What are the features in the development of the nervous system of children?
At the time of birth, the baby's brain weight is one tenth of his body weight.
By nine months, the brain mass doubles. By the age of three it triples. The mass of the adult human brain is 1/40 of the body mass. It turns out that per kilogram of a newborn’s body weight there is approximately 109 grams of brain matter, and in an adult it is only 20-25 grams. During the prenatal period, the parts of the brain are formed from five brain vesicles. But by the time a child is born, brain formation is not yet complete. There are certain age-related features of the anatomy of the central nervous system:
- The convolutions of the cerebral hemispheres and the large grooves between these convolutions are small in height and also in depth. The number of small grooves is small. But their number increases in the first months of life;
- The frontal lobe is small and the occipital lobe is large compared to the same parts of the adult brain;
- Poor development of the cerebellum. Its hemispheres are small, the bark is thin, the furrows are superficial;
- Relatively large volume of the lateral ventricles of the brain.
At the very beginning of life, the gray matter of the baby’s brain is still poorly demarcated from the white matter. Complete differentiation of the cortex ends by school age. Only by the age of eight years does the cerebral cortex of a little person become similar in macro- and microscopic structure to the adult cortex.
Phylogenetically, early structures are better formed at the time of birth. The nuclei of the hypothalamus, medulla oblongata and spinal cord in the anatomical and functional state are more mature than the cerebral cortex, pyramidal tracts and striatum. Due to these factors, at the time of birth, life-sustaining activity is regulated at the subcortical level.
Children under one year old retain some reflexes, which, as they grow older, lose their significance and are reduced. For example, the hand-mouth reflex provides nutritional needs in the first months of life. And the automatic walking reflex, which manifests itself even in the prenatal period of development, prepares the baby for future upright walking. Subsequently, conditioned reflexes are formed, which will help the child adapt to a new environment and evaluate changing environmental conditions.
During early childhood, stable conditional connections of the emerging personality with society are formed. Children learn extremely quickly.
Over the years, the rate of formation of cognitive skills decreases exponentially. And those skills and behavior patterns that were acquired before the age of three remain for life.
Before the beginning of the second month of life, the baby develops several elementary conditioned reflexes. And by the end of the third month, it becomes possible to form complex, differentiated reflexes. This indicates the rapid development of the analyzing function of the cerebral cortex.
A newborn cannot yet differentiate signals coming from different sense organs. During this period, the child perceives the world in a generalized way. And only after two months of age does he begin to highlight certain aspects of his environment (mother, toys, food).
With the growth and development of a little person, many millions of nerve cells - neurons - die. At the same time, the formation of interneuron connections occurs. Memory develops with this process.
The younger the child, the faster the development of the nervous system occurs. The most intensive period of development is the first three months of a baby’s life.
The blood supply to the brain in children is better, thanks to which the organ is provided with an abundant supply of oxygen and glucose. But in children of the first year of life, venous outflow through diploic veins (as in adults) is difficult. These veins are finally formed only when the fontanelles close. In addition, the blood-brain barrier is fully formed by the age of three. Therefore, the brain of children at this age is especially susceptible to intoxicating factors (neurotoxicosis).
From the age of two, the child’s brain is already mature enough to form the second signal system - speech. The main contribution to the development of linguistic skills comes from the child’s communication with adults: parents, relatives, and educators.
Lesions of the central nervous system: at what stages of pregnancy?
Damage to the central nervous system in a child occurs in two ways - in utero or during childbirth.
If developmental abnormalities occur in the fetus during the embryonic stage of intrauterine development, they often turn into defects that are incompatible with life, or are extremely severe and cannot be treated or corrected. If a damaging effect was exerted on the fetus after the eighth week of pregnancy , this will not affect the child in the form of gross deformity, but may well cause minor deviations that will have to be treated after birth. The negative impact on the fetus in the later stages - after the twenty-eighth week of pregnancy - will not manifest itself in the form of defects at all, but can become a catalyst for the occurrence of diseases in a normally formed child.
It is very difficult to predict which specific negative factor and at what stage of pregnancy will cause irreparable damage to the fetus. Therefore, the expectant mother needs to be extremely careful and monitor her health even before the moment of conception. Preparing for pregnancy is an important stage of family planning, because the child’s health can be affected by both the bad habits of the mother and her chronic diseases, hard work and unhealthy psychological state.
How exactly he is born is also important for the child’s future life. It is at the moment of birth that there is a danger of damage in the second way - intranatally. Any incorrect intervention or, conversely, lack of timely assistance is highly likely to have a negative impact on the baby. At risk are premature birth, as well as birth at the scheduled time, but rapid or, conversely, protracted.
