Ulnar nerve neuritis is often accompanied by numbness and paralysis of the affected limb. This is due to a violation of the innervation of skeletal muscles in the forearm, hand and some fingers.
In the absence of timely treatment, muscle tissue atrophy and irreversible changes in the structure of the ulnar nerve are possible. The latter leads to complete loss of sensitivity and various motor activity disorders without the possibility of recovery.
What is the ICD-10 code?
Ulnar nerve neuritis is an inflammation of various etiologies affecting the myelin sheath and axial cylinders of the nerve fiber.
The pathology is accompanied by acute pain, loss of sensitivity and decreased motor activity of the affected arm.
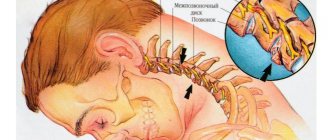
Disruption of innervation gradually leads to atrophy of the surrounding muscles of the forearm and hand. The nerve is most often damaged in the area of the ulnar groove : at the entrance and exit from the cubital canal.
In the ICD-10 classification, inflammation of the ulnar nerve is not classified as a separate niche. Therefore, such neuritis has code G56.2.
ICD neuralgia (ICD-10)
It is known that the ICD (International Classification of Diseases) is the main document for processing statistical data in all healthcare institutions; diseases are classified by different codes. In the Russian Federation, the transition to the modern ICD, tenth revision (ICD-10) occurred in 1999, and outpatient, inpatient and statistical institutions of the Ministry of Health still work with this document, namely ICD-10. Each patient who is diagnosed in a clinic or in a hospital, who has an outpatient card or medical history, has an encrypted diagnosis, preliminary or final according to ICD-10, this also applies to neuralgia.
Neuralgia in ICD-10
Neuralgia is presented in ICD-10 in two classes (codes): G (diseases of the nervous system, class 6) and M (diseases of the musculoskeletal system and connective tissue, class 13). This division is justified, since very often the cause of neuralgia is large muscles that cause compression or compression of one or another nerve. This situation may be accompanied by myofascial muscular-tonic syndrome.
“Pure” neuralgia, in which muscles and compression with their help have no role, are described in class G. An example is trigeminal neuralgia.
Examples of class G neuralgia:
- 1Lesions of the glossopharyngeal nerve;
- Trigeminal neuralgia;
- 1 Atypical facial pain;
- 0*Neuralgia after herpes zoster.
Examples of class M neuralgia:
- 1 Radiculopathy (this includes brachial, lumbar, lumbosacral and thoracic variants);
- 2 Cervicalgia;
- 3 Sciatica;
- 4 Lumbago with sciatica.
This is where certain options, precisely determined using the ICD, end. Since reality is much more complex and unpredictable than any precise diagnosis, the international classification of diseases provides loopholes for the free formation of a diagnosis. So, you can use the following encoding:
M79.2 Neuralgia and neuritis, unspecified
This diagnosis can be made, for example, due to lack of time. It is known that in hospitals, MES, or medical and economic standards, “rule the show.” In the event that a patient has been “over-lying” without reason, the department’s internal expert points out the shortcomings, and an external examination or unscheduled inspection may assign penalty points, which will affect funding.
Therefore, in extreme cases, you can be discharged with this diagnosis, and clarification can be done on an outpatient basis.
Another heading, which is sometimes interpreted in an extremely broad way, is the following:
R52 Pain not elsewhere classified. This refers to pain that cannot be attributed either to the mammary gland, ear, pelvis, spine or any other part of the body. For example, “wandering pain.”
Pain not elsewhere classified (R52)
As you can see, it belongs to class R. It is referred to as “Symptoms, signs and abnormalities identified by clinical and laboratory tests, not classified elsewhere.”
How to correctly decipher the diagnosis
This allows the doctor to “get out”, but such encryption may cause dissatisfaction with the hospital administration for the reason that this class is non-core. In other words, this diagnosis says: “we found something, but what we found does not fit into anything.”
