the beginning it was possible to stop the growth of the tumor with just one session of stereotactic radiosurgery, then after 8 years a course of radiation therapy of 30 sessions over 1.5 months was needed
Rice. 1. Small meningioma of the petroclival area, without brainstem compression at the time of initial diagnosis. No visual disturbances
Rice. 2. After 2 years, there is a clear growth of the tumor with initial signs of impact on the brain stem and intimate adherence to the left optic tract. No visual disturbances
Rice. 3. After 6 years. Multiple increases in tumor size with severe compression of the brainstem and involvement of the visual pathways in the tumor over a large area. Severe visual impairment
In this regard, alternative techniques for influencing the tumor are relevant, among which a special place is occupied by stereotactic radiosurgery using the Gamma Knife device (SRGN), as the most proven method, with long-term treatment results studied in large cohorts of patients over a long period of time. The main advantages of using SRCHN are its non-invasiveness, the ability to target surgically difficult-to-reach and multiple tumors, and high efficiency.
Diagram 1. Correlation of various types of extracerebral intracranial tumors in radiosurgical practice
According to the results of a European multicenter study (2012), which combined data on the results of SRCHN of meningiomas in 4565 patients with a follow-up period of at least 24 months (median follow-up 63 months), a decrease in tumor size was noted in 58% and stabilization in size in 34.5%. Thus, control of tumor growth was noted in 92.5%. Progression was detected in 7.5% (281 tumors) with a median of 48.7 months. Of these, 197 tumors did not require additional treatment at the time of last follow-up. Kaplan-Meier disease-free survival estimates at 5, 7.5, and 10 years were 95.2%, 91.3%, and 88.5%, respectively. Control MRI data were significantly better in women than in men (P < 0.001) and in those patients who had not previously been operated on for this tumor. Patients with single meningiomas had significantly better treatment results than those with multiple formations (P<0.001), and basal tumors were better controlled than convexital tumors. Clinical improvement was noted in 53.5% of patients, incl. in 22.2% - complete regression of symptoms. Complications occurred in 12.9%, and in half of them (6.3%) they were temporary. Mild or intermittent disturbances after SRCHN were observed in 4.7%, persistent, but not affecting the quality of daily life - in 6.8%, and only in 1.3% were severe or constant. Thus, the authors summarize, SRCHN is a safe and effective method for the treatment of benign meningiomas even in the mid- and long-term follow-up period
Rice. 4. Meningioma of the sphenopetroclival area on the right. Reduction in tumor volume by 40% over 7 years of follow-up after SRCHN
Rice. 5. Meningioma of the left cerebellopontine angle. Reduction in tumor volume by 64% over 6 years of follow-up after SRCHN
Rice. 6. Meningioma of the parietal-parasagittal region on the right. Reduction in tumor volume by 69% over 7 years of follow-up after SRCHN
Radiosurgery of intracranial meningiomas has a huge number of features depending on the specific anatomical location, tumor size, its histological structure, proximity to functional vascular and neural structures of the brain. The format of the website does not allow us to cover this fully. I will only dwell on the question of the advisability of performing SRCHN of those meningiomas that are asymptomatic.
In some cases, meningiomas are an incidental finding during a routine CT/MRI examination and do not have focal symptomatic manifestations, or general cerebral symptoms (for example, headaches) cannot be reliably explained only by the presence of a tumor. To date, there is no clear opinion regarding the advisability of SRCHN of asymptomatic meningiomas. Proponents of conservative treatment (essentially observation over time) base their position on literature data that up to 2/3 of incidentally detected meningiomas do not grow during further observation. This conclusion was made based on linear-metric analysis of CT and MRI data from 303 meningiomas. It is noted that a hypointense signal from a tumor in T2WI on MRI or a hyperdense signal on CT, corresponding calcifications, as well as the elderly (over 60 years) age of patients are prognostic factors for slow growth or its absence. At the same time, a hyperintense signal in T2WI is characteristic of more actively growing tumors. It should be noted that all of these studies were carried out on the basis of an analysis of CT and MRI data obtained in the 90s of the twentieth century and were based on assessing changes in the linear sizes of tumors. Growth of the formation was considered to be an increase in at least one linear dimension by at least 2 mm. However, the most objective assessment of dynamic changes is provided by measuring tumor volume. For this purpose, mathematical processing of MRI or SCT data in DICOM format is used using specialized software. For clarity, we can give a simple example: the volume of a ball with a diameter of 10 mm is 4.19 cc, while an increase in diameter by just 1 mm will increase the volume to 4.85 cc (16%), and by 2 mm - up to 5.58 cc (33%). Thus, visual and even linear-metric assessment of the dynamics of tumor development has significant subjectivity and error and cannot be considered as reliable confirmation of the absence of continued growth. Oya et al. (2011) published data on dynamic observation of patients with meningiomas of various intracranial localization using linear and volumetric control. The mean follow-up period in this subgroup was 3.6 years. An increase in the linear size of tumors was noted in 44% (120 of 273 tumors), while an increase in tumor volume was observed in 74.0% (114 of 154) of cases. Factors associated with the highest annual growth rates were male gender (p = 0.0002), initial diameter greater than 25 mm (p < 0.0001), symptomatic course (p = 0.037), tumor signal hyperintensity on T2- weighted MRI (p = 0.0001), and the presence of peritumoral edema (p < 0.0001). Jo KW et al. compared the advantages and disadvantages of preventive irradiation of asymptomatic meningiomas and their conservative management. 5-year progression-free survival in the first group (after SRCHN) was 100%, while in the second only 61.7%. Salvetti et al (2012) analyzed the results of SRCHN of forty-two patients with asymptomatic solitary meningiomas. The most common tumor location was convex (23.8%), and the mean volume was 4.0 cc. They found that actuarial tumor growth control rates were 100%, 95.7%, and 95.7% over 2. 5 and 10 years, respectively. Actuarial symptom control at 5 and 10 years was 97% and 93.1%, respectively. Overall progression-free survival was 91.1% and 77.8% at 5 and 10 years, respectively. Based on these data, the researchers concluded that patients with asymptomatic meningiomas benefit from prophylactic radiosurgery at the asymptomatic stage compared with patients who did not receive any treatment. In addition, SRCHN as a treatment option has an overall low risk of complications and morbidity.
Summarizing the above, we can safely say that the use of Gamma Knife in the treatment of intracranial meningiomas is a highly effective and fairly safe treatment method. Indications and contraindications for radiosurgery should be determined by a specialist who has both theoretical and practical training in neurosurgery and radiology.
Prognosis for brain cancer
Diagnosis that was carried out in a timely and correct manner significantly increases the chances of survival. But it is also worth considering other important factors - the patient’s age, the size of the tumor and its nature, the location of the tumor, the stage of development.
In the early stages of development, brain cancer is treated quickly and successfully. With a correctly designed treatment regimen and timely surgical intervention, patient survival is about 80% over the next five years. If the patient seeks help at the last stage of tumor development, and surgical intervention is no longer possible, then the chances of survival are significantly reduced - up to 40%. Medical statistics show that comprehensive treatment started in the early stages of brain cancer can save more than 60% of lives.
It is important to consider the types of cancer tumors. Some of them are so aggressive that no more than 5% of patients have a chance of survival. Thus, when a brain glioma is detected, the prognosis remains unfavorable even with timely treatment and is independent of the patient’s age. The maximum five-year survival rate for patients with this type of brain cancer remains between 10-19%.
The location of the malignancy plays an important role. If the tumor was completely removed, then the chances of recovery immediately increase to 50%. If the localization of the tumor is such that it is impossible to carry out any method of therapy, then the patient will not survive.
The occurrence of relapses after treatment is also a negative indicator and significantly reduces the chances of survival. In such cases, the doctor is obliged to soberly assess the situation and make a decision in favor of repeated intensive or initiation of palliative therapy. In some cases, it makes sense not to torture the patient, but to help him live the rest of his life better.
Types of benign skin tumors
New growths on the skin do not necessarily originate from epidermal or dermal cells. Most often this is the growth of adipose, vascular tissue or sebaceous gland. Let's look at these types of tumors in more detail.
Lipoma
Lipoma is a benign tumor of adipose tissue. It is visually localized on the skin, but is located in the subcutaneous fatty tissue. Usually it reaches several centimeters in diameter and growth stops, however, there are known cases of the development of huge lipomas, which significantly reduce the patient’s quality of life. It very rarely becomes malignant, but it is better to remove it even for aesthetic reasons.
Atheroma
A benign tumor that develops due to blockage of the sebaceous gland. Localized on the skin, usually in places rich in sebaceous and sweat glands - armpits, head, back. It does not become malignant, but can fester. The size of the atheroma is on average from a centimeter to 5.
Papilloma
A benign tumor that develops from skin epithelial cells. It is purely viral in nature and is caused by HPV (human papillomavirus). Papilloma usually ranges in size from a few millimeters to 0.5 cm, and is white, flesh-colored, or discolored. The surface may be uneven.
Pigmented nevus
The neoplasm originates from pigment cells - melanocytes. People call them moles or warts. Nevus is dangerous because it can become malignant and turn into melanoma - an extremely dangerous and aggressive oncological disease.
Keratoma
Just like papilloma, it comes from the epithelium, but has a different nature; here the epithelial cells become keratinized and grow. The causes of development are exposure to external aggressive factors on the skin - temperature, chemical burns, and so on. May develop into skin cancer.
Fibroma
A benign tumor arising from the growth of connective tissue under the skin. It mainly occurs due to skin trauma or insect bites. It looks like a dense nodule under the skin, ranging in size from 1 millimeter to half a centimeter.
Structuring diseases
- Intracerebral tumors Primary Gliomas Astrocytoma Diffuse
- Pilloid astrostoma
- Anaplastic astrocytoma
- Fibrillary astrocytoma
- Glioblastoma
- Ependymoma
- Meningioma
- Pituitary adenoma
- Arnold-Chiari malformation