The main causes of central nervous system damage in newborns are oxygen starvation, which leads to hypoxia, and birth trauma. Less obvious and diagnosable causes are less common: intrauterine infections, hemolytic disease of the newborn, malformations of the brain and spinal cord, hereditary metabolic disorders or chromosomal pathology.
Doctors identify several syndromes of central nervous system pathology in newborns.
How a child's personality is formed
The formation of personality is a complex and multi-stage process in which complex connections of a person as an individual with the objective world are naturally formed. As we have already said, according to Locke’s theory of tabula rasa, our psyche (from psychos - soul) is a “blank slate”. And in the process of life, everything that a person encounters leaves its imprint on this board. In childhood, these traces are most vivid.
In order for a child to develop properly, he needs a clear daily routine - a regime. The baby is specially and arbitrarily taught good and bad skills. Parents must create comfortable conditions so that speech, targeted motor activity, and proper physical and mental development can be formed.
There are several approaches to describing the stages of personality development. Not all of them are clear and unambiguous.
For example, according to Freud’s theory of mental development of children, a child goes through several stages in his development:
- oral;
- anal;
- phallic;
- latent;
- genital
But as some of the most suitable, we can highlight the stages of “birth of personality” according to Leontiev:
- The first “birth” of personality is in preschool age. At this time, the child first correlates personal motives and needs with social rules. And submits to these social demands;
- During adolescence, the second “birth” of the personality occurs. It is directly related to the quality of education. What was invested in the child over the previous years of development is born in the form of his almost formed personality. The little man is aware of his motives and can prefer or subordinate them. Self-leadership and self-awareness emerge. Because of this, the child begins to bear criminal responsibility and be responsible for certain offenses according to the law.
From the point of view of this theory of mental development, the child’s personality experiences two crisis moments: the first in preschool age and the second in adolescence. However, the concept of this theory does not describe mental development in infancy. And this is also important for a holistic understanding of everything that can happen to a growing organism. Because the foundations for personality formation are laid when the baby doesn’t even know how to walk.
Theories of mental development describe ideal sequential stages through which a child should pass in due course.
Aspects that are necessary for the successful formation of a healthy personality:
- Confidence. This is the first personal quality that should be taught to a child. The child must learn to distinguish between those situations in which he can trust unconditionally, and those in which he should be more attentive to the words and actions of others.
- Safety. During infancy, children should not be exposed to extreme situations. The only thing that is required for them in this period of life is to be in a calm and safe environment with loving parents.
- Initiative. You need to praise your child for good deeds, encouraging him to always do the right thing. Often parents forget to do this (although they always practice punishment).
How to assess a child’s neuropsychological development
The individuality of each baby is undeniable. But the pace of development is different for all children. A child may acquire certain skills earlier than normal, while others later. Be that as it may, the growth and maturation of the individual must be adequate to the age, gender, and psychological characteristics of the little person. At the same time, the harmonious development of the neuropsychic sphere also plays an important role.
Developmental delay forces parents to think about possible causes. Some skills may be ahead of age standards, while others may not reach the standards. But if the baby is lagging behind in several respects, parents should think about whether they are doing everything right in raising the heir.
Help with mental development disorders in children and adolescents at the ROSA clinic
- Experienced specialists: psychologist, neuropsychologist, child neurologist, child psychiatrist, massage therapist and rehabilitation specialist.
- The clinic has its own hospital, an outpatient department and a functional diagnostics laboratory, where studies of the nervous system and mental sphere are carried out.
- We work around the clock.
- Possibility of comprehensive assistance: from psychological support and correction to drug treatment.
- Psychological support for family members and relatives.
- Make an appointment upon first request at a convenient time.
Conditioned reflex activity of children, development of emotions and forms of communication
Conditioned reflex activity begins to form immediately after birth. The crying baby is picked up, and he becomes silent and makes exploring movements with his head, anticipating feeding. At first, reflexes form slowly and with difficulty. With age, the concentration of excitation develops, or the irradiation of reflexes begins. As the child grows and develops, from about the 2nd-3rd week, differentiation of conditioned reflexes occurs. In a 2-3 month old child, a fairly pronounced differentiation of conditioned reflex activity is observed. And by 6 months, children can develop reflexes from all sensory organs. During the second year of life, the child’s mechanisms for the formation of conditioned reflexes are further improved.
