Hospitalization and treatment under the compulsory medical insurance quota. More details after viewing the pictures.
Chronic subdural hematoma of the brain is a pathological condition in which there is an accumulation of blood between the arachnoid and dura mater. The main cause of the disease is traumatic brain injury (TBI). The disease accounts for about 40% of all intracranial hemorrhages. Hematoma can appear at any age. Experts distinguish subdural traumatic and non-traumatic hemorrhage.
Classification
Subdural hematomas are classified according to the speed of development of clinical signs. There are the following types of hemorrhages:
- acute subdural hematoma: manifestations occur within seventy-two hours from the moment of injury;
- subacute subdural hematoma is defined when symptoms develop within four to fourteen years after injury;
- chronic subdural hematoma is characterized by the onset of symptoms several weeks or months after injury (usually more than three weeks).
Subacute and chronic types of hemorrhages occur more often as a result of vascular damage under the influence of various factors; acute – as a result of traumatic brain injury. Subdural hemorrhage occurs with equal frequency both on the side of injury and on the opposite side according to the biomeanical principle of counter-impact (the brain is displaced to the side opposite to the impact and can be injured when colliding with the bone skull on the opposite side).
What diseases can it be associated with?
In approximately half of the cases with subdural hematomas, bradycardia is recorded. Congestion in the fundus is a common component of compression syndrome. In the chronic course, there is a decrease in visual acuity and elements of optic disc atrophy. It should be noted that due to severe concomitant brain contusions, subdural hematomas, especially acute ones, are often accompanied by brainstem disorders in the form of respiratory disorders, arterial hyper- or hypotension, early hyperthermia, diffuse changes in muscle tone and reflex sphere.
Often, a change in pupil diameter with a subdural hematoma is accompanied by ptosis of the upper eyelid on the same side; this is combined with limited mobility of the eyeball and most often indicates a craniobasal radicular genesis of oculomotor pathology.
Symptoms
The symptoms of a subdural hematoma are extremely variable. Manifestations of hematoma are caused by local, cerebral and brainstem disorders. A “light” period is characteristic - the time period immediately after the injury, when there are no manifestations. The duration of the “light” interval can vary from minutes and hours to several days. In chronic forms, this period can be months or years.
Subdural hematomas are characterized by an undulating course, while other patients may suddenly fall into a coma.
Focal symptoms depend on the location of the hemorrhage, general cerebral symptoms depend on its volume and the amount of compression of the brain, brainstem symptoms depend on the nature of the lesion in the brainstem and the percentage of its wedging into the foramen magnum.
Tests and diagnostics
In terms of diagnostics, patients are prescribed:
- X-ray of the skull in two projections.
- Echoencephalography.
- Angiography of the brain (to determine vascular disorders).
- CT scan. The main CT sign is displacement of brain structures, which is noted in 100% of cases. The degree of displacement ranges from 5 to 28 mm. On CT, epidural hematomas have a lenticular or lens-shaped shape and are localized in the area of the temporal bone. The subdural hematoma has a crescent shape and crosses the suture lines.
- MRI of the brain accurately determines the location, volume and structure of hematomas, which makes it possible to determine the tactics of surgical treatment.
Variants of the course of the disease
There are three main variants of the clinical picture of subdural hemorrhages:
- Classic clinic. A change in the state of consciousness occurs in three phases: loss of consciousness at the time of injury, a clear “bright” interval, and repeated loss of consciousness. During the recovery period, the patient reports severe headaches, nausea, dizziness, and possible memory loss. Focal symptoms manifest themselves later, during the period of deepening stunning. At the same time, a sharp increase in headache occurs and vomiting develops.
Focal symptoms: most often these are mydriasis, sensitivity disorders, contralateral pyramidal insufficiency (lack of brain function appearing on the opposite side from the side of the lesion).
From stem symptoms
: secondary stem syndrome (decrease in heart rate, respiratory dysfunction, tonic convulsions).The three-phase clinical pattern is more common for the subacute form than for the acute form. In these cases, euphoria and decreased criticism of one’s condition may occur.
