Hospitalization and treatment under the compulsory medical insurance quota. More details after viewing the pictures.
A brain abscess forms against the background of an infectious process. The disease is the result of the penetration of pathogens into the cranial cavity. A large formation causes an increase in intracranial pressure and can lead to severe complications, including the death of the patient. Signs of a brain abscess are an indication to contact a neurosurgeon. Pathology requires the provision of qualified medical care.
Abscess of brain tissue is caused by staphylococci, E. coli, various anaerobic bacteria, and streptococci. The infection enters the brain through contact or hematogenous routes. The cause of the disease can be inflammatory processes in the lungs, ENT organs, consequences of injuries, gunshot wounds, and long-term immunodeficiency conditions.
The Medsi Clinic treats brain abscess using all available surgical techniques. Drug therapy for this disease is used only at the initial stage of development. The gold standard of neurosurgery is surgical intervention.
Causes
“Blue” heart defects, open and penetrating traumatic brain injury, lung pathology, as well as bacterial endocarditis and the presence of immunodeficiency (including those caused by HIV) can increase the risk of developing a brain abscess. The main pathogens are Escherichia coli, staphylococci, toxoplasma, anaerobic bacteria, streptococci, pneumococci, fungi and meningococci. 25% contain a sterile abscess. The infection enters the brain through contact or hematogenous means, also known as metastatic.
Diagnostic procedures for identifying AGM
Suspecting a disease, the patient is subjected to thorough examinations to refute or establish the fact of its presence on reasoned grounds. It is necessary to take into account that in the late period the clinical picture is similar to that of brain tumors. The principle of differentiation plays a huge role in diagnosis. It is based on anamnesis data about the patient’s infectious and inflammatory diseases and the use of imaging methods.
Computed tomography with contrast is a fundamental method that allows one to distinguish purulent pathogenesis in brain tissue from intracranial neoplasms, to establish the exact location, size, type and multiplicity of the lesion, and perifocal signs. The following are used as auxiliary diagnostic techniques to clarify the diagnosis:
- magnetic resonance imaging;
- echoencephalography;
- cerebral angiography;
- abscessography.
The patient is given directions for general laboratory tests, which are a mandatory part of any diagnostic program. But, as experts point out, laboratory tests, unlike neuroimaging methods, do not play a key role in making a diagnosis. For example, ESR, high C-reactive protein values, and elevated white blood cell counts characterize many body conditions associated with inflammation and infections. That is, these are not specific, but general infection indicators. Moreover, cultures for bacteremia in a dominant amount (almost 90% of patients) ultimately turn out to be sterile.
Types of disease
Most often in the clinic there are contact abscesses caused by otitis, mastoiditis, suppuration in the nasal cavities, meninges, orbit or skull bones.
- Otogenic. Occurs in most cases. An abscess is more often complicated by chronic purulent otitis than by an acute process. In the case of otitis media, the infection enters the brain from the temporal bone through the cavernous sinuses and the roof of the tympanic cavity into the middle fossa of the skull, resulting in inflammation of the brain in the temporal lobe of the brain. An infection of otogenic origin can also penetrate into the posterior cranial fossa, passing through the labyrinth and then the sigmoid sinus, which is why a cerebellar abscess occurs.
- Rhinogenic. Often concentrated in the frontal parts of the brain. First, it is caused by local pachymeningitis, after which it passes into the stage of adhesive limited meningitis and ultimately this process ends with the formation of limited purulent encephalitis in the brain tissue. It is very rare that rhinogenic and otogenic types of disease manifest themselves hematogenously as a result of sinuses, venous thrombosis or septic arteritis. In this case, the abscesses are concentrated deep in the brain.
- Traumatic. Often occur during open skull trauma. If the dura mater is damaged, the infection enters the brain tissue through the perivascular gaps. If a foreign body enters the brain, the infection enters along with it. Nowadays, traumatic abscesses reach 15% of all possible types of this disease.
- Metastatic. Often occurs as a result of lung diseases such as pleural empyema, pneumonia (pneumonia) or bronchiectasis. Such abscesses are accompanied by the penetration of infection into the brain by septic embolism. About 30% of metastatic abscess diseases are multiple and form in the deep parts of the white matter of the brain.
