When visiting a neurologist, more than 30% of patients present with somatic complaints that cannot be explained by any organic disease [1, 2].
Thus, the diagnosis of “tension headache” (TTH) ranks second in frequency among the 20 most common diagnoses established by a neurologist [3]
.
At a specialized otoneurological appointment, the diagnosis of “non-vestibular vertigo” takes second place after “benign paroxysmal positional vertigo” (BPPV) [4].
Suffice it to say that the prevalence of irritable bowel syndrome (IBS), according to various sources, reaches 10-20% in the population [5], the number of patients with functional disorders of the gastrointestinal tract (GIT) in a specialized gastroenterology hospital is about 45% [6] , and IBS - 23% [7] .
Similar data can be provided for other clinical functional syndromes, in particular chronic fatigue syndrome (CFS), hyperventilation syndrome, non-cardiac chest pain, intersitial cystitis, non-bacterial prostatitis, etc.
Below are the functional symptoms encountered at appointments with doctors of different specialties: gastroenterology - IBS, non-ulcer dyspepsia; rheumatology - fibromyalgia; cardiology - non-cardiac chest pain; pulmonology - hyperventilation syndrome; infectious diseases - CFS; neurology - tension-type headache, back pain, functional dizziness, psychogenic seizures, paresis, dysbasia, etc.; dentistry - atypical facial pain; ENT diseases - feeling of a “lump in the throat”; allergology - multiple chemical sensitivity (pseudoallergies); uro-gynecology - intersitial cystitis, non-bacterial prostatitis, chronic pelvic pain, premenstrual syndrome.
The clinical picture of the above diseases is dominated by chronic pain syndromes and various subjective sensations (dizziness, lack of air, fatigue, “lump in the throat”). Along with subjective symptoms, objectively recorded disorders are also detected (changes in the frequency and nature of stool, tachycardia, increases in blood pressure, changes in breathing patterns, swelling, signs of nonspecific immunity disorders, etc.). The predominance of functional symptoms is detected at the population level, at the general practitioner’s appointment and among patients referred for consultation to a specialist [8]. These patients are often prescribed various consultations, expensive studies and treatments, which, as a rule, do not lead to a positive result, causing dissatisfaction for both the patient and the doctor [9].
Terminology and classification
In domestic medicine, such disorders are most often referred to as “vegetative dystonia syndrome” (G-90.9, ICD-10) or “astheno-neurotic reactions” (F-48.0, R-53, ICD-10); in therapeutic practice the term “ neurocirculatory dystonia" (NCD) (F-45.3, ICD-10), in gastroenterology there is IBS (K-58, ICD-10). Some authors use the term “psychovegetative syndrome”, proposed in the 60s of the last century by German internists [10] .
In the practice of foreign colleagues, the terms SVD and NDC are practically not used today. As a rule, doctors prefer to use terms that denote specific clinical syndromes, for example, tension-type headache, “non-coronary pain”, “non-ulcer dyspepsia”, IBS, “hyperventilation syndrome”, CFS. Various terms have been used to denote this entire category of diseases: “somatoform”, “somatized” [11-13], “medically unexplained symptoms” ( eng.
.: medically unexplained symptoms) [14], “subjective health complaints” (
English
: subjective health complaints) [15].
However, these terms are not satisfactory, since most of them are based not on positive, but on negative criteria. Currently, terms with more positive content are proposed: “bodily distress syndrome” [
16, 17] and “dysfunctional syndromes” [18, 19].
Term «
functional diseases” was proposed back in the 80s of the last century [20].
The latest American Classification of Mental Illnesses, released in 2013, made significant changes to the Somatoform Disorders category, which was renamed Somatic Symptoms and Related Disorders. Officially to
refer to somatic and neurological symptoms. without an organic cause, the terms “functional somatic symptoms” (FSS) and “functional neurological symptoms” (FNS) were proposed. These changes are proposed to be used in preparing the next 11th version of the International Classification of Diseases (ICD-11). The advantage of the latter terms is their positive meaning. Firstly, the presence of any violations is emphasized, i.e. the validity of the patient’s complaints; secondly, the term is acceptable for the patient, since the term “unexplained” does not sound disturbing to the patient; thirdly, the role of the psychogenic factor, the existence of which is beyond doubt, is not emphasized, but is not recognized by the patient, and its mention usually causes internal resistance from the patient.
