Story
In 1841, the English pediatrician William James West (1793–1848) wrote a letter to the editor-in-chief of the British journal The Lancet, where it was published. The letter was entitled: “On the specific form of infantile paroxysms.” William's son suffered from an unknown illness from the age of four months.
In the letter, Dr. West described his son’s seizures as “tilts.” The child bowed his head to his knees, and then his body completely relaxed. The attack could last up to 2-3 minutes and include up to 20 “tilts”, the intervals between them lasting only a few seconds. The doctor observed such attacks in the boy up to 3 times a day. In his letter, the pediatrician asked his colleagues for help. At the time of writing the letter, the boy was about a year old, and he could no longer acquire new skills and did not know how to move his limbs, never cried or laughed, looked indifferent, could not support his body in an upright position or hold his head on his own. By 11 months, the boy’s seizures began to resemble generalized tonic ones.
Over the next 100 years, epileptologists described syndromes similar to those described by West in children, and by the middle of the last century, about 70 similar cases had accumulated in the world literature. In the early 60s, neurologists first described the EEG pattern in children with paroxysms: hypsarrhythmia, that is, erratic high-amplitude asynchronous spikes and slow-wave activity. In 1964, the term “West syndrome” first appeared.
So what is this disease? West syndrome (WS) is an epileptic encephalopathy in children, manifested by a triad:
- Infantile spasms (IS). These are short, strong contractions of the muscles connecting the head to the spine and the muscles located along the spine (flexor, extensor, or mixed).
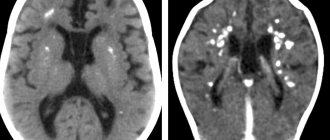
- Hypsarrhythmia - interictal changes on the EEG.
- Progressive impairment of cognitive, behavioral and neurological functions.
SV occurs in 2–6 cases per 10,000 newborns and accounts for up to 9% of epileptic syndromes in early childhood. Boys are more likely to suffer from West syndrome - up to 60% of the total number of patients.
Forms
Officially, SV is divided into symptomatic (up to 85%), as well as cryptogenic and idiopathic forms (together up to 20%). But from a clinical point of view, the disease has only 2 forms, since there are practically no differences between the cryptogenic and idiopathic forms. The symptomatic form of West syndrome includes cases of the disease against the background of existing brain pathology or developmental disorders. Half of the children with the symptomatic form had a history of complicated intrauterine conditions: infections, metabolic disorders, genetic and chromosomal defects (Down syndrome, etc.), as well as impaired intrauterine circulation in the mother. Pathology of the birth period is less common. These are hypoxic-ischemic brain damage, trauma and other complications during childbirth. Postnatal causes of WS include infections, trauma, hypoxic-ischemic strokes, and tumors.
The cryptogenic, or idiopathic, form of the disease is diagnosed in children with West syndrome epilepsy for no apparent reason, with normal psychomotor development and without brain damage before the onset of the disease. This is a more favorable form of SV.
The pathogenesis of West syndrome is currently unknown. Patients have a shortened REM sleep phase (rapid eye movement phase), during which the EEG normalizes and the frequency of spasms decreases. In this regard, there is a version that with WS, dysfunction of serotonergic neurons involved in the formation of sleep cycles occurs in the brain stem. There are other hypotheses that involve genetic and immune disorders in young patients.
Clinical picture
Most often, the syndrome debuts in children aged 4–6 months, and earlier symptoms are an unfavorable prognostic factor. Infantile spasms of West syndrome can occur with high frequency and be extremely varied - flexion of the body, vertical movements of the eyeballs, or eye movements similar to nystagmus, as well as “throwing up” of the arms like an oriental greeting, etc. One spasm lasts a fraction of a second, spasms grouped in series - up to 50 attacks in a series, the number of episodes per day - from one to several dozen. Often attacks develop upon awakening and falling asleep, and may be accompanied by moving the head or eyes to the side. Only half of the body may be involved in the spasm. The appearance of epilepsy attacks means a stop in the baby’s psychomotor development, and often a regression of acquired skills. In 1–2% of cases, spontaneous self-healing is possible.
Appeal to German medicine
Anna (patient’s mother): “My husband and I realized that wasting time was unacceptable for us. I studied a lot of information about the treatment of epilepsy. And in the end we decided to go to Germany.
On the Internet, after reviewing many offers for the treatment of epilepsy, I found the company GLORISMED, which we are now incredibly happy about. After the first request, we were contacted. What we really liked was that they took our case to work right away. After that, we called GLORISMED employees every day, sent them the necessary medical documents, which immediately went to German doctors.”
We received answers for the family from several German pediatric neurology clinics. Because Artem's case was quite severe, with daily epileptic seizures; Artem's parents chose a highly specialized center for the treatment of epilepsy in children located in Berlin.
Treatment
The most important goal of therapy is to completely stop or reduce the frequency of attacks and suppress hypsarrhythmia, which makes the normal development of the child impossible. Antiepileptic drugs in this case are ineffective. So is there a cure for West syndrome?
In 1958, the most important work on epilepsy and the effectiveness of corticotropin administration for infantile spasms was published in the European Journal of Neurology (authors L. Sorel and AA Duchamp-Boyol). ACTH helped in 50–90% of cases, and the cryptogenic form responded better to treatment than the symptomatic form. In a large Finnish study from 1980, the fatal complication rate of corticotropin therapy was 5% and the incidence of serious adverse events was 37%. The high risk of complications and low effectiveness of corticotropin in the symptomatic form of WS led to the need for further search for drugs to relieve spasms.