Pathogenesis: how does the process develop?
The development of the disease consists of 4 separate stages, or stages:
- The first stage is early infiltration. During the first 3 days after entry of the pathogenic agent, a poorly demarcated diffuse focus of inflammation is formed with destruction of brain tissue and swelling around it.
- The second stage is late cerebritis. The center of focal inflammation undergoes suppuration and necrotization on days 4-9, which is accompanied by the formation of a cavity. The cavity is filled with semi-liquid purulent exudate. Fibroblasts accumulate along the outer part.
- The third stage is the formation of the gliosis capsule. From 10-13 days the protective capsule of the abscess begins to form. Thus, there is an intensification of the growth of the layer of fibroblasts bordered by a rim of neovascularization. Along with this, reactive astrorcytosis is noted.
- The last stage (4th stage) is the final formation of the capsule. The capsular component around the filled purulent cavity is fully compacted (reactive collagen takes part in this). The necrotic focus takes on clear outlines.
Further processes at the last stage depend on the virulence of the pathogenic flora, the route of spread, the immune status of the patient, and the level of hypoxia of the affected brain structures. The correctness of diagnostic and therapeutic measures will no less affect the degree of progression of AGM. As a rule, the disease cannot regress on its own. Without adequate therapy, in the vast majority of cases, the internal volume of the abscess increases, and the appearance of new infected areas along the periphery of the capsule cannot be ruled out.
Diagnostics
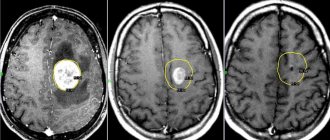
Diagnosis of the disease is made using MRI or computed tomography, both with and without contrast enhancement. Identifying the source of infection is essential for further treatment of the abscess and its successful completion. In most cases, the purulent process occurs in teeth affected by caries, the air sinuses of the nose, and the middle ear.
Symptoms of sinusitis
There are acute and chronic forms of sinusitis, which differ in their symptoms.
Acute sinusitis. Symptoms:
- Runny nose lasting more than 7-10 days, without signs of improvement;
- nasal congestion, mucous or purulent discharge from the nose;
- mucus running down the back of the throat, copious discharge of purulent sputum in the morning;
- headache, heaviness and pain in the inflamed sinus area. Sometimes pain in the teeth, eyes, cheekbones, cheeks;
- increased sensitivity of the facial skin in the projection of the affected sinus;
- increase in body temperature (up to 38°C and above). As a rule, this symptom is observed in an acute case. In a chronic process, body temperature rarely rises or remains at subfebrile levels (37-37.50°C);
- weakness, fatigue, irritability. Photophobia, lacrimation, loss of appetite, sleep disturbance;
- weakened or absent sense of smell;
- swelling of the cheeks and eyelids.
Chronic sinusitis. Symptoms:
Symptoms of chronic sinusitis depend on the form of the disease. Outside of an exacerbation, symptoms may be very mild or absent. The most common symptoms of concern are:
- nasal congestion, difficulty in nasal breathing;
- scant mucous or purulent discharge from the nose, may be in the form of drying crusts;
- constant leakage from the nose, causing cracks and abrasions at the entrance to the nose;
- mucus running down the back of the throat;
- dry throat;
- headache;
- bad breath.
As the disease worsens, symptoms characteristic of acute sinusitis may appear.
Treatment
Therapy for the disease must be comprehensive. Most often, surgical intervention is used in combination with adequate combination antibacterial therapy. Antibacterial therapy can last several weeks. Subsequently, a long period of rehabilitation is required. Depending on the resulting neurological defect, one should resort to neuroprotective therapy, massage, exercise therapy, and sometimes, when symptomatic epilepsy develops, the selection of antiepileptic drugs is necessary.
Brain abscess (Cerebral abscess)
At the encephalitic stage of the abscess (history of up to 2 weeks), as well as in the case of a small brain abscess (up to 3 cm in diameter), conservative treatment is recommended, the basis of which should be empirical antibacterial therapy. In some cases, it is possible to perform a stereotactic biopsy for the purpose of final verification of the diagnosis and isolation of the pathogen.