- Option with an erased picture of the “light” gap. Primary loss of consciousness can reach the level of coma. Stem and focal symptoms are clearly expressed. Then there is a partial restoration of consciousness (usually to the point of stunning). After some time, the patient again falls into stupor or coma, and the disturbances in vital functions deepen. Epileptic seizures may develop, and hemiparesis increases.
- Option without a “light” gap. Occurs with multiple, severe brain injuries. The patient is in a stuporous state or in a coma. Moments of clarity of consciousness are either erased or absent; there is practically no positive dynamics noted.
Every year in Russia, about 600 thousand people suffer traumatic brain injury (TBI). 50 thousand of them die, and another 50 thousand become disabled. The incidence of TBI in men is twice as high as that in women, with this relationship maintaining in all age groups.
The most common causes of TBI
Typical clinical manifestations of traumatic brain injury.
TBI is characterized by a three-phase change in consciousness: a primary short-term loss of consciousness at the time of injury, subsequent recovery ( light interval ) and, after a certain period of time, repeated loss of consciousness . However, such a classical development of changes in the state of consciousness is not always observed. Often there are cases that occur without a light gap, or it is erased. Sometimes there may be no primary loss of consciousness. The duration of the clear interval (both with full and partial restoration of consciousness) in most patients with acute EDH is measured in several hours or even minutes.
Patients who have suffered a trauma and are accessible to contact usually complain of a headache with increasing intensity. In many cases, the headache has a bright shell-like hue, radiates to the eyeballs, jaws, and is accompanied by photophobia, hyperesthesia with characteristic facial reactions. The headache is usually constant with periodic crisis-like exacerbations, often accompanied by repeated vomiting . In severe pain, victims moan, demand help, grab their heads with their hands, toss in bed, and lose sleep.
After a traumatic brain injury, patients often experience bradycardia (in almost 1/2 of patients, the pulse rate does not exceed 60 beats per minute); in approximately 1/4 of the observations, an increase in maximum blood pressure above 150 mm Hg is noted. Art.
In victims with traumatic hematomas, it is almost always possible to identify one or another focal symptomatology . Among the signs of damage to the cerebral hemispheres, the first place belongs to motor disorders (weakness in the arm and leg, most often opposite the side of the hematoma). The severity of these disorders varies - from anisoreflexia to hemiplegia (paralysis).
Occasionally, the clinical picture of intracranial hematomas includes symptoms of irritation of the cerebral cortex in the form of general or focal epileptic seizures .
Among craniobasal symptoms, the most important role in the clinic of TBI is given to the dilation of one pupil with a decrease or loss of its reaction to light .
Clinical classification of TBI.
According to the clinical picture, traumatic brain injury is divided into:
1. Focal • brain contusions (mild, moderate, severe), • intracranial hematomas (epidural, subdural, intracerebral), • subdural hygromas, • depressed fractures, • head compression;
2. Diffuse • concussion, • diffuse axonal damage, • subarachnoid hemorrhage.
Diagnostics.
Currently, the gold standard when examining patients with traumatic brain injury is the following set of examinations: 1. Clinical examination by a neurosurgeon. 2. X-ray of the skull in two (at least) projections. 3. Echoencephalography. 4. CT (computed tomography) of the brain. The issue of additional examination methods is decided individually.
Very often, epidural hematomas are accompanied by a fracture of the skull bones.
Types of intracranial hematomas.
Brain contusions include focal macrostructural damage to its substance as a result of trauma. According to the unified clinical classification of traumatic brain injury adopted in Russia, focal brain contusions are divided into three degrees of severity: 1) mild, 2) moderate, and 3) severe.
| CT scan of the brain. Severe brain contusion, intracerebral hematomas of both frontal lobes. |
Epidural hematomas are a collection of blood caused by trauma, located between the inner surface of the skull bones and the dura mater, causing local and general compression of the brain.
The frequency of epidural hematomas among observations of initially hospitalized victims with TBI varies widely from 0.54% to 9%.
