Stroke: stages and tactics of intensive care (lecture)
Professor, academician of the Russian Academy of Natural Sciences and MANEB Nazarov I.P.
| Part 1 - Diagnostics | Part 3 – Neuroprotection |
| Part 2 – Stroke Treatment | Part 4 – Hemorrhagic stroke |
Part 1. Diagnostics, stages of assistance
Introduction.
Stroke is one of the leading causes of morbidity and mortality in the world. As the population ages, the burden of this disease on society will become greater. In terms of prevalence, stroke is the most significant cause of morbidity and long-term disability. It is also the second leading cause of dementia, the most common cause of epilepsy in adults, and a common cause of depression.
The incidence of stroke is 2.5 - 3 cases per 1000 population per year, mortality is 1 case per 1000 population per year. Mortality in the acute period of stroke in Russia reaches 35%, increasing by 12-15% by the end of the first year after a stroke. Post-stroke disability ranks first among all causes of disability and is 3.2 per 10,000 population. 20% of people who have had a stroke return to work, despite the fact that one third of people with stroke are people of working age.
Thus, in Russia, 400–450 thousand people develop stroke annually, approximately 200 thousand of them die. There are more than 1 million people in the country who have suffered a stroke, and 80% of them are disabled. Despite the fact that primary prevention plays a decisive role in reducing mortality and disability due to stroke, a significant effect in this regard is achieved by optimizing the system of care for patients with stroke, introducing treatment and diagnostic standards for these patients, including rehabilitation measures and the prevention of recurrent strokes. The European Regional Office of the World Health Organization (WHO) believes that the creation of a modern system of care for patients with stroke will reduce mortality during the first month of the disease to 20% and ensure independence in everyday life 3 months after the onset of the disease for at least 70% of surviving patients.
According to the WHO definition: Stroke is a rapidly developing focal or global disorder of brain function, lasting more than 24 hours or leading to death, if other genesis of the disease is excluded. Acute cerebrovascular accident (ACVA, stroke) is the sudden (within minutes, less often – hours) appearance of focal neurological symptoms (motor, speech, sensory, coordination, visual, auditory, etc.) and/or general cerebral disorders (changes consciousness, headache, vomiting, etc.). Symptoms persist for more than 24 hours.
Main risk factors for stroke
| Uncorrectable risk factors | Adjustable risk factors |
| Age | Hypertension |
| History of stroke or stroke | Diabetes |
| Stroke or myocardial infarction from blood relatives | Atrial fibrillation |
| Migraine | Smoking |
| Gender (men are larger than women) | Hypercholesterolemia |
| Ethnicity | Thrombosis factors |
| Constriction of carotid or vertebral Arteries | Excessive alcohol consumption |
| Psycho-emotional overload. | Excessive salt intake |
Distribution of “risk factors” for the development of cerebrovascular insufficiency
( G. J. Hankey ,
J. M. Wardlaw , 2002 ) _ _ _
| The most important “Risk Factors” | Frequency of occurrence of the factor in patients with signs of cerebrovascular accident |
| Tendency to increase blood pressure | 50 – 75% |
| Heart diseases | 35 – 40% |
| Lipid disorders | 40 – 45% |
| Abuse of alcohol, smoking | 10 – 20% |
| Increased salt intake | 25 – 30% |
| Excess body weight | <15% |
| Unfavorable heredity | 5-10 % |
| Frequent stressors | 5% |
| Physical inactivity | 8% |
Stroke is divided into hemorrhagic and ischemic (cerebral infarction). Ischemic stroke accounts for about 80%, although recently published data in the journal Stroke (Shiber JR, Fontane E, Adewale A. Stroke registry: hemorrhagic vs ischemic strokes. Am J Emerg Med. Mar 2010;28(3):331-333), based on a retrospective review of data obtained from stroke centers increased the proportion of hemorrhagic stroke to 40.9%. The authors attribute this increase to improved diagnostics due to the use of SCT and the increased use of antiplatelet agents and warfarin.
According to the nature of the course, a small stroke is also distinguished, in which the impaired functions are completely restored during the first 3 weeks of the disease. However, such relatively mild cases occur in only 10-15% of stroke patients.
Transient cerebrovascular accidents (TCI)
are characterized by the sudden onset of focal neurological symptoms that develop in a patient with vascular disease (arterial hypertension, ischemic heart disease, rheumatism, etc.) and last several minutes, less often – hours, but no more than a day and end with complete restoration of impaired functions.
Transient neurological disorders with focal symptoms that develop as a result of short-term local cerebral ischemia are also referred to as transient ischemic attacks (TIA).