In fact, there should be no non-core diagnoses in the department: three days are given to establish a diagnosis, when it changes from a “diagnosis upon admission” to a working one. If it turns out that the patient is a “stranger,” he must be transferred or discharged. If he spent time in the department with a non-core diagnosis and was discharged, then this is a sign of incompetent management of the department.
Therefore, the correct use of ICD-10 in coding certain types of neuralgia can not only help process large amounts of statistical data, but also save significant funds for a medical institution.
Causes
The most common cause of a neurological disorder is elbow injury . Neuritis of this etiology occurs in 28-34% of patients.
Prolonged bed rest with squeezing the arm between the body and the bed, puncture and cutting wounds, fractures and dislocations can lead to damage to the cubital canal.
In this case, there is a malnutrition and gradual destruction of the nerve fiber, accompanied by acute inflammation. In such a situation, the pathological process becomes chronic.
In some cases, neuritis manifests itself decades after the injury . This is due to the gradual progression of ligament fibrosis. Another name for the pathology is Miche's ulnar neuropathy.
Other causes of neuritis include:
- prolonged hypothermia;
- infectious lesions: diphtheria, typhoid fever, herpes virus, measles and brucellosis;
- vascular pathologies, ischemia in the elbow joint, in which the nerve stops receiving the required amount of oxygen and nutrients;
- alcohol poisoning, intoxication with heavy metal salts;
- epicondylitis, periarthrosis of the head of the humerus;
- diseases of the endocrine system: diabetes mellitus, thyroid disorders;
- compression of nerve tissue during sleep, with a sudden change in hand position;
- cervical osteochondrosis, herniated intervertebral discs: lead to compression of the vessels supplying the ulnar nerve.
In children, ulnar nerve neuritis often appears in the absence of timely vaccination against measles and typhus . The cause of the disease can be hypovitaminosis, congenital pathologies of the cubital canal.
In the latter case, there is compression of the nerve in the ulnar groove by a fibrous arch stretched between the heads of the flexor carpi.
Development of the disease due to work characteristics
Neuritis, which occurs due to pinching of the ulnar nerve, develops in office workers, operators or people in industrial production. The costs of the profession force people to often rest their elbows on the table, armrests or machines.
The disease can occur with prolonged overexertion of the arms in patients whose activities involve heavy physical labor. Over time, mechanical stress leads to injury, which causes neuritis.
Ulnar nerve neuropathy treatment
Treatment should be comprehensive, that is, use all available methods. It is necessary to perform exercises for the hands, and here the patient must be motivated to recover. First of all, provoking factors are identified and removed. These may be inconvenient tools for work, some habits.
If neuropathy is caused by a common medical condition, treat it aggressively. A special orthosis, elastic bandages and other orthopedic devices are put on the wrist.
Important: maintain a work-rest schedule, spend more time in the fresh air, eat vegetables and fruits, and foods containing calcium.
Drug therapy
In mild cases, non-steroidal anti-inflammatory drugs (aspirin, diclofenac) are prescribed. If the cause of compression may be edema, then diuretics (Lasix, etc.). Novocaine, analgin, and glucocorticosteroids are injected into the affected area (elbow or wrist). The dosage depends on the patient’s age, severity of the disease, and concomitant diseases. It is advisable to rub pain-relieving ointments and gels onto the area of nerve damage.
Vitamins
Help restore immunity.
Strengthen metabolism in the nerve, eliminate ischemia, expand capillaries. Used: Vitamins B1, B6, as well as complex preparations: Milgamma. They are prescribed intramuscularly, or you can inject directly into the area of compression or injury to the ulnar nerve. It will be useful to take multivitamin complexes internally.
Clinical picture: symptoms and manifestations
The intensity of symptoms depends on the degree of damage to the ulnar nerve and the individual characteristics of the patient. Peripheral nerve fibers consist of sensory, autonomic and motor neurons.
When each of them is damaged, the following clinical picture is observed:
- With neuritis, changes in tactile perception are observed in the area of the hand and fingers. Sensory neurons of the ulnar nerve do not innervate the skin of the forearm.