At 2-3 weeks, while sucking, after taking a break to rest, the baby carefully examines the mother’s face and feels the breast or bottle from which he is fed. By the end of the 1st month of life, the child’s interest in the mother increases even more and manifests itself outside of meals. At 6 weeks, the mother's approach makes the baby smile. From the 9th to the 12th week of life, hearing is formed, which is clearly manifested when the child communicates with his mother. General motor excitement is observed.
By 4-5 months, the approach of a stranger causes the noise to stop, and the child carefully examines him. Then either general excitement appears in the form of joyful emotions, or as a result of negative emotions - crying. At 5 months, the child already recognizes his mother among strangers and reacts differently to the disappearance or appearance of his mother. By 6-7 months, children begin to develop active cognitive activity. While awake, the child manipulates toys; often a negative reaction to a stranger is suppressed by the manifestation of a new toy. Sensory speech is formed, i.e. understanding the words spoken by adults. After 9 months there is a whole range of emotions. Contact with strangers usually causes a negative reaction, but it quickly becomes differentiated. The child develops timidity and shyness. But contact with others is established thanks to interest in new people, objects, and manipulations. After 9 months, the child’s sensory speech develops even more; it is already used to organize his activities. The formation of motor speech also dates back to this time, i.e. pronouncing individual words.
Speech development
The formation of speech is a stage in the formation of human personality. Special brain structures are responsible for a person’s ability to articulate. But speech development occurs only when the child communicates with another person, for example, with his mother.
There are several stages in the development of speech.
Preparatory stage . The development of humming and babbling begins at 2-4 months.
The stage of the emergence of sensory speech . This concept means the child’s ability to compare and associate a word with a specific object or image. At 7-8 months, the child, in response to the questions: “Where is mom?”, “Where is the kitty?”, begins to look for an object with his eyes and fix his gaze on it. Intonations that have a certain coloring can be enriched: pleasure, displeasure, joy, fear. By the age of one year, a child already has a vocabulary of 10-12 words. The child knows the names of many objects, knows the word “no”, and fulfills a number of requests.
Stage of emergence of motor speech . The child speaks his first words at 10-11 months. The first words are built from simple syllables (ma-ma, pa-pa, dyad-dya). A child's language is formed: a dog - “aw-aw”, a cat - “kitty-kitty”, etc. In the second year of life, the child’s vocabulary expands to 30-40 words. By the end of the second year, the child begins to speak in sentences. By the age of three, the concept of “I” appears in speech. More often than not, girls master motor speech earlier than boys.
In children from the newborn period, a mechanism of instant contact - imprinting - is formed. This mechanism, in turn, is associated with the formation of the child’s neuropsychic development.
Maternal upbringing very quickly creates a sense of security in a child, and breastfeeding creates a feeling of security, comfort, and warmth. The mother is an indispensable person for the child: she forms his ideas about the world around him, about the relationship between people. In turn, communication with peers (when the child begins to walk) forms the concept of social relationships, camaraderie, and inhibits or enhances the feeling of aggressiveness. The father also plays a large role in raising a child. His participation is necessary for the normal building of relationships with peers and adults, the formation of independence and responsibility for a particular matter, and a course of action.
Dream
For full development, a child needs proper sleep. In newborns, sleep is polyphasic. During the day, the child falls asleep from five to 11 times, not distinguishing day from night. By the end of the 1st month of life, the rhythm of sleep is established. Night sleep begins to prevail over daytime sleep. Hidden elements of polyphase persist even in adults. On average, the need for nighttime sleep decreases over the years.
A decrease in the total duration of sleep in children occurs due to daytime sleep. By the end of the first year of life, children fall asleep once or twice. By the age of 1-1.5 years, the duration of daytime sleep is 2.5 hours. After four years, not all children have daytime sleep, although it is advisable to maintain it until the age of six.
Sleep is organized cyclically, i.e. the slow-wave sleep phase ends with the REM sleep phase. Sleep cycles change several times during the night.
In infancy, sleep problems usually do not occur. At the age of one and a half years, the child begins to fall asleep more slowly, so he himself chooses techniques that promote falling asleep. It is necessary to create a familiar environment and behavior pattern before bedtime.
Muscle tone disorders
Movement disorder syndrome - a pathology of motor activity - is diagnosed in almost all children with intrauterine abnormalities in the development of the central nervous system. Only the severity and level of damage varies.
When making a diagnosis, the pediatrician must understand what the zone and location of the lesion is, whether there is a problem in the functioning of the brain or spinal cord. This is a fundamentally important question, since treatment methods differ radically depending on the identified pathology. Also of great importance for making a diagnosis is a correct assessment of the tone of various muscle groups.