Causes of epidural hematomas. A temporary local deformation of the skull that occurs during an injury, often with a depressed fracture of the skull bones and rupture of the vessels of the dura mater, leads to the release of blood from the damaged vessel, which, exfoliating the dura mater, spreads within the cranial sutures, where the shell is tightly fused with the internal bone plate. For this reason, epidural hematomas have a smaller area of distribution and greater thickness than subdural hematomas.
| CT scan of the brain. Acute epidural hematoma in the left occipital region with brain dislocation and compression. |
Subdural hematomas are a volumetric accumulation of blood caused by trauma, located between the dura and arachnoid maters and causing local and general compression of the brain.
Subdural hematomas are more common than epidural hematomas. Isolated SDH accounts for approximately 2/5 of the total number of cases of brain-compressing intracranial hemorrhages; they occupy first place among various types of hematomas.
| CT scan of the brain. Acute subdural hematoma in the right fronto-parietal-temporal region with brain dislocation and compression. |
Post-traumatic chronic subdural hematomas are encapsulated volumetric hemorrhage located under the dura mater and cause local and general compression of the brain. The incidence of these hematomas ranges from 2 to 13 cases per 100,000 population per year, increasing significantly in elderly and senile people.
Chronic subdural hematomas differ from acute and subacute traumatic hematomas by a demarcation capsule that usually appears 2 weeks after the injury, which determines all the features of their pathogenesis, clinical course and treatment tactics. The volume of CSH ranges from 50 ml to 250 ml and is more often 100-150 ml.
If previously chronic subdural hematomas were detected exclusively in elderly and senile people, now they have become significantly “younger”, occurring quite often in young and middle-aged people, as well as in children.
The distinctive clinical sign of these hematomas is that the clear interval can last for weeks, months and even years. Clinical manifestation is extremely polymorphic. There is both a gradual development of compression syndrome and a sudden sharp deterioration in the patient’s condition to stupor and coma, spontaneously or under the influence of various additional factors (mild repeated head injury, overheating in the sun, alcohol consumption, colds, etc.).
The clinical picture may resemble various diseases of the central nervous system: benign and malignant brain tumors, etc. During the period of a detailed clinical picture of chronic subdural hematoma, changes in consciousness in the form of stupor or amentive confusion with impaired memory and orientation are frequent.
| CT scan of the brain. Bilateral chronic subdural hematomas. |
Damage to the structures of the posterior cranial fossa (PCF) is one of the severe types of traumatic brain injury (TBI). Their peculiarity lies in their extremely difficult clinical diagnosis and high mortality. Before the advent of computed tomography, the mortality rate for PCF injury was close to 100%.
The clinical picture of damage to the structures of the PCF is characterized by a severe condition that occurs immediately after the injury: depression of consciousness, a combination of cerebral, meningeal, cerebellar, and brainstem symptoms due to rapid compression of the brainstem and impaired cerebrospinal fluid circulation. If there is significant damage to the substance of the cerebrum, hemispheric symptoms are added.
The proximity of the location of damage to the PCF structures to the liquor-conducting pathways causes their compression and disruption of liquor circulation by a small-volume hematoma. Acute occlusive hydrocephalus, one of the most severe complications of damage to the structures of the posterior canal, is detected in 40%.
Treatment.
All patients with clinical signs of compression of the brain, as well as when this compression is detected on CT or MRI in severely ill patients, are advised to undergo urgent surgery - removal of the hematoma.
Consequences of subdural hematoma
The occurrence of subdural hemorrhage is accompanied by rapid displacement of the brain and infringement of its stem structures. Subdural hematoma usually develops against the background of severe damage to the skull and brain, and therefore has an unfavorable prognosis.
The outcome and consequences of a subdural hematoma of the brain depend on the speed of recognition of the hemorrhage and the competently chosen treatment method. The prognosis is based on other factors: the patient’s age, the volume of hemorrhage, somatic complications. Statistics today indicate a high mortality rate among such patients and disability among survivors.