Numbness may develop, which is accompanied by a decrease or complete loss of sensitivity in the affected area.In some cases, paresthesia appears. When they occur, the patient feels tingling and frequent goosebumps.
- Impaired motor activity is accompanied by the appearance of paralysis or paresis.
The pathological process can cover the area from the elbow joint to the fingertips. There is muscle weakness in the skeletal muscles innervated by the ulnar nerve. If left untreated, atrophy and loss of tendon reflexes may develop. Due to lack of physical activity, the muscles decrease in size, so the affected forearm appears thinner when compared to the healthy arm. - Autonomic disorders are accompanied by trophic changes. The limb swells, blueness of the skin and depigmentation are observed. Hair falls out on the arm and sweating increases. Nails often break and trophic ulcers appear.
- When the ulnar nerve is pinched in the musculoskeletal canal, tunnel syndrome occurs.
The pathology is accompanied by pain . As the disease progresses, it leads to numbness of half the ring finger and little finger on the palmar side.
On the back of the hand, there is a loss of sensitivity in half of the middle finger and a complete loss of tactile perception in the ring and little fingers.
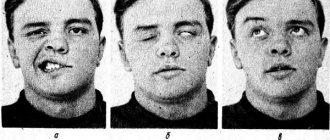
Numbness of the fingers is accompanied by muscle weakness, muscle wasting and atrophy. The brush resembles a bird's paw .
Possible patient complaints
Patients come with complaints of periodic numbness of the arm in areas innervated by the ulnar nerve. Loss of sensitivity is observed in the IV, V, half of the third finger on the back of the hand, the skin on the palms .
Numbness can be complete or partial depending on the severity of the pathological process. People report that after sensation is restored, there is tingling, burning, or cramping in the affected area.
Pain appears on the outside of the elbow joint . The pain syndrome often radiates to the thumb, ring finger, and little finger. The pain may spread to the shoulder area, the first third of the forearm.
Due to muscle weakness, patients cannot clench their hand into a fist. They often lose the ability to coordinate the movements of the affected arm. In severe cases of the pathological process, paralysis is observed .
How other types of neuritis of the extremities manifest themselves:
- brachial and median nerves;
- sciatic nerve;
- femoral, tibial and fibular.
What symptoms most often occur with ulnar nerve neuritis?
Sensitivity disorders due to neuritis are manifested by numbness in the area of the little and ring fingers, and the inner surface of the hand. At the same time, unpleasant sensations appear in these places: tingling, a feeling as if “goosebumps are crawling” on the skin. Pain in the hand may be bothersome.
Among the movement disorders, weakness is noted in the muscles that spread in different directions and bring the fingers together. The main phalanges (those that connect directly to the hand) of the fingers are extended (since another nerve, the radial one, is responsible for their extension), and the distal ones are bent. As a result, the hand acquires a characteristic appearance - doctors call it a “clawed paw” in their jargon. Gradually, the small muscles of the hand decrease in size and atrophy.
Autonomic disorders with ulnar nerve neuritis manifest themselves in the form of symptoms such as dryness or increased moisture of the skin, cyanosis, and coldness.
Diagnostic methods
Diagnosis and determination of further treatment regimen is carried out by a neurologist. The specialist collects anamnesis and records the patient’s main complaints in the medical history. After this, the neurologist conducts a visual examination.
With ulnar nerve neuritis, the hand takes on the appearance of a bird's paw: the third and fourth fingers are bent, the little finger is moved to the side. The doctor notes cyanosis, hair loss, brittle nails, and weight loss in the affected limb.
After the examination, the neurologist conducts a series of neurological tests to determine muscle strength, degree of numbness and loss of reflexes and makes a preliminary diagnosis.
To confirm the initial conclusion, the specialist prescribes laboratory and instrumental examinations , which allow us to find out the cause of neuritis:
- General and biochemical blood test . Necessary for identifying pathogenic agents of infectious diseases, the presence of produced antibodies and leukocytes.