Impaired tone in various muscle groups leads to a delay in the appearance of motor skills in the baby: for example, the child later begins to grasp objects with the whole hand, finger movements are formed slowly and require additional training, the child gets up on his feet later, and the cross of the lower extremities prevents the formation of correct walking.
Fortunately, this syndrome is treatable - in most children, thanks to proper treatment, there is a decrease in muscle tone in the legs, and the child begins to walk well. Only a high arch of the foot may remain as a memory of the disease. This does not interfere with normal life, and the only difficulty remains choosing comfortable and well-fitting shoes.
What are unconditioned reflexes?
The unconditioned reflexes of a newborn are, first of all, nature-programmed responses and protective reactions to external stimuli that are necessary for the child’s life. Without these reflexes, the child would not be able to find the nipple and take the breast, or carry out the correct sucking movements. Almost all unconditioned reflexes are formed by the time of birth and persist from 1.5 to 4–5 months of a child’s life, giving way to the development of conscious motor skills. Longer preservation of a newborn's reflexes prevents the formation of these skills and is a manifestation of pathology.
So what unconditioned reflexes are characteristic of a newborn? Let's list
- search reflex (when stroking the corner of the mouth, the child turns his head in this direction and tries to touch the stimulus with his tongue);
- sucking reflex (when any object enters the child’s mouth, the baby grabs it with his lips and begins rhythmic sucking movements);
- Babkin's palm-oral reflex (when pressing on the palm, the child opens his mouth);
- Moro reflex (when hitting the surface on which the child is lying, he first spreads his arms to the sides, and then makes a grasping movement and brings his arms to the body);
- grasping reflex (when pressing on the palm, the child squeezes his fingers);
- support reflex (when the child’s legs touch the support, he first presses them in, and then straightens them and leans on the surface);
- automatic gait reflex (in an upright position with the body slightly tilted, the child begins to step with his feet on the table surface);
- protective reflex (when the baby is placed on his stomach, he turns his head to the side);
- Bauer's crawling reflex (in a position lying on his stomach with his feet resting, the child begins to crawl forward, alternately moving his arms and legs).
Assessing the state of the newborn's unconditioned reflexes is one of the main points of examining the newborn, especially if this examination is carried out by a neurologist. Changes in these reflexes, their weakening or absence, rapid exhaustion (the first time the reflex can be evoked, with subsequent irritations it is expressed less and less) can be observed with prematurity or immaturity, with birth damage to the nervous system, in the presence of a general infectious disease or other pathology of the period newborns.
First skills
Nervous system of the newborn As mentioned above, by the time the baby is born, the spinal cord is the most mature. The brain, as a more complex structure, by the end of the prenatal period has not yet completed its development, not only morphologically (the formation of convolutions of the cerebral cortex continues, the ratio of the white and gray matter of the brain changes), but also functionally. So, a very important point is that the number of nerve cells in the cerebral cortex of a newborn child and an adult is the same. But in a newborn, these cells are still immature in their structure; they have very few processes connecting the cortical cells with each other, and it is the presence of these connections that determines many functions of higher nervous activity, such as memory, emotions, and skills.
However, the development of the cerebral cortex occurs quite quickly, and we notice this by how quickly the baby changes. A newly born baby is not yet able to hold his head and fix his gaze, he can only distinguish bright light and sees his mother’s face as a blurry spot, all his movements are chaotic and unconscious. But a month passes and the child makes significant progress in his development. First of all, all senses are improved.
In the first month of a baby’s life, the movements of his eyeballs are not yet coordinated; from time to time, convergent or divergent strabismus is noted. But by the fifth week, the child already focuses his gaze quite well on a specific object, thanks to which he can clearly see surrounding objects and faces. By this age, he begins to understand that all the positive emotions in his life are associated with the face he sees most often - saturation, warmth, comfort. Most often this is the face of his mother. Accordingly, the baby sees a direct connection between the appearance of the mother’s face and the appearance of comfort, saturation and warmth. This becomes the beginning of the formation of positive emotions.
The hearing organ functions already in the last weeks of intrauterine development. The fetus may experience increased heart rate in response to sharp sounds and... on the contrary, the normalization of the heartbeat and bioelectrical activity of the brain when listening to melodic music. In a newborn, the reaction to sound is in the nature of an indicative reflex: in response to a sound stimulus, the child can close his eyes, open his mouth slightly, shudder and hold his breath.
The taste organ is also fully formed at the time of birth: the newborn is good at distinguishing sweet from sour, bitter or salty. When a sweet substance enters a child's mouth, he begins to make sucking movements. Bitter, sour or salty substances cause a grimace of displeasure, closing the eyes, and crying.