A special form of PNMK is acute hypertensive encephalopathy (AHE).
More often, acute hypertensive encephalopathy develops in patients with malignant arterial hypertension and is clinically manifested by severe headache, nausea, vomiting, impaired consciousness, convulsive syndrome, and in some cases is accompanied by focal neurological symptoms.
The appearance of a TIA or minor stroke indicates a high risk of repeated and, as a rule, more severe stroke (since the pathogenetic mechanisms of these conditions are largely similar) and requires their prevention. Recent population-based and hospital-based epidemiological studies have demonstrated a high risk of stroke immediately after TIA. Studies have shown that prompt evaluation of patients with TIA in the clinic and immediate initiation of treatment reduces the risk of stroke after TIA. This emphasizes the need for emergency hospitalization of patients with TIA for evaluation and immediate treatment.
Stages of medical care for stroke
The main principle of managing patients with acute stroke is the staged organization of medical care.
The following stages are distinguished:
I. Diagnosis of stroke and emergency measures at the prehospital stage.
II. The earliest possible hospitalization of all patients with stroke.
III. Diagnosis of the nature of the stroke.
IV. Clarification of the pathogenetic subtype of stroke.
V. Selection of optimal treatment tactics.
VI. Rehabilitation and measures for secondary prevention of stroke.
Stages of medical care for acute stroke and the goals of its provision:
1. Prehospital
(doctor, family or local doctor, ambulance or FAP paramedic)
- Diagnosis of stroke
- Carrying out emergency treatment measures
- Hospitalization
Diagnostics:
History (presence of cerebrovascular pathology, high blood pressure and other risk factors). Acute development of neurological symptoms (weakness in the limbs, impaired speech, breathing, consciousness, facial asymmetry, etc.).
The main task at the prehospital stage is the correct and rapid diagnosis of stroke as such. An exact determination of the nature of the stroke (hemorrhagic or ischemic) is not required; it is only possible in a hospital after CT or MRI studies of the brain. The clinical picture of the development of stroke is characterized, as a rule, by the sudden (within minutes, less often hours) appearance of focal (or cerebral, and in the case of subarachnoid hemorrhage (SAH) - meningeal symptoms.
For correct and timely diagnosis of stroke, it is necessary to know the focal, cerebral and meningeal symptoms characteristic of this disease.
Diagnostic and treatment methods
Treatment tactics depend on the type of major stroke, the patient’s age, concomitant diseases and other factors. With the hemorrhagic type, it is important to eliminate the source of bleeding, and some patients may require surgery to remove the hematoma or aneurysm. For ischemic stroke, therapy is carried out in several directions:
- correction of breathing and heartbeat;
- elimination and prevention of brain swelling;
- thinning the blood and preventing the formation of blood clots;
- symptomatic treatment aimed at relieving seizures, fever and other clinical signs.
The Clinical Institute of the Brain has all the necessary conditions for the treatment and rehabilitation of patients with strokes. At the first stage, all procedures must be carried out in a hospital, under round-the-clock supervision of doctors. In addition, in the first weeks the likelihood of a second attack is increased, and it is important not to miss its first symptoms. After complete stabilization, treatment continues at home, with mandatory examinations and constant monitoring of the patient’s condition.
Focal symptoms
1. Unilateral (right or left) motor disorders in the limbs in the form of paresis (decreased muscle strength) or paralysis (complete lack of movement in the limb) are the most common symptoms of stroke. Test. You can identify paresis in the following way: ask the patient to hold his arms outstretched forward for a few seconds; the affected arm will drop faster. In case of complete paralysis, the patient will not be able to hold his hand in front of him at all.
2. Speech disorders (dysarthria, aphasia). In the case of aphasia, both the understanding of addressed speech (the patient will not comply with requests and commands) and his own speech production may be impaired - the patient cannot construct his own speech. Dysarthria is manifested by unclear, “blurred” speech, there is a feeling of “porridge in the mouth”, the patient’s perception of the addressed speech does not suffer. Test. To identify the presence of speech disorders, ask the patient to say his name or say a simple phrase.
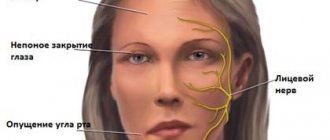
3. Facial asymmetry (smoothness of the nasolabial fold). Test. It is necessary to ask the patient to smile or show teeth and gums.
4. Unilateral (in the arm and/or leg) sensitivity disorders (hypoesthesia) – there is a feeling as if the patient was “lying down” on his limb; he may not feel touching it. Test. To identify sensory disorders, it is necessary to apply injections to symmetrical areas of the limbs on the right and left. If there are sensory disorders, the patient will not feel the injections on one side or feel them significantly weakened.
5. Oculomotor disorders. Paresis of gaze to the side may occur (restriction of movements of the eyeballs), up to a forced tonic rotation of the eyeballs. An ominous symptom is anisocoria (different pupil sizes), which usually occurs due to dislocation of the brain (in this case, due to superior - temporotentorial - herniation). Test. To check gaze paresis, it is necessary to ask the patient to follow an object moving horizontally and illuminate the pupils with a flashlight to compare their sizes and photoreaction.
6. With a stroke, there may be other focal symptoms - hemianopsia (loss of half the visual fields), dysphagia (swallowing disorders) and others.
What may be needed when a patient is in intensive care. Let's summarize
For hygiene
- lined disposable absorbent diapers;
- wet wipes 30 * 40 cm;
- liquid soap for washing skin;
- camphor alcohol;
- foam with panthenol for treating bedsores;
- diapers (check size and absorbency)
For tube feeding:
- nutritional mixtures (jelly, liquid porridge, broths);
- ready-made forms for tube feeding (available at the pharmacy)
Discuss with your doctor what you need at the moment, what you can bring and how much.
General cerebral symptoms
This group of symptoms includes: disturbances in the level of consciousness, headache, nausea, vomiting, dizziness, convulsions. General cerebral symptoms are characteristic signs of increased intracranial pressure with subarachnoid or intracerebral hemorrhage, extensive cerebral infarction.
Criteria for clear consciousness:
the patient is awake, correctly assesses the environment, is oriented in time, place, situation and his own personality.
There are quantitative (unproductive) and qualitative (productive) forms of disturbance of the level of consciousness.
Quantitative (“depression of consciousness”) forms include: stunning
(superficial and deep),
stupor, coma
(first, second and third degree). Currently, it is generally accepted to use assessments of the degree of depression of consciousness - the Glasgow scale.
Stunning (moderate, deep) - characterized by impaired attention, loss of coherence of thoughts or actions. When stunned, the patient is awake, but he is lethargic, drowsy, quickly becomes exhausted and falls asleep.
Stupor - the patient opens his eyes only after exposure to a strong stimulus (loud sound, pain, strong smell, etc.) The reaction to verbal instructions is weak or absent, there is no speech production. At the same time, targeted and local defensive reactions remain intact.
Coma is a complete loss of consciousness; we cannot awaken the patient. Superficial coma (first degree) - it is impossible to wake the patient, he reacts to painful stimuli with simple, erratic movements, there is no opening of the eyes to any irritation. Vital functions are not depressed.
Deep coma (second degree) - the patient does not respond with motor reactions to painful stimuli. Most reflexes are suppressed, but breathing and hemodynamics are still not there.
Atonic coma (third degree) is the complete absence of the patient’s response even to very strong painful stimulation. Muscle atony, areflexia, impaired or absent breathing, depression of cardiac activity may be observed.
Qualitative changes in consciousness consist in the fact that the patient is awake, but productive contact with him is difficult or impossible due to severe psychotic disorders. Examples of such conditions are dementia, delirium, twilight state of consciousness and a number of others. Psychomotor agitation is often observed.
Headache is most typical for hemorrhagic forms of stroke. For example, with subarachnoid hemorrhage, the headache is very intense, unusual in nature, appears like a “blow” to the head, and there may be a feeling of heat, pulsation, or a hot wave inside the head.
Convulsive seizures (tonic, tonic-clonic, clonic-tonic, generalized or local) are often observed at the onset of a stroke (primarily hemorrhagic).
Dizziness, nausea, and vomiting are not symptoms specific to acute stroke, but are often the leading reason for seeking medical help at “03” services or a clinic. In addition, like other general cerebral symptoms, they indicate the need for emergency symptomatic therapy.
Rules for visiting a patient
The intensive care unit is a special department, the operating mode of which differs from that established in the general ward of the hospital department. If the attending physician has given permission to visit a patient in intensive care, adhere to the following rules:
- Do not visit a patient if you have an infectious disease. Postpone your visit until you recover;
- Remove outer clothing before entering the emergency room or intensive care unit. Put on a robe, mask and cap;
- Visitors under the influence of alcohol or drugs are prohibited from visiting;
- Speak quietly, don't shout. Do not touch medical equipment and follow the instructions of medical personnel;
- No more than 2 visitors are allowed at the same time;
- Visiting children under 14 years of age is prohibited;
- During medical procedures and procedures, visits are prohibited;