Other hormonal agents are now used: prednisolone, dexamethasone and tetracosactide. The latter drug is a synthetic polypeptide that has the properties of endogenous corticotropin and produces fewer complications than corticotropin itself. Over the past 20 years, the antiepileptic drug vigabatrin has proven itself. Susceptibility to therapy is 23–68%. The optimal dose and duration of treatment have not yet been determined for either vigabatrin or corticotropin and tetracosactide.
In addition, valproate and benzodiazepines are prescribed in the treatment of West syndrome. However, the complete disappearance of infantile spasms with these drugs occurs later than with treatment with steroids and vigabatrin. For a localized focus of epileptoid activity, surgical treatment is possible, but it is not effective in all cases.
The dynamics must be assessed by EEG monitoring, since during therapy, spasms can become subclinical, which are difficult to recognize without an EEG. In remission (a month without attacks), hypsarrhythmia may completely disappear, replaced by a normal EEG. But in 23–50% of cases of West syndrome, the prognosis is not very good - the disease transforms into other forms of epilepsy, which sometimes can only manifest themselves during puberty.
Drug treatment for epilepsy in Berlin
Anna (patient’s mother): “In a German clinic, Artem underwent an MRI of the brain, the conclusion of which was very different from the one in Kazan. They did a CSF (cerebrospinal fluid) analysis, an EEG and a number of other examinations. Based on the diagnostic results, the diagnosis of “infantile spasms” was confirmed and drug therapy was recommended.
The selection of medications began right at the clinic. Every day in the morning our attending physician came - a wonderful specialist, the head physician of the center for the treatment of childhood epilepsy. He learned the news, inquired about his health and adjusted the treatment.
Every three days, blood and urine were taken from my son to analyze the effectiveness and adjust the treatment. If in Russia Artyom could be kept on one drug for months, which in principle was not suitable for the child, then in the German clinic there is a completely different approach - a drug is selected with regular assessment of effectiveness based on laboratory tests.
During the first stage of epilepsy treatment in Germany, specialists increased the dosage of the prescribed medication within 2 weeks - and the attacks went away!”
A week after the child’s epileptic seizures stopped, Artem and his mother were discharged from the clinic. However, the family remained in Berlin for further outpatient monitoring in a German clinic.
Forecast
Since William West's letter to The Lancet, the prognosis for Westies has undoubtedly improved, but remains extremely grave. Unfortunately, the mortality rate from the disease itself or complications of its treatment during the first 3 years of life reaches 11% and over the past 40 years it has remained unchanged. Normal intellectual development is preserved in 9–28% of children. Normal or close to normal intelligence in cryptogenic and idiopathic forms is preserved more often - in 38-78% of cases, whereas in the symptomatic form - only in 2-18% of children. The prognosis of each child with West syndrome is extremely individual - the quality and length of life depends both on the form of the disease itself and on the timeliness and effectiveness of treatment.
Sources
- Kholin A. A., Mukhin K. Yu. West syndrome. Etiology, electro-clinical characteristics and differential diagnosis // Mukhin K. Yu., Petrukhin A. S., Kholin A. A. Epileptic encephalopathies and similar syndromes in children. M.: Art-Service Ltd (2011): 95–133.
- Gaponova O. V., Belousova E. D. Prognostic criteria for infantile spasms // Epilepsy and paroxysmal conditions 3.3 (2011).
- Temin P. A. et al. Infantile spasms and West syndrome // Diagnosis and treatment of epilepsy in children. M.: Mozhaisk-Terra. (1997): 287–354.
Medical Internet conferences
Relevance. West syndrome is a common (9% of all forms of epilepsy in children), disabling age-dependent epileptic syndrome in young children. Since the use of hormonal drugs (especially adrenocorticotropic hormone) in the treatment of West syndrome, it has become possible to quickly and completely relieve drug-resistant infantile spasms, but many clinicians are very reserved about hormonal treatment due to severe side effects. The emergence in recent decades of a number of new antiepileptic drugs has made it possible to use them in clinical practice for the treatment of West syndrome.
However, the numerous studies currently available on the effectiveness and safety of pharmacotherapy for West syndrome are of limited value due to the small number of patients, short follow-up period, lack of standardized treatment regimens, and lack of comparative analysis of the effectiveness of treatment for West syndrome during long-term follow-up.
Purpose of the study: retrospective assessment of long-term results of combination therapy for West syndrome including tetracosactide in comparison with other antiepileptic drugs (AEDs).
Material and methods. The study included 150 children with a confirmed diagnosis of West syndrome who received treatment at Children's Hospital No. 8 in Kazan in 2000-2015. Risk ratios (RR) and their confidence intervals (CI) were calculated using the Revman 5.0 Software program.
Results . All children with West syndrome are divided into 2 groups: group I - children who received tetracosactide in combination with other antiepileptic drugs as therapy - 90 people (60% of the total number of patients); group II – children who received any type of antiepileptic drugs, excluding tetracosactide – 60 people (40% of the total number of patients). Children in both groups were comparable in age, gender, neurological status, and severity of the disease. Long-term treatment results (favorable outcome - complete clinical remission lasting 3 years) did not differ significantly in both groups: 59 out of 90 patients (66%) in group I and 37 out of 60 patients (62%) in group II. The hazard ratio for long-term outcomes was RR=1.12; 95% CI [0.88 – 1.42], P=0.37.
Conclusion. Long-term treatment outcomes (with follow-up of 3 or more years) in children treated with tetracosactide and children treated with other antiepileptic drugs but not treated with tetracosactide for the treatment of West syndrome are comparable.