Not only changes in terminology are discussed, but also the movement of this category of diseases from the class of mental diseases to neurological ones. Very important are the DSM-5 comments for this class of diseases, which “recommend diagnosis in the presence of stressful somatic symptoms in response to which inappropriate thoughts, feelings and behavior arise” [21].
Thus, when diagnosing functional disorders, it is proposed not only to exclude an organic disease, but also to identify positive criteria, i.e., the patient’s erroneous ideas about the disease and its consequences, emotional reactions and changes in behavior in response to these stressful symptoms.
These patients are united into a single category of functional disorders by the presence of symptoms common to different functional disorders (comorbidity). Clinicians often observe suppression of symptoms characteristic of different functional diseases, sometimes simultaneously, sometimes sequentially [22]. Thus, patients with IBS or non-ulcer dyspepsia present complaints not only of a gastroenterological nature. Upon detailed questioning, they reveal symptoms characteristic of CFS, complaints of chest pain of non-cardiac origin, and allergies of unknown etiology. CFS can be combined with manifestations of fibromyalgia [23], premenstrual tension and headache of unknown etiology. Of the 12 patients with functional syndromes, 8 complained of bloating, 8 of constant headache, 6 of abdominal pain, 6 of chronic fatigue [24]. From 2 to 25 non-gastroenterological symptoms occur per patient in 84% of patients with IBS, while associated symptoms most often manifest themselves as pain in different parts of the body [25, 26]. In almost 80%, IBS symptoms are combined with functional disorders in the urological area [27 ], and in 35-44% - with pelvic pain [25, 28]. These facts show that the specificity of these syndromes is blurred by many repetitions of common symptoms [24]. All these data support the assumption that patients with one functional syndrome meet criteria for other functional diseases. It is no coincidence that questions arise about the uniqueness of each individual syndrome and about the possibility of forming a clinical picture of the disease from a group of syndromes [24].
According to a number of studies, in ¾ of patients with IBS, symptoms persisted for 10 years or more after their identification, which led to significant costs for repeated examinations and treatment [29]. Similar data were obtained for functional neurological disorders. Thus, after 12 years, FNS persisted in 83% of patients, and other FNS and FSS also appeared; the majority of these patients continued to remain in distress, were disabled and in need of medical care [30].
Clinical analysis of large samples of patients with CFS [31],
fibromyalgia [32], IBS [33, 34], and non-ulcer dyspepsia [35] showed that these syndromes are significantly more common in women. Thus, the ratio of women to men with IBS is 2-2.5:1 [36], and among patients visiting specialized medical institutions, it reaches 5:1 [37]. The ratio of women to men observed in a specialized gastroenterological institution with IBS is 2.5:1 [38]. These data allow us to discuss the role of sex hormones in the pathogenesis of functional disorders in different systems.
In the vast majority of patients with functional disorders, evidence of abuse in childhood, mental, physical or sexual violence in the family can be identified. These situations are considered as extreme stress, leading to the development of post-traumatic stress syndrome (PTSD) with irreversible changes in the central nervous system, neuroendocrine and immune regulation [39-41]. It is believed that it is these disorders that subsequently play a significant, if not leading role in the formation and chronicization of functional disorders.
It has been shown that not only violence, but also a number of factors that disrupt the quality of interaction between people providing primary care for a child during the first 18 years of life (including serious maternal illness, marital discord, divorce) can have an equally detrimental effect on predisposition of an adult to diseases [42]. Data on the role of psychosocial factors in the onset, chronicity and exacerbation of IBS symptoms are extensive [43]. Childhood sexual abuse was more often detected in the anamnesis of patients with CFS, as well as in patients with functional gastrointestinal diseases in comparison with organic ones [44, 45]. In women with chronic pelvic pain, a history of abuse led to hypocortisolemia and disturbances in its fluctuations in the concentration of cortisol in the blood, which was not observed in healthy women [46]. Patients with FNS reported a higher frequency of physical and sexual abuse compared to patients suffering from affective disorders. [47].
The important role of personality traits and emotional disorders in the genesis of functional diseases, their course and response to therapy has been revealed. A number of studies using standard personality questionnaires have shown a significant predominance compared to controls of such personality traits as neuroticism, introversion, isolation, anxiety, depression, as well as personality disorders of obsessive-compulsive, paranoid, schizoid and avoidant types in patients with CFS, psychogenic dizziness , IBS [48-50]. These patients are more often diagnosed with chronic anxiety, depressive and somatoform disorders.