Abscesses that cause brain dislocation and increased intracranial pressure, as well as those localized in the area of the ventricular system (pus entering the ventricular system often leads to death) are absolute indications for surgical intervention. Traumatic brain abscesses located in the foreign body area are also subject to surgical treatment, since this inflammatory process cannot be treated conservatively. Despite the poor prognosis, fungal abscesses are also an absolute indication for surgery.
Contraindications to surgical treatment are brain abscesses located in vital and deep structures (the optic thalamus, brain stem, subcortical nuclei). In such cases, it is possible to carry out a stereotactic method of treatment: puncture of the brain abscess and its emptying, followed by washing the cavity and administering antibacterial drugs. Both single and multiple (through a catheter installed for several days) rinsing of the cavity is possible.
Severe somatic diseases are not an absolute contraindication to surgical treatment, since stereotactic surgery can also be performed under local anesthesia. An absolute contraindication to surgery can only be an extremely serious condition of the patient (terminal coma), since in such cases any surgical intervention is contraindicated.
Drug treatment
The goal of empirical (in the absence of culture or when it is impossible to isolate the pathogen) antibacterial therapy is to cover the maximum possible range of pathogens. Recommended treatment programs:
- For brain abscess without a history of TBI or neurosurgical intervention, the following treatment algorithm is indicated: vancomycin; III generation cephalosporins (cefotaxime, ceftriaxone, cefixime); Metronidazole. In the case of post-traumatic brain abscess, metronidazole is replaced with rifampicin.
- The causative agent of brain abscess in patients with immunodeficiency conditions (except HIV) is most often Cryptococcus neoformans, less often Candida spp or Aspergillius spp. Therefore, in these cases, amphoreticin B or liposomal amphoreticin B is prescribed. After the abscess disappears (according to neurovisualization studies), fluconazole is used for 10 weeks, subsequently the dose is halved and left as a maintenance dose.
- In patients with HIV, the causative agent of brain abscess is most often Toxoplasma gondii, so empirical treatment of patients should include sulfadiazine with pyrimethamine.
After isolation of the pathogen from culture, treatment must be changed, taking into account the antibiogram. If cultures are sterile, empirical antibiotic therapy should be continued. The duration of intensive antibiotic therapy is at least 6 weeks, after which it is recommended to change the antibiotics to oral ones and continue treatment for another 6 weeks.
The prescription of glucocorticoids is justified only in the case of adequate antibacterial therapy, since only with a positive prognosis can glucocorticoids cause a decrease in the severity and reverse development of the brain abscess capsule. In other cases, their use may cause the inflammatory process to spread beyond the primary focus.
Surgery
The main methods of surgical treatment of intracerebral abscesses are simple or inflow-outflow drainage. Their essence is to install a catheter into the abscess cavity, through which the pus is evacuated, followed by the administration of antibacterial drugs. It is possible to install a second catheter of a smaller diameter (for several days), through which a rinsing solution is infused (most often, 0.9% sodium chloride solution). Drainage of the abscess must be accompanied by antibacterial therapy (first empirical, then taking into account the sensitivity of the isolated pathogen to antibiotics).
Stereotactic aspiration of abscess contents without installing a drain is an alternative method of surgical treatment of brain abscess. Its main advantages are lenient requirements for the qualifications of medical staff (close attention and special knowledge are required to control the functioning of the inflow and outflow system) and a lower risk of secondary infection. However, in 70% of the use of this method, repeated aspirations are necessary.
In the case of multiple brain abscesses, it is necessary first of all to drain the focus that is most dangerous in terms of complications (breakthrough of pus into the ventricular system, brain dislocation), and also the most significant in the clinical picture. In the case of empyema or subdural abscess of the brain, drainage is used without using the inflow and outflow system.
Sinusitis in children
Sometimes sinusitis in children is more difficult to see than sinusitis in adults. The disease usually develops after an infection: influenza or sore throat, and is often accompanied by otitis media. The symptoms are somewhat blurred and appear weaker than in adults. Here are the main ones:
- purulent or mucous discharge from the nose;
- general weakness, malaise;
- pungent odor from the mouth.
With sinusitis in children, one side of the face is often inflamed. While sinusitis in adults is often accompanied by headaches, headaches in children are extremely rare.