By the end of the first month of life, the child acquires skills such as the ability to follow a bright moving object with his eyes, recognize his mother and smile at her. respond to the mother's voice. His daily routine is still dominated by periods of sleep, while during wakefulness - negative emotions: in this way, the baby signals hunger, discomfort associated with overexcitation or fatigue, and wet diapers. But gradually, periods of calm wakefulness begin to appear in his emotional state, when the baby tries to look at surrounding objects, studies his mother’s face or listens to her voice. All this is the beginning of the formation of his psyche, his higher nervous activity, which becomes possible thanks to the rapid development of the cerebral cortex and sensory organs.
Major events in newborn brain development
In a newborn child, less intensely than in a fetus, new nerve cells are born and move to their destinations in the deep structures and cortex of the brain. Due to this, the volume of gray matter in the brain continues to increase in newborns. The occipital and parietal areas of the cortex, which take part in the processing of visual and tactile information, increase most intensively. Contacts between nerve cells are very actively formed. This is necessary for the formation of complex brain systems capable of processing various information. Some nerve cells and their connections die. This is a normal process, the purpose of which is to get rid of defective and unused nerve elements.
The long endings of nerve cells (axons) are actively covered with a special substance - myelin, due to which the speed of nerve impulse transmission along the nerve increases. Myelin forms the basis of the white matter of the brain. The sensory pathways (nerves going from the receptors of the eye, ear, skin, etc. to the brain) are the first to myelinate, then the motor nerves. Deep structures myelinate earlier than the cerebral cortex. At the level of deep structures, the primary processing of all information coming to a person from outside and inside occurs, and many movements are regulated. Deep structures are directly involved in maintaining motivation, emotions, level of alertness and important types of memory.
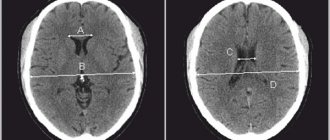
At 2-4 weeks of life, the baby's brain size is 36% of the adult's brain size.
Table. Main indicators of psychomotor development in the period from birth to 1 month [2].
| Age | Visual orientation reactions | Auditory orientation reactions | Emotions and social behavior | Hand movement / Actions with objects | General movements | Speech |
| 10 days | Keeps a moving object in the field of view (step tracking) | Startles and blinks when there is a sharp sound | Grasp reflex | |||
| 18-20 days | Keeps a stationary object (adult's face) in sight | If he was crying, he calms down (stops crying) at a sharp sound | The first signs of a “revival complex” may appear - a reciprocal smile, motor excitement in the presence of an adult | |||
| 1 month | Focuses his gaze on a stationary object, on the face of an adult speaking to him. Smooth tracking of a moving object appears | Listens to the sound, to the voice of an adult | Revival complex in response to an adult’s appeal | Grabs the other hand with one hand. | Makes erratic movements with limbs brought to the body. Can't hold head upright. Lying on his stomach, he tries to raise and hold his head. | Makes individual sounds in response to conversations with him |
First smile
A certain semblance of a smile can be observed in the baby in the first days after birth (in a dream, after eating). But this grimace cannot be called a smile. At the moment when the movements of the eyeballs are already sufficiently well coordinated and the baby can focus his gaze on his mother’s face, when a sufficient number of connections between nerve cells have been formed in the cortex of his brain that determine the ability to remember, a true miracle occurs - the baby smiles meaningfully for the first time. This usually occurs around 1 month of age. Nothing can compare with the joy of a mother who sees a smile on her child’s face for the first time!
Features of the nervous system of a newborn
In the first days of a newborn's life, the excitability of his nervous system is significantly reduced. This is necessary so that the abundance of irritating factors, sudden changes in environmental conditions, and intense stress during childbirth do not cause damage to the nervous system. During the first week of a child's life, excitability gradually increases.
One of the features of the nervous system of a newborn is that its efficiency is low: fatigue and exhaustion of nervous functions occurs much faster than in adults, so children cannot endure monotonous irritations for a long time, for example, they quickly cease to be interested in a rattle and need a change of impressions, for example, conversations with mom, soft music. But these impressions should not be excessive, since their abundance and great intensity can also cause fatigue and overstimulation. The nervous system of a newborn is more sensitive to a lack of oxygen due to the high level of metabolic processes, which require high blood oxygen saturation. This is associated with the vulnerability of the nervous system of the fetus and newborn to hypoxia (lack of oxygen) during childbirth and during the first days after birth.