Traditionally, this category of patients is prescribed standard therapy, which is symptomatic in nature: patients with tension-type headaches receive painkillers; for functional gastrointestinal diseases, proton pump inhibitors, H2 receptor blockers, antidiarrheals or laxatives are prescribed; for chronic non-vestibular vertigo - betahistines, etc. Standard symptomatic therapy or so-called on-demand therapy is generally ineffective in the long term. Its results are short-term and often minimal. Thus, patients with IBS follow a diet for years, take antispasmodics, prokinetics, antidiarrheal drugs or laxatives, but their effectiveness is short-lived and concerns only individual symptoms. Patients with tension-type headache take analgesics for a long time (often in large doses) and at the same time note that they do not relieve the headache. Moreover, long-term use of analgesics leads to the development of abuse, which in turn contributes to the chronicity of headaches.
Functional disorders in general medical practice: diagnosis and therapy
Functional diseases - what are they?
Functional diseases today refer to disorders in which even a thorough examination of the patient does not reveal organic disorders that could explain the existing symptoms (Reuber et al., 2005).
In almost every medical specialty there are such patients. Table 1 presents functional syndromes in the practice of doctors of different specialties (Wessely et al., 1999). Table 1. Functional syndromes in general medical practice
Functional somatic symptoms are present in 20-25% of cases at the initial consultation and in 35% of patients in the hospital (Hamilton et al., 1996).
It is important to note that the quality of life in patients with functional disorders (FDs) suffers significantly more than in organic patients: they visit doctors more often, they require significantly more diagnostic tests, and, as a rule, the prescribed therapy is ineffective.
Traditionally, in these cases, the medical diagnosis algorithm is based on negative examination data: normal laboratory tests, Holter monitoring, EEG, ultrasound, X-ray, CT, MRI, biopsy and other studies. The absence of deviations from the norm leads the doctor to diagnose a “functional disorder” of one or another organ or system.
Since the 1980s, interest in these patients has increased significantly. In various fields of medicine, scientific directions are being created that study the clinical manifestations and pathogenesis of individual risk factors. The most well-known include the Rome Foundation, which has become the leading organization in relation to functional diseases of the gastrointestinal tract (Drossman et al., 1997, 2006), the Association of Functional Neurological Disorders Society, and communities and groups studying functional vestibular disorders (Staab et al., 2017). More detailed studies of various risk factors have revealed many common patterns in their clinical manifestations and pathogenesis. However, it is difficult for a doctor to imagine that the pathogenesis of irritable bowel syndrome, hyperventilation syndrome, chronic tension headache and hyperkinetic syndrome develops and exists according to the same patterns. All this raised the key question: “Is this one disease or many?” (Wessely et al., 1999). As a result, positive criteria for functional diseases were formulated, which are shown in Table 2 (Dyukova et al., 2017).
Table 2. Criteria for a positive diagnosis of functional disorders
In the 11th version of the International Classification of Diseases (ICD-11), instead of the term “somatoform disorders”, terms with more positive content are proposed: “bodily distress syndrome” and “dysfunctional syndromes”. To denote somatic and neurological symptoms that do not have an organic cause, the terms “functional somatic symptoms” (FSS) and “functional neurological symptoms” (FNS) have been proposed.
The importance of using criteria for a positive diagnosis of RF is dictated by the need for early diagnosis, since the long course of the disease naturally leads to its chronicity and, accordingly, to a worsening prognosis for the effectiveness of therapy .
Therapy for functional disorders
The vast majority of patients with RF are observed and treated either by neurologists or general medical practitioners. The dominance of asthenia, pain and vegetative syndromes in the clinical picture, the hidden nature of emotional disorders often prompts doctors to use predominantly somatotropic drugs in therapy: antihypertensive and vegetotropic drugs, analgesics, vascular-metabolic therapy, antioxidants, adaptogens, etc. And only in cases of obvious emotional disorders can tranquilizers be included in therapy. Such therapy often turns out to be ineffective, undermining the patient’s faith in the possibility of a cure and contributing to the chronicity of the process.
Already at the first contact, the doctor must determine the further strategy for managing the patient. If the doctor has a good idea of the algorithm for treating a particular organic symptom, then the therapy of such a patient baffles him. Traditionally, drugs of “uncertain” and “doubtful” action are prescribed: metabolic, immunocorrective, vascular, nootropic, etc. Typically, the effect of these drugs is comparable to the effect of placebo.
Despite the fact that pain and autonomic disorders are the most obvious in the clinical picture, psychopharmacology is currently the basic method of treatment. Psychotherapy also plays a significant role.
The main goals of RF therapy are:
- relief of the leading symptom or syndrome;
- impact on secondary syndromes (anxiety, phobias, including agoraphobia, depression, asthenia);
- prevention of relapses and further progression of the disease.
For this purpose, the following are used: symptomatic, pathogenetic and preventive therapy . Sometimes an explanatory conversation with a doctor about the essence of the disease, perhaps in combination with placebo therapy, is enough. Studies have shown that in 35–42% of patients suffering from RF, significant improvement was achieved only with the help of placebo therapy (Dyukova et al., 1992).
Symptomatic therapy is aimed at quickly relieving the leading symptom. This stage of therapy has several goals. Firstly, rapid relief of the patient’s condition, which in itself has a psychotherapeutic effect, since it removes the fear of a threatened and incurable disease. Secondly, relief of the leading symptom prevents the process from becoming chronic. Thus, rapid and early relief of acute back pain prevents the development of persistent muscle spasm, which is an important pathogenetic mechanism for the formation of chronic back pain. Early and successful relief of a panic attack prevents the development of agoraphobic syndrome and restrictive behavior, which are the main factors of social disability in patients with functional disorders.
Symptomatic therapy may include various approaches. For most functional symptoms, pharmacological drugs are used as symptomatic therapy - the so-called “treatment on demand”: to relieve nausea - prokinetics (cerucal), to reduce tachycardia - beta-blockers, to relieve pain - non-steroidal anti-inflammatory drugs and muscle relaxants, for relief diarrhea - antidiarrheal drugs (loperamide), panic attacks - tranquilizers. It is necessary to remember and explain to the patient that this treatment operates on the “here and now” principle and is a short-term therapy, which will be canceled as the main pathogenetic therapy takes effect. Moreover, the patient’s healing process is characterized by a decrease in the need for these “life-saving” drugs. Often the patient himself does not yet realize a noticeable improvement in his condition, and the doctor can make him understand this if in the conversation he focuses on the obvious decrease in the number of “on-demand” medications taken in the last week. Thus, the effectiveness of pathogenetic therapy is substantively proven to the patient.
Pathogenetic therapy is aimed at preventing the reappearance of paroxysmal manifestations (panic attacks, psychogenic seizures, pain attacks, etc.), regression of the abusive factor, relief of anticipation anxiety, agoraphobic syndrome and restrictive behavior, secondary depression, asthenia and other motivational disorders.
Over the past 40 years, drugs designated in medical reference books as antidepressants (ADs) have become widespread in general medical practice. And although the name of this large group of drugs and the official indications for their use state that they should be used only for depression and comorbid anxiety as part of psychiatric disorders, nevertheless, many years of medical experience and modern research data indicate that these drugs are effective not only for depression, but also for chronic anxiety, aggression, dysphoria, bulimia and a wide variety of functional somatic and neurological diseases that general practitioners often encounter.
Numerous multicenter placebo-controlled studies have shown that antidepressants are the cornerstone drugs in the treatment of functional disorders (Kroenke, 2007). ADs are effective for chronic pain syndromes of various localizations (Dharmshaktu, 2012; Fishbain, 2000), chronic functional dizziness (Lin, 2013), functional gastrointestinal disorder (Bixquert-Jiménez, 2005; Clouse, 1994), panic disorders (Gorman, 1997; Freire , 2011), asthenic syndrome (Pae, 2009). Moreover, ADs are effective, regardless of whether these syndromes are combined with depression or not, and the doses used for the treatment of RF are significantly lower than for the treatment of major depressive disorder.
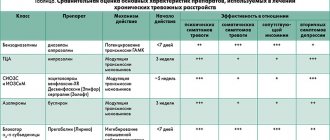
It should be noted that the pronounced side effects of a number of ADs, in particular tricyclic ADs, significantly reduce the possibility of their use, especially in outpatient practice. Therefore, the drugs of first choice are currently drugs from the group of selective serotonin reuptake blockers (SSRIs) (fluoxetine, fluvoxamine, sertraline, paroxetine, citalopram and escitalopram) and selective serotonin and norepinephrine reuptake blockers (SNRIs) (venlafaxine, duloxetine and milnacipran) .
The choice of drug is determined mainly by the clinical picture of the disease and the characteristics of the drug. The following rules may be helpful in determining the dose:
- Taking into account the individual sensitivity and anxious suspiciousness of this category of patients, it is advisable to start therapy with small doses (1/4-1/2 of the planned dose) with a gradual increase over 3-5 days.
- The criterion for limiting the dose may be the severity of side effects that do not disappear within 3-5 days.
- A daily distribution of the drug is recommended depending on the hypnogenic effect.
Before prescribing a course of drug therapy, the doctor must explain to the patient the basic principles of therapy and warn about possible difficulties in the treatment process. The following points need to be emphasized in this conversation:
- The essence of the treatment is that it is aimed at preventing the recurrence of symptoms and the social adaptation of the patient.
- The effect of therapy may be delayed; In most patients, the effect of AD appears with a latent period of 14–21 days from the start of their use at full dose.
- The course of treatment should be long, sometimes it can last up to a year.
- Abrupt withdrawal of drugs at any stage of treatment can lead to exacerbation of the disease, so drug withdrawal is carried out gradually.
An important aspect of treatment is psychotherapy, aimed at the formation of new patterns and stereotypes of behavior, correct cognitions, motivations, emotional, affective and behavioral reactions.
In 1998, a meta-analysis of randomized placebo-controlled trials of the effectiveness of antidepressants for psychogenic pain syndromes was conducted. From 155 publications, 11 studies were selected that met the criteria for analysis. The results showed that in this category of patients, AD reduced pain intensity significantly more than placebo (Fishbain et al., 1998, 2000). Another study showed a significantly greater effectiveness of antidepressants in the treatment of patients with somatoform pain in whom pain was the leading syndrome (89 patients), in contrast to patients where the leading syndrome was FNS (185 patients), and pain was a concomitant disorder. At the same time, it should be noted that in the first group, depressive disorders, both manifest and manifest, or hidden, were significantly more likely to be present (Heinemann, 2003). A wide range of antidepressants today allows you to choose a drug depending on the range of its side effects, additional effects (stimulating or sedative effects), and influence on abnormal behavioral patterns.
There are enough publications in the scientific literature on the effectiveness of venlafaxine in the treatment of functional disorders. The drug has been shown to significantly reduce pain in tension-type headaches (Zissis, 2007), fibromyalgia (Dwight et al., 1998; Sayar et al., 2003) and other pain syndromes, including neuropathic ones (Grothe Dale et al. ., 2004). The effectiveness of the drug increases significantly if pain is associated with depression (Heinemann, 2003). Venlafaxine is effective not only for depression, but also for anxiety disorders - GAD, panic disorders, social phobias. It is known that anxiety is the leading pathogenetic link in the development and maintenance of functional somatic disorders.
Currently, the pharmacological company Egis produces venlafaxine under the trade name “VELAXIN” in 2 forms: in the form of tablets of 37.5 and 75 mg, and also in the form of capsules of 75 and 150 mg. The advantage of the drug in capsule form is its prolonged action. So, at the beginning of treatment, the patient can take a minimum dose of ½ tablet of 37.5 mg and, gradually increasing the dose, bring it to 75 mg, and then switch to 1 capsule (75 mg) of prolonged action. In this way, it is possible to increase the patient’s compliance with therapy and achieve an adequate dose.
Bibliography
- Bixquert-Jiménez M, Bixquert-Pla L. Antidepressant therapy in functional gastrointestinal disorders. Gastroenterol Hepatol. 2005; 28(8):485–92.
- Clouse RE, Lustman PJ, Geisman RA, Alpers DH. Antidepressant therapy in 138 patients with irritable bowel syndrome: a five-year clinical experience. Aliment Pharmacol Ther. 1994; 8(4):09–16.
- Dharmshaktu P, Tayal V, Kalra BS. Efficacy of antidepressants as analgesics: a review. J Clin Pharmacol 2012; 52(1):6–17.
- Drossman DA, Whitehead WE, Camilleri M. Irritable bowel syndrome: a technical review for practice guideline development. Gastroenterology. 1997; 112:2120–2137
- Drossman DA. The functional gastrointestinal disorders and the Rome III process. Gastroenterology 2006; 130:1377–1390.
- Dwight MM, Arnold LM, O'Brien H, Metzger R, Morris-Park E, Keck PE Jr. An open clinical trial of venlafaxine treatment of fibromyalgia. Psychosomatics 1998; 39:14–7.
- Dyukova GM, Shepeleva IP, Vorob'eva OV. Treatment of vegetative crises (panic attacks). Neurosci Behav Physiol, 1992; 22(4):343–5.
- Fishbain D. Evidence-based data on pain relief with antidepressants. Ann Med, 2000; 32(5): 305–16.
- Fishbain DA, Cutler RB, Rosomoff HL, Rosomoff RS Do antidepressants have an analgesic effect in psychogenic pain and somatoform pain disorder? A meta-analysis // Psychosom-Med. 1998; 60(4):503–509.
- Freire RC, Hallak JE, Crippa JA, Nardi AE. New treatment options for panic disorder: clinical trials from 2000 to 2010. Expert Opin Pharmacother, 2011; 12(9):1419–28.
- Functional Neurological Disorders Society
- Gorman JM. The use of newer antidepressants for panic disorder. J Clin Psychiatry 1997; 58 Suppl 14:54–8;
- Grothe Dale R., Scheckner Brian, Dominick Albano, Treatment of Pain Syndromes with Venlafaxine. Pharmacotherapy 2004; 24(5):621–629.
- Hamilton J, Campos R, Creed F. Anxiety, depression and management of medically unexplained symptoms in medical clinics. JR Coll Physicians 1996; 30:18–21.
- Heinemann AC Klinicher und diagnostischer Stellenwert von Schmerzsymptomen bei 274 Patienten einer neurologischen Universitätsklinik mit psychogenen Symptomen. 2003.
- Kroenke K. Efficacy of treatment for somatoform disorders: a review of randomized controlled trials. Psychosom Med. 2007; 69(9):881–888.
- Lin E, Aligene K. Pharmacology of balance and dizziness. NeuroRehabilitation. 2013;32(3):529–42.
- Pae CU, Marks DM, Patkar AA, Masand PS, Luyten P, Serretti A. Pharmacological treatment of chronic fatigue syndrome: focusing on the role of antidepressants. Expert Opin Pharmacother, 2009, 10(10): 1561–70.
- Reuber M. et al. Functional symptoms in neurology: questions and answers J Neurol Neurosurg Psychiatry 2005,76:307–314.
- Sayar K, Aksu G, Ak I & Tosun M. Venlafaxine treatment of fibromyalgia. The Annals of Pharmacotherapy 2003; 37:1561–1565
- Staab JP et al. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the Classification of Vestibular Disorders of the Bárány Society // J. Vestib. Res. 2021. Vol. 27, No. 4. P. 191–208.
- Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes: one or many? Lancet. 1999; 354(11):936–9.
- Zissis NP, Harmoussi S, Vlaikidis N, Mitsikostas D, Thomaidis T, Georgiadis G, Karageorgiou K. A randomized, double-blind, placebo-controlled study of venlafaxine XR in out-patients with tension-type headache. Cephalalgia. 2007; 27(4):315–24.
- Dyukova G.M. et al. Functional disorders: taxonomy of clinical manifestations and pathogenesis. Journal of Neurology and Psychiatry. Korsakova, 12, 2021, 137-144. doi: 10.17116/jnevro2016116121
The effectiveness of multimodal therapy
Numerous multicenter placebo-controlled studies have shown that the most effective in the treatment of all functional disorders are information and educational programs [51], cognitive behavioral psychotherapy, physical therapy rehabilitation, including dosed physical activity and the use of antidepressants. The effectiveness of these methods has been shown for CFS [52], functional vertigo [4], fibromyalgia [53], IBS [54], and FNS [55].
The key concepts in the treatment of patients with functional disorders are psychological involvement in the therapy process with awareness and acceptance of one’s own thoughts, feelings and condition without criticism and condemnation. In this context, the English-language literature uses the term “mindfulness” - “non-judgmental awareness”. The purpose of this line of therapy is cognitive regulation of the perception of symptoms [56].
It is known that the basic drugs for the treatment of chronic pain syndromes of various localizations are antidepressants (AD) [57]. They are effective whether chronic pain is combined with depression or not. ADs turned out to be effective not only for the treatment of emotional disorders and pain, but also for such disorders as tachycardia, dyspnea, frequency and character of stool, postural phobic dizziness, etc. [58-60]. Thus, in a 16-week prospective study of the effectiveness of sertraline in patients with chronic subjective dizziness, it was shown that at a dose of 25–200 mg/day (average dose 100 mg/day), the drug caused more than 50% reduction in dizziness in 73% of patients, and 40% have complete remission [59].