- X-ray using contrast .
Allows you to assess the condition of the vessels supplying the ulnar nerve. X-rays also make it possible to take into account the anatomical features of the elbow joint and cubital canal, and to identify the degree of damage to the musculoskeletal tunnel in the event of injury. - Ultrasound and MRI . Ultrasound and magnetic resonance imaging help assess the condition of blood vessels, soft tissues and bone structure in case of fractures, pinched nerves and other injuries.
- Electroneuromyography . The procedure helps determine the extent of damage to the skeletal muscles.
Special diagnostic criteria for determining the disease
Neurological tests to make a preliminary diagnosis of ulnar neuritis often include the following:
- Pitre's test. To carry it out, the patient must place his palm on the table and try to spread and close his fingers. With neuritis, the patient cannot bring the ring finger and little finger to the midline.
- Afterwards, the doctor asks the patient to try to scratch the surface of the table with his little finger. Due to inflammation of the nervous tissue, he is unable to do this.
- With neuritis, the patient cannot clench his hand into a fist, or hold a sheet of paper with two fingers. When you clench your hand into a fist, the middle, ring and little fingers do not bend.
- If the patient presses the hand firmly to the table, the little finger moves to the side. In this position, the patient cannot make horizontal movements of the third, fourth, fifth finger.
What diseases should be distinguished from?
After recording the patient's complaints in the medical history, differential diagnosis with radial nerve neuritis is carried out . In contrast to damage to the ulnar nerve, in this situation the hand hangs down and a strong muscle spasm is observed.
If the radial nerve is damaged, the patient cannot straighten the hand independently; the thumb is reduced to the index finger. The sensitivity of the 1st, 2nd, and 3rd fingers of the affected limb is impaired.
It is difficult to distinguish ulnar nerve neuritis from damage to the C8 nerve root in the neck due to radiculopathy . With radicular syndrome, numbness is observed on the ulnar surface of the forearm, which is not typical for neuritis. With inflammation of the ulnar nerve, only numbness of the hand is observed.
When conducting a differential diagnosis, the neurologist pays attention to the presence of a specific symptom of ulnar nerve neuritis - numbness of the radial surface of the ring finger.
When the nerve roots of the spine, spinal cord, or plexus are affected, there is a loss of sensation in the entire finger.
ICD neuralgia (ICD-10)
It is known that the ICD (International Classification of Diseases) is the main document for processing statistical data in all healthcare institutions; diseases are classified by different codes. In the Russian Federation, the transition to the modern ICD, tenth revision (ICD-10) occurred in 1999, and outpatient, inpatient and statistical institutions of the Ministry of Health still work with this document, namely ICD-10. Each patient who is diagnosed in a clinic or in a hospital, who has an outpatient card or medical history, has an encrypted diagnosis, preliminary or final according to ICD-10, this also applies to neuralgia.
Neuralgia in ICD-10
Neuralgia is presented in ICD-10 in two classes (codes): G (diseases of the nervous system, class 6) and M (diseases of the musculoskeletal system and connective tissue, class 13). This division is justified, since very often the cause of neuralgia is large muscles that cause compression or compression of one or another nerve. This situation may be accompanied by myofascial muscular-tonic syndrome.
“Pure” neuralgia, in which muscles and compression with their help have no role, are described in class G. An example is trigeminal neuralgia.
Examples of class G neuralgia:
- 1Lesions of the glossopharyngeal nerve;
- Trigeminal neuralgia;
- 1 Atypical facial pain;
- 0*Neuralgia after herpes zoster.
Examples of class M neuralgia:
- 1 Radiculopathy (this includes brachial, lumbar, lumbosacral and thoracic variants);
- 2 Cervicalgia;
- 3 Sciatica;
- 4 Lumbago with sciatica.
This is where certain options, precisely determined using the ICD, end. Since reality is much more complex and unpredictable than any precise diagnosis, the international classification of diseases provides loopholes for the free formation of a diagnosis. So, you can use the following encoding:
M79.2 Neuralgia and neuritis, unspecified
This diagnosis can be made, for example, due to lack of time. It is known that in hospitals, MES, or medical and economic standards, “rule the show.” In the event that a patient has been “over-lying” without reason, the department’s internal expert points out the shortcomings, and an external examination or unscheduled inspection may assign penalty points, which will affect funding.
Therefore, in extreme cases, you can be discharged with this diagnosis, and clarification can be done on an outpatient basis.
Another heading, which is sometimes interpreted in an extremely broad way, is the following:
R52 Pain not elsewhere classified. This refers to pain that cannot be attributed either to the mammary gland, ear, pelvis, spine or any other part of the body. For example, “wandering pain.”
Pain not elsewhere classified (R52)
As you can see, it belongs to class R. It is referred to as “Symptoms, signs and abnormalities identified by clinical and laboratory tests, not classified elsewhere.”
How to correctly decipher the diagnosis
This allows the doctor to “get out”, but such encryption may cause dissatisfaction with the hospital administration for the reason that this class is non-core. In other words, this diagnosis says: “we found something, but what we found does not fit into anything.”
In fact, there should be no non-core diagnoses in the department: three days are given to establish a diagnosis, when it changes from a “diagnosis upon admission” to a working one. If it turns out that the patient is a “stranger,” he must be transferred or discharged. If he spent time in the department with a non-core diagnosis and was discharged, then this is a sign of incompetent management of the department.
Therefore, the correct use of ICD-10 in coding certain types of neuralgia can not only help process large amounts of statistical data, but also save significant funds for a medical institution.
Features of treatment
Treatment begins with fixation of the hand and forearm in a plaster splint , thanks to which the elbow joint remains at rest.
The hand is in a half-bent state. The patient should suspend the limb using a scarf or bandage.
When developing a treatment regimen, the neurologist focuses on eliminating the cause of the neurological disorder. For this purpose , drug therapy is carried out, physical therapy and massage are prescribed .
In case of infection, after identifying a pathogenic pathogen, the doctor prescribes antiviral drugs or antibiotics. If blood circulation is impaired, the patient is prescribed a vasodilator to restore trophism of the nervous tissue. It allows you to eliminate the consequences of ischemia.
To eliminate swelling of the ulnar nerve, the patient should take potassium-sparing diuretics and NSAIDs.
For pain relief in high intensity pain syndrome, the use of analgesics is indicated. B vitamins help speed up the recovery of nervous tissue.
After 2 weeks from the start of drug therapy, complex treatment is supplemented with physiotherapy:
- ultraphonophoresis;
- electrophoresis with the introduction of analgesics and biogenic stimulants;
- UHF therapy;
- magnetic therapy;
- electrical stimulation for muscle tissue damage;
- acupuncture.
Massage technique
Massage helps relieve pain, accelerate nerve fiber regeneration , and restore original sensitivity and motor activity. The patient must undergo a course of 15-20 procedures.
Massaging begins with the cervical and thoracic spine. This is necessary to ensure blood flow to the affected limb.
Afterwards, a preliminary massage of the sore arm is carried out using the following techniques:
- tong-like rubbing;
- kneading stiff muscles;
- stroking.
After this, the specialist massages the skeletal muscles innervated by the ulnar nerve . To do this, he uses muscle kneading, vibration, rubbing with his fingers, and pressing with the pad of his thumb. The total duration of the procedure is about 10-15 minutes.
Massaging the ulnar nerve is carried out in the area between the process of the ulna and the medial epicondyle of the head of the humerus. To gain access to the lesion, the arm is slightly bent at the elbow.
Exercise therapy
Physical activity is introduced into the treatment program 48 hours after the splint is applied . Physical therapy consists of the following exercises:
- It is necessary to bend your arm at the elbow and lean on the table so that your forearm is perpendicular to its surface. After this, you need to bend your index finger down, then raise your thumb up. Movements should be alternated.