During intrauterine development, the fetal muscles are constantly in a state of flexion, which ensures the characteristic fetal position. After the birth of a child, the predominance of the tone of the flexor muscles remains in his skeletal muscles, that is, the baby constantly strives to occupy the so-called fetal position, but the activity of the motor centers that provide the tone of the extensor muscles gradually increases. Thanks to this, active movements become possible.
All movements of the fetus and newborn child are in the nature of reflexes and extend to the entire body. At this age, the baby is not yet able to carry out purposeful movements - his movements are chaotic and are a response to some kind of irritation.
Another very interesting and important feature of the function of the nervous system of a newborn is that all his behavior is subject to food dominance: if the child is hungry, his reflexes are inhibited, and his excitability is further reduced. He needs only one thing - to satisfy his immediate need for food.
Particular attention should be paid to the peculiarities of the nervous system of a newborn, associated with incomplete myelination of nerve fibers. Myelination is the process of formation of a special sheath covering the nerve endings. This membrane plays the role of a kind of insulation, ensuring the spread of a nerve impulse from a nerve cell to an organ or muscle, but not to a muscle group. Since by the time of birth not all nerve endings have a myelin sheath, any nerve impulse passing through a nerve bundle, which combines many nerve fibers, spreads to neighboring fibers. This is due to the fact that any excitation becomes more or less general, affecting neighboring muscles or organs. So, if a newborn experiences discomfort or pain, this signal is “transmitted” to the entire body. This is one of the reasons for such pronounced anxiety in a child due to intestinal colic: abdominal pain spreads to neighboring organs.
A striking example of the generalization of a nerve impulse is the unconditioned reflexes of a newborn. For example, when running a finger along the spine, the body is straightened, arms and legs are bent, a cry is heard, and even sometimes urination occurs.
In the early stages of development in a growing organism, the nerve centers have a high degree of ability to compensate for adaptation. If the activity of any center is disrupted, its function is taken over by other parts of the brain or spinal cord. This ability helps restore some functions of victims as a result of an unfavorable course of the intrauterine period. This truly lucky ability of the brain makes it possible to use many of its reserve capabilities to ensure the proper development of the child.
Thus, the nervous system is small: by the time of birth, it is already largely formed, its structure practically does not differ from that of an adult, but those parts of it that are responsible for the highest and most complex activities are still very immature. Their maturation lasts throughout the first year of a child’s life.
Homo sapiens
Of course, all organs and systems are important and necessary for the functioning of the human body, but the nervous system stands apart among them, one might say, on a pedestal. It is this that makes a person a rational and thinking being. The main importance of the nervous system is to ensure the best adaptation of the body to the influence of the external environment and the implementation of its optimal response to this influence. That is why during the first year of a baby’s life, his nervous system undergoes greater changes than any other, developing literally by leaps and bounds.
Start
Of all the parts of the central nervous system, by the time intrauterine maturation is complete, the spinal cord is the most mature. Its growth is associated with the formation of pathways (nerves) connecting the brain with muscles, for example, limbs and other parts of the body and internal organs. The beginning of the functioning of these pathways is associated with the formation of the activity of the central nervous system, which determines the work of various muscle groups. This formation is facilitated by the fact that its development is directly stimulated by any irritation to which the fetus is exposed in the womb. Among them are skin irritations - contact of the skin with amniotic fluid, the walls of the uterus, irritation of joints and muscles during the motor activity of the fetus and irritation of the hearing organ (the fetus perceives speech sounds and other sounds that the mother hears, although for him they do not sound so loud, as for her).
The formation of reflex activity occurs in three stages:
- the stage of individual local movements (2-3 months of intrauterine development), when the fetus carries out simple limited movements in response to irritation;
- the stage of generalized responses (3-4th month of intrauterine development), characterized by the appearance of generalized uncoordinated reactions, when, in response to irritation of a separate part of the body, movements are made in the upper and lower extremities, neck and back;
- the stage of specialized reflex responses that give rise to the development of unconditioned reflexes in the newborn.
What are unconditioned reflexes?
The unconditioned reflexes of a newborn are, first of all, nature-programmed responses and protective reactions to external stimuli that are necessary for the child’s life. Without these reflexes, the child would not be able to find the nipple and take the breast, or carry out the correct sucking movements. Almost all unconditioned reflexes are formed by the time of birth and persist from 1.5 to 4 - 5 months of a child’s life, giving way to the development of conscious motor skills. Longer preservation of a newborn's reflexes prevents the formation of these skills and is a manifestation of pathology.
