2.The main common causes of the development of carpal tunnel syndrome
The main common causes of the development of carpal tunnel syndrome include:
- monotonous, systematically repeated physical activity (sports or professional, for example, computer typing, weight training, truck drivers’ habit of putting their elbow out the open window, and many others);
- injuries;
- frequent vibration or temperature exposure;
- endocrine diseases (diabetes mellitus, hypothyroidism, etc.).
Visit our Neurology page
Anatomy of the ulnar nerve and cubital tunnel
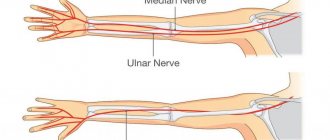
The ulnar nerve originates in the cervical plexus, being one of the three main nerves of the upper limb. It runs along the inner surface of the shoulder, then lies in the canal formed by the olecranon process, the internal epicondyle and the ligament that connects these two bone formations, forming a rather narrow cubital canal.
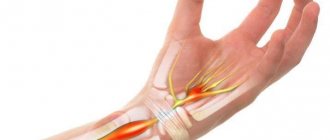
Next, the nerve passes through the intermuscular space of the forearm, flowing into another channel, this time on the wrist. This canal is called the Guyon Canal. It is at the level of this canal that the ulnar nerve begins to divide into 3, sometimes 4 branches, ending with the sensory branches of the 5th and inner half of the 4th fingers, as well as the motor branches of the 3-4-5 lumbrical muscles of the hand.
Diagnosis of cubital tunnel syndrome
When examining the elbow joint by a doctor, the patient may notice a significant increase in pain. A painful examination is necessary for a specialist to make an accurate diagnosis:
- If the nerve is compressed in the canal, there will be a positive Tinnel's sign, which is manifested by the sensation of a current shooting through the nerve into the little and ring fingers when the doctor taps with a neurological hammer - although this can happen when the nerve is without pathology, with a strong blow.
- The doctor will check to see if the nerve slips out of the canal when the patient bends the arm at the elbow.
- Tests sensitivity and strength in the hand and fingers.
If the doctor has doubts about the causes of cubital tunnel syndrome, the patient may be recommended to undergo additional examinations, such as MRI, ENMG, and radiography.
Radiography. Based on radiographs, it is possible to determine bone exostoses in the projection of the canal, which compress the nerve. But most of the causes of compression of the ulnar nerve cannot be seen on x-ray, since they are of soft tissue etiopathogenesis.
Electroneuromyography (ENMG). This study makes it possible to determine how well the impulses are transmitted along the nerve and to determine at what level and how much the nerve is compressed.
During nerve conduction testing, the nerve is stimulated proximally and the time required to conduct the impulse is measured and compared with normal values.
Treatment
If a person experiences discomfort only after squeezing the elbow, then conservative treatment is carried out. The load on the cubital canal is reduced, including in the form of flexions in this section, which contributes to the rapid restoration of its function.
To completely eliminate the load, at night the arm is fixed in such a way that it does not bend at all at the elbow. For example, a bent or twisted towel is tied to the elbow with a bandage, which does not allow the arm to bend.
When working with a computer, you will also need to hold your elbow, and when driving a vehicle, straighten your arms as much as possible.
In order for the symptoms of the disease to disappear as quickly as possible, you will have to use external anti-inflammatory drugs. In this case, Voltaren gel helps well, which is applied to the affected area up to 3-4 times a day. Such drugs can relieve pain and swelling, which often causes the development of cubital tunnel syndrome.
NSAID drugs are an important treatment measure for cubital tunnel syndrome. If they do not help, your doctor may prescribe stronger corticosteroids. For example, a Hydrocortisone injection in combination with an anesthetic has a good effect.
Sometimes doctors prescribe vitamin B6 for quick recovery, but it is worth remembering that you cannot take it on your own. Only a doctor can determine the advisability of its use and the required dosage.
This conservative treatment can last up to a month. In some cases it may take longer. But if numbness in the elbow persists, then the doctor may decide on surgical intervention.
Clinical picture[edit | edit code]
The cubital canal is formed in front by the medial epicondyle of the humerus, on the lateral side by the elbow joint, and on the medial side by the two heads of the flexor carpi ulnaris. There are structures proximal, distal, and within the cubital tunnel that can cause compression, entrapment, tension, dislocation, or irritation of the ulnar nerve. Structures located proximal to the canal include the arcade of Straders (not to be confused with the ligament of Straders, which causes compressive neuropathy of the median nerve) and the medial head of the triceps muscle. Within the canal, damage can be caused by the medial epicondyle, the ulnar nerve groove, the anconeus muscle, the two heads of the flexor carpi ulnaris muscle, and the arch of tendinum connecting them (Osborn's ligament); Distally, ulnar nerve injury may be contributed to by the fascia of the flexor carpi profundus. Regardless of the location of compression, compression neuropathy develops ischemia and fibrosis of the ulnar nerve.
The first symptom is pain in the medial ulnar region of varying intensity, periodically radiating to the medial forearm. Paresthesia may occur in fingers innervated by the ulnar nerve. Athletes typically seek medical attention before forearm muscle weakness occurs. The first step is to determine whether there is damage to the ulnar collateral ligament, which may accompany cubital tunnel syndrome. When the ulnar nerve is dislocated, patients may feel a clicking sensation in the joint. The diagnosis is based mainly on the clinical picture and the results of two provocative tests. In most patients, when tapping in the projection of the place of compression of the ulnar nerve, Tinel's symptom appears. The second test involves full flexion of the elbow joint and maximum extension of the wrist joint. The test is considered positive if pain or paresthesia occurs after a minute. Sensitivity is examined using a monofilament esthesiometer, and in advanced cases, discriminatory sensitivity is assessed. Impaired motor function develops later and is rare in athletes. These include asymmetric atrophy of the eminence of the little finger, weakening of the rough and pinch grip, abducted position of the little finger (Wartenberg's sign), Froment's sign, and claw deformity of the fingers innervated by the ulnar nerve. With a variant of the anatomical structure, when the wrist flexors are innervated by the median nerve (Martin-Gruber anastomosis), motor disorders may be absent even in advanced cases.
To exclude diseases with similar manifestations, such as cervical radiculopathy, neuropathy of the medial bundle of the brachial plexus, thoracic outlet syndrome, a thorough examination of the neck and shoulder girdle is performed.
Plain x-rays and x-rays in special projections can reveal bony changes in the cubital canal area that cause compression of the ulnar nerve. MRI can identify soft tissue changes that are causing compression. Electromyography does not detect abnormalities in more than 50% of cases. Pathological changes are characterized by a slowdown in the speed of propagation of excitation along the nerve of less than 50 m/s with the elbow joint bent. A decrease in the action potential of sensory nerve fibers confirms the diagnosis of early neuropathy.
Causes of cubital tunnel syndrome
The cause of this particular disease is compression of the nerve in the cubital canal. In this article we do not discuss nerve injury.
There are several causes of cubital tunnel syndrome:
- repeated trauma to the ligaments and bone structures of the elbow joint that form the canal,
- intense sports,
- arthritis, arthrosis of the elbow joint
- synovitis of the elbow joint or hemarthrosis
- repeated monotonous activities,
- consequences of fractures can also be the causes of the syndrome.
For drivers, the disease can be caused by the habit of placing their elbow on the window opening of the car door. When symptoms appear, this habit will have to be eradicated.
At the computer, you should pay attention to the position of your hand when working on the keyboard and mouse. When doing this type of work, the forearm should rest completely on the tabletop. You can put something soft under the sore elbow.
Compression of the ulnar nerve in the canal can be caused by inflammatory processes not only in the nerve tissue, but also in the soft tissue component of the cubital canal wall. For example, with medial epicondylitis, inflammation in the projection of the internal epicondyle can cause swelling and compression of the nerve. Failure to consult a doctor in a timely manner and delays in starting treatment can lead to organic damage to the wall and the process becoming chronic. As a result of the thickening of the nerve sheath, the transmission of nerve impulses may become difficult, leading to loss of sensation and motor function in some muscles of the hand and forearm.
Treatment[edit | edit code]
Treatment of cubital tunnel syndrome begins with conservative measures (rest, cold, NSAIDs, immobilization of the upper limb with a splint with a soft pad in the position of flexion at the elbow joint at an angle of 30-45°). In the early stages, immobilizing the affected arm overnight in an extended position is often very effective. Due to the superficial location of the nerve, glucocorticoid blocks are not recommended. In athletes, conservative treatment is often ineffective due to the inability to rest the arm and the high risk of ulnar nerve dislocation. Indications for surgical treatment: unsuccessful conservative treatment, dislocation of the ulnar nerve, as well as lesions of the elbow joint that contribute to compression of the ulnar nerve (for example, medial instability). Several operations have been developed to relieve compression: simple decompression of the cubital tunnel, medial epicondylectomy, subcutaneous and submuscular transposition of the ulnar nerve. All of them are aimed at eliminating possible causes of compression: from the ligament of Straders proximal to the cubital canal to the two heads of the flexor carpi ulnaris distal to the canal.
Although the success rate for all of these primary surgeries is 85% and all of these surgeries can cause complications, submuscular ulnar nerve transposition is now the preferred procedure for athletes. After simple decompression alone, recurrence is possible because the medial epicondyle is left behind, which can compress the ulnar nerve. Performing a medial epicondylectomy alone may result in instability of the ulnar nerve and may also cause damage to the medial ligamentous complex. Therefore, subtotal medial epicondylectomy is recommended only in selected cases. With submuscular transposition, the ulnar nerve is placed between the flexors and pronator teres, which eliminates compression, reduces tension on the nerve and protects it from injury. This operation requires more extensive tissue dissection. In addition, cutting the flexor and pronator teres muscles at their insertion on the medial epicondyle and then suturing them after repositioning the ulnar nerve anteriorly can cause weakness of these muscles. After short-term postoperative immobilization, passive and then active movements begin (at the 4th week). Weight-bearing exercises and throwing exercises begin at 8 weeks postoperatively.
Signs and symptoms of cubital tunnel syndrome
Symptoms of cubital tunnel syndrome include each of the following:
It is not necessary to have all the signs.
- Stiffness, loss of sensation, or significant dull or sharp pain in the ulnar part of the hand, 4th and 5th fingers.
- Pain and weakness when attempting to grasp an object with a brush.
- Discomfort in the elbow area.
Such symptoms indicate ischemia (lack of blood supply) of the nervous tissue. These symptoms are most pronounced in the morning, after the hand has been resting overnight. After some time, when the patient performs a certain amount of movements, the pain and numbness slightly recedes.