- The arm bent at the elbow joint should be placed on the table top. Then you need to bend the second finger down, lift the third up. With the other hand, you should alternately bend and straighten the remaining fingers in the middle and main phalanx.
Exercises are repeated at least 10-15 times . To increase the effectiveness of therapeutic exercises, it is recommended to lower the sore hand into a basin of warm water.
Therapy for post-traumatic joint inflammation
Treatment of neuritis resulting from injury is carried out depending on the nature of the injury. Penetrating wounds are sutured and treated with medications and physical procedures .
If neuritis appears due to compression in the cubital canal with the subsequent occurrence of tunnel syndrome, the patient is prescribed local administration of drugs.
Painkillers and hormonal medications necessary to relieve pain, soft tissue swelling and reduce the activity of the inflammatory process are injected into the musculoskeletal canal .
In case of severe compression of the nerve, which usually occurs with fractures and dislocations, surgery is prescribed. Surgery is performed for the purpose of decompression .
Patients with destructive changes in the ulnar nerve resulting from prolonged inflammation may be referred for surgery. In such a situation, the damaged nerve fiber is sutured and repaired.
Coding of intercostal neuralgia in ICD 10
Acute pain in the chest or sides of the body occurs in most cases due to pinched nerve endings located in the thoracic spine.
This pathology has a specific code for intercostal neuralgia according to ICD 10 and looks like M79.2, which causes the following etiotropic factors:
- muscle spasm due to intense physical activity or overwork;
- lack of B vitamins;
- violation of metabolic processes;
- the presence of osteochondrosis is considered the most common cause of nerve inflammation in the thoracic or cervical region;
- Much less often, intercostal neuralgia is provoked by a problem in the lumbar region, that is, radiculitis;
- stress and post-traumatic consequences;
- influence of an external factor (draft, cold).
Typically, intercostal neuralgia occurs in middle-aged and older people.
Symptoms of neuralgia
In ICD 10, intercostal neuralgia has code M79.2 and is differentiated with a diagnosis of acute coronary syndrome, a type of coronary heart disease.
The patient’s subjective complaints are indeed similar to cardiovascular pathology. The most common symptoms are:
- cutting, dull, aching or sharp pain appearing in the chest area, sometimes with a projection to the shoulder blades;
- a sudden movement, for example, a deep breath, sneezing, coughing or turning, greatly increases the pain;
- at the site of a pinched nerve, swelling, redness and numbness may be observed;
- often there is point pain, that is, pain when pressing with fingers, which is not observed when diagnosing myocardial infarction.
During attacks of angina pectoris (I20 according to ICD 10) or in the case of acute myocardial infarction (I21), the pain does not intensify after changing body position or taking a deep breath. Relief occurs after taking nitroglycerin, which is one of the main signs of cardiac pathology.
The most important criterion for an unspecified diagnosis is an electrocardiogram, according to which an experienced doctor will accurately determine the origin of the pain syndrome. The picture of acute coronary syndrome on the cardiogram is pronounced, but pinched nerves with severe tissue swelling can also cause changes on the ECG due to intense pain and conduction disturbances. Usually, a neurologist deals with neuropathy, but in this case, consultation with a cardiologist or resuscitator is essential to avoid making a fatal mistake.
Therapeutic measures
Intercostal neuralgia has a specific code in the International Classification of Diseases, 10th revision, which determines the availability of unified protocols for patient management and recommendations for adequate and effective treatment.
Intercostal neuralgia is treated comprehensively, that is, by treating not only the pain symptom, but also the cause of the neuritis.
The complex of therapeutic measures includes the following aspects:
- the use of non-steroidal anti-inflammatory drugs to reduce the severity of pain;
- the use of complex preparations of B vitamins to normalize the transmission of nerve impulses;
- decongestant medications help eliminate swelling at the site of pinched nerve and restore tissue circulation;
- Physiotherapy techniques, such as acupuncture, darsonvalization, therapeutic massage, cope well with such pathologies of the nervous system.
Neuralgia is perfectly amenable to diagnosis and treatment, and its prognosis is very favorable, which is encoded with the code M79.2.
Save the link, or share useful information on social media. networks
Prognosis and prevention
With timely treatment, a favorable prognosis for recovery is observed.
With mild to moderate severity of the pathology, sensitivity and motor activity are restored within 8-10 weeks. Rehabilitation against the background of severe pathology takes a longer time.
To prevent the development of neuritis, it is recommended to resort to the following preventive measures:
- promptly treat infectious and viral diseases;
- keep the body warm, prevent hypothermia;
- balance the diet;
- avoid increased physical stress on your hands;
- to refuse from bad habits.
People who are indicated for long periods of bed rest are advised to take a comfortable position . Paralyzed or comatose patients need to change body position every 2 hours and massage the elbow joint area.
Ulnar nerve neuritis is accompanied by inflammation of the nerve tissue, which impairs sensitivity and motor activity of the hand.
The disease is easy to diagnose by the external manifestations of the pathological process : the hand bends like a bird's paw, the patient feels tingling, numbness and muscle weakness.
To treat the disease, complex therapy is carried out with drugs, exercise therapy, massage and physiotherapy. Rehabilitation with timely diagnosis and initiation of treatment is possible within 2 months.
Features of post-traumatic arthritis
Traumatic arthritis is a fairly common pathology. The disease develops due to insufficient attention to one’s own health. Avoiding this complication is not at all difficult; you just need to consult a doctor if you receive an injury and provide rest to the damaged joint for a while.
Most often, professional athletes or people whose activities involve increased stress on the joints experience post-traumatic arthritis.
A feature of post-traumatic arthritis is a slow increase in symptoms. The disorder develops against the background of injuries received over a long period of time. Pathology leads to a slowly developing disorder of motor activity in the affected joint
The difficulty is that a person often does not pay attention to pain and decreased range of motion, associating these symptoms with a recent injury. Most people believe that the discomfort will go away on its own after some time is needed to recover from the injury.
During this time, arthritis slowly progresses, destroying bone and cartilage tissue.
Due to the way the human body distributes stress, traumatic arthritis most often affects the lower legs, knees, and small joints of the feet.
Diagnostics
Neurologists make a diagnosis of polyneuropathy based on:
- analysis of complaints and how long ago symptoms appeared;
- clarification of possible causative factors;
- establishing the presence of diseases of internal organs;
- establishing the presence of similar symptoms in close relatives;
- identifying signs of neurological pathology during a neurological examination.
An obligatory component of the diagnostic program is an examination of the lower extremities in order to identify autonomic failure:
- thinning of the skin of the legs;
- dryness;
- hyperkeratosis;
- osteoarthropathy;
- trophic ulcers.
During a neurological examination, if the nature of the polyneuropathy is unclear, doctors palpate the available nerve trunks.
To clarify the cause of the disease and changes in the patient’s body, the Yusupov Hospital determines the levels of glucose, glycated hemoglobin, protein metabolic products (urea, creatinine), perform liver tests, rheumatic tests, and toxicological screening. Electroneuromyography allows one to evaluate the speed of impulse transmission along nerve fibers and determine signs of nerve damage. In some cases, a nerve biopsy is performed for examination under a microscope.
If there are indications, instrumental methods for studying the somatic status are used: radiography, ultrasound. Cardiointervalography allows identifying violations of autonomic function. A study of cerebrospinal fluid is carried out if demyelinating polyneuropathy is suspected, and when searching for infectious agents or an oncological process.
Vibration sensitivity is examined using a biotensiometer or a graduated tuning fork with a frequency of 128 Hz. The study of tactile sensitivity is carried out using hair monofilaments weighing 10 g. Determination of the threshold of pain and temperature sensitivity is carried out using a needle prick and a Tip-therma thermal tip in the skin of the dorsal surface of the big toe, dorsum of the foot, medial surface of the ankle and lower leg.