Treatment of other diseases starting with the letter - s
| Treatment of salmonellosis |
| Treatment of cutaneous sarcoidosis |
| Treatment of pulmonary sarcoidosis |
| Treatment of Kaposi's sarcoma |
| Treatment of uterine sarcoma |
| Treatment of Ewing's sarcoma |
| Treatment of type 2 diabetes mellitus |
| Treatment of type 1 diabetes mellitus |
| Treatment of seborrhea |
| Treatment of sepsis |
| Treatment of heart failure |
| Treatment of anthrax |
| Treatment of Budd-Chiari syndrome |
| Treatment of Guillain-Barré syndrome |
| Treatment of Gilbert's syndrome |
| Treatment of Parhon's syndrome |
| Treatment of polycystic ovary syndrome |
| Treatment of empty sella syndrome |
| Treatment of irritable bowel syndrome |
| Treatment of Sjögren's syndrome |
| Treatment of sinusitis |
| Treatment of systemic lupus erythematosus |
| Treatment of systemic scleroderma |
| Treatment of systemic sclerosis |
| Treatment of syphilis |
| Treatment of scoliosis |
| Treatment of somatoform disorders |
| Treatment of spinal stroke |
| Treatment of spondylosis and spondyloarthrosis |
| Treatment of laryngeal stenosis |
| Treatment of tracheal stenosis |
| Treatment of stenosing ligamentitis |
| Treatment of tetanus |
| Treatment of stomatitis |
| Treatment of ringworm |
| Treatment of subarachnoid hemorrhage |
The information is for educational purposes only. Do not self-medicate; For all questions regarding the definition of the disease and methods of its treatment, consult your doctor. EUROLAB is not responsible for the consequences caused by the use of information posted on the portal.
Treatment
It is performed conservatively or surgically, depending on its type, volume, as well as the individual characteristics of the patient. In the acute form, removal of the subdural hematoma is often indicated. Detection of displacement and compression of brain structures is a stimulus for surgery as soon as possible from the moment of injury (or rupture of a vessel).
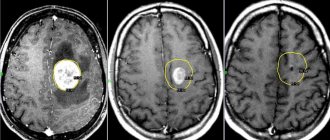
a) With MRI without contrast, the image reveals areas of fluid accumulation indicated by white arrows - subacute subdural hematomas. b) MRI visualizes foci of increased signal intensity (indicated by white arrows), as well as foci of reduced MRI signal intensity (indicated by black arrows), these signs are characteristic of acute subdural hematomas.
The absolute indication for surgical treatment of a subdural hematoma is the thickness of the accumulated blood more than one centimeter, determined by imaging studies (MSCT, MRI). The postoperative period should be accompanied by the maintenance of vital functions and control of intracranial pressure.
The operation is also indicated for subacute subdural hemorrhage, if there is an increase in focal symptoms and the appearance of signs of intracranial hypertension.
Treatment of subdural hemorrhage (acute) non-traumatic
- Maintenance of vital body functions, antihypertensive drugs, analgesics, calcium channel antagonists, dehydration, anticonvulsants.
- Question about surgical evacuation of hemorrhage (removal or stereotactic drainage of the hematoma).
- Secondary prevention.
Treatment is prescribed only after confirmation of the diagnosis by a medical specialist.
Essential drugs
There are contraindications. Specialist consultation is required.
- Mannitol (diuretic, decongestant). Dosage regimen: intravenous, slow stream or drip. Therapeutic dose is 1-1.5 g/kg body weight, prophylactic dose is 0.5 g/kg. The daily dose should not exceed 140-180 g.
- Furosemide (diuretic). Dosage regimen: intramuscularly or intravenously (slow stream) 20-60 mg 1-2 times a day, if necessary, the dose can be increased to 120 mg. The drug is administered for 7-10 days or more, and then the drug is taken orally.
- Ketoprofen (analgesic). Dosage regimen: orally, during meals; tablets 100 mg 3 times a day or 150 mg/day. (retard) with an interval of 12 hours. Capsules - 50 mg in the morning and afternoon, 100 mg in the evening.
- Carbamazepine (anticonvulsant). Dosage regimen: treatment begins with a dose of 0.1 g orally 2 times a day. Then the daily dose is gradually increased by 1/2-1 tablet. to minimally effective (0.4 g per day). It is not recommended to exceed a dose of more than 1200 mg/day.
- Nifedipine (calcium channel blocker, antihypertensive drug). Dosage regimen: intravenous drip, infusion rate should be 0.6-1.2 mg/h; the maximum daily dose is 30 mg, treatment period is 2-3 days. To continue therapy, it is advisable to switch to long-acting oral forms.