So what unconditioned reflexes are characteristic of a newborn? Let's list
- search reflex (when stroking the corner of the mouth, the child turns his head in this direction and tries to touch the stimulus with his tongue);
- sucking reflex (when any object enters the child’s mouth, the baby grabs it with his lips and begins rhythmic sucking movements);
- Babkin's palm-oral reflex (when pressing on the palm, the child opens his mouth);
- Moro reflex (when hitting the surface on which the child is lying, he first spreads his arms to the sides, and then makes a grasping movement and brings his arms to the body);
- grasping reflex (when pressing on the palm, the child squeezes his fingers);
- support reflex (when the child’s legs touch the support, he first presses them in, and then straightens them and leans on the surface);
- automatic gait reflex (in an upright position with the body slightly tilted, the child begins to step with his feet on the table surface);
- protective reflex (when the baby is placed on his stomach, he turns his head to the side);
- Bauer's crawling reflex (in a position lying on his stomach with his feet resting, the child begins to crawl forward, alternately moving his arms and legs).
Assessing the state of the newborn's unconditioned reflexes is one of the main points of examining the newborn, especially if this examination is carried out by a neurologist. Changes in these reflexes, their weakening or absence, rapid exhaustion (the first time the reflex can be evoked, with subsequent irritations it is expressed less and less) can be observed with prematurity or immaturity, with birth damage to the nervous system, in the presence of a general infectious disease or other pathology of the period newborns.
First skills
Nervous system of the newborn As mentioned above, by the time the baby is born, the spinal cord is the most mature. The brain, as a more complex structure, by the end of the prenatal period has not yet completed its development, not only morphologically (the formation of convolutions of the cerebral cortex continues, the ratio of the white and gray matter of the brain changes), but also functionally. So, a very important point is that the number of nerve cells in the cerebral cortex of a newborn child and an adult is the same. But in a newborn, these cells are still immature in their structure; they have very few processes connecting the cortical cells with each other, and it is the presence of these connections that determines many functions of higher nervous activity, such as memory, emotions, and skills.
However, the development of the cerebral cortex occurs quite quickly, and we notice this by how quickly the baby changes. A newly born baby is not yet able to hold his head and fix his gaze, he can only distinguish bright light and sees his mother’s face as a blurry spot, all his movements are chaotic and unconscious. But a month passes and the child makes significant progress in his development. First of all, all senses are improved.
In the first month of a baby’s life, the movements of his eyeballs are not yet coordinated; from time to time, convergent or divergent strabismus is noted. But by the fifth week, the child already focuses his gaze quite well on a specific object, thanks to which he can clearly see surrounding objects and faces. By this age, he begins to understand that all the positive emotions in his life are associated with the face he sees most often - saturation, warmth, comfort. Most often this is the face of his mother. Accordingly, the baby sees a direct connection between the appearance of the mother’s face and the appearance of comfort, saturation and warmth. This becomes the beginning of the formation of positive emotions.
The hearing organ functions already in the last weeks of intrauterine development. The fetus may experience increased heart rate in response to sharp sounds and... on the contrary, the normalization of the heartbeat and bioelectrical activity of the brain when listening to melodic music. In a newborn, the reaction to sound is in the nature of an indicative reflex: in response to a sound stimulus, the child can close his eyes, open his mouth slightly, shudder and hold his breath.
The taste organ is also fully formed at the time of birth: the newborn is good at distinguishing sweet from sour, bitter or salty. When a sweet substance enters a child's mouth, he begins to make sucking movements. Bitter, sour or salty substances cause a grimace of displeasure, closing the eyes, and crying.
By the end of the first month of life, the child acquires skills such as the ability to follow a bright moving object with his eyes, recognize his mother and smile at her. respond to the mother's voice. His daily routine is still dominated by periods of sleep, while during wakefulness - negative emotions: in this way, the baby signals hunger, discomfort associated with overexcitation or fatigue, and wet diapers. But gradually, periods of calm wakefulness begin to appear in his emotional state, when the baby tries to look at surrounding objects, studies his mother’s face or listens to her voice. All this is the beginning of the formation of his psyche, his higher nervous activity, which becomes possible thanks to the rapid development of the cerebral cortex and sensory organs.
First smile
A certain semblance of a smile can be observed in the baby in the first days after birth (in a dream, after eating). But this grimace cannot be called a smile. At the moment when the movements of the eyeballs are already sufficiently well coordinated and the baby can focus his gaze on his mother’s face, when a sufficient number of connections between nerve cells have been formed in the cortex of his brain that determine the ability to remember, a true miracle occurs - the baby smiles meaningfully for the first time. This usually occurs around 1 month of age. Nothing can compare with the joy of a mother who sees a smile on her child’s face for the first time!
Features of the nervous system of a newborn
In the first days of a newborn's life, the excitability of his nervous system is significantly reduced. This is necessary so that the abundance of irritating factors, sudden changes in environmental conditions, and intense stress during childbirth do not cause damage to the nervous system. During the first week of a child's life, excitability gradually increases.
One of the features of the nervous system of a newborn is that its efficiency is low: fatigue and exhaustion of nervous functions occurs much faster than in adults, so children cannot endure monotonous irritations for a long time, for example, they quickly cease to be interested in a rattle and need a change of impressions, for example, conversations with mom, soft music. But these impressions should not be excessive, since their abundance and great intensity can also cause fatigue and overstimulation. The nervous system of a newborn is more sensitive to a lack of oxygen due to the high level of metabolic processes, which require high blood oxygen saturation. This is associated with the vulnerability of the nervous system of the fetus and newborn to hypoxia (lack of oxygen) during childbirth and during the first days after birth.
During intrauterine development, the fetal muscles are constantly in a state of flexion, which ensures the characteristic fetal position. After the birth of a child, the predominance of the tone of the flexor muscles remains in his skeletal muscles, that is, the baby constantly strives to occupy the so-called fetal position, but the activity of the motor centers that provide the tone of the extensor muscles gradually increases. Thanks to this, active movements become possible.
All movements of the fetus and newborn child are in the nature of reflexes and extend to the entire body. At this age, the baby is not yet able to carry out purposeful movements - his movements are chaotic and are a response to some kind of irritation.
Another very interesting and important feature of the function of the nervous system of a newborn is that all his behavior is subject to food dominance: if the child is hungry, his reflexes are inhibited, and his excitability is further reduced. He needs only one thing - to satisfy his immediate need for food.
Particular attention should be paid to the peculiarities of the nervous system of a newborn, associated with incomplete myelination of nerve fibers. Myelination is the process of formation of a special sheath covering the nerve endings. This membrane plays the role of a kind of insulation, ensuring the spread of a nerve impulse from a nerve cell to an organ or muscle, but not to a muscle group. Since by the time of birth not all nerve endings have a myelin sheath, any nerve impulse passing through a nerve bundle, which combines many nerve fibers, spreads to neighboring fibers. This is due to the fact that any excitation becomes more or less general, affecting neighboring muscles or organs. So, if a newborn experiences discomfort or pain, this signal is “transmitted” to the entire body. This is one of the reasons for such pronounced anxiety in a child due to intestinal colic: abdominal pain spreads to neighboring organs.
A striking example of the generalization of a nerve impulse is the unconditioned reflexes of a newborn. For example, when running a finger along the spine, the body is straightened, arms and legs are bent, a cry is heard, and even sometimes urination occurs.
In the early stages of development in a growing organism, the nerve centers have a high degree of ability to compensate for adaptation. If the activity of any center is disrupted, its function is taken over by other parts of the brain or spinal cord. This ability helps restore some functions of victims as a result of an unfavorable course of the intrauterine period. This truly lucky ability of the brain makes it possible to use many of its reserve capabilities to ensure the proper development of the child.
Thus, the nervous system is small: by the time of birth, it is already largely formed, its structure practically does not differ from that of an adult, but those parts of it that are responsible for the highest and most complex activities are still very immature. Their maturation lasts throughout the first year of a child’s life.
How to teach a newborn different skills
Learning is a process that leads to permanent changes in behavior based on experience. Babies learn in different ways.
Most often, the learning process looks like the use of rewards and/or punishments. Reinforcement reinforces desired behavior, while negative reinforcement shows which response is undesirable.
For example, a child who sees that smiling attracts parental attention smiles more at his parents.
Mostly, newborns learn through observation and imitation of others.
For example, a baby learns to clap by watching and imitating its older brother. This form of learning is the fastest and most natural way for children to acquire new skills.
What can an adult do to promote a child's cognitive development?
It is important to try to eliminate obstacles that hinder free development. So, if a child does not develop one of the skills in a timely manner, it is necessary to check whether everything is in order with his muscle tone, reflexes, etc. This can be done by a neurologist. If an obstacle becomes obvious, it is important to eliminate it in a timely manner. In particular, when it comes to impaired muscle tone (muscle dystonia), therapeutic massage, physical therapy and visiting the pool are of great help. In some cases, drug treatment is required.
It is very important to create conditions conducive to development. By creating conditions we mean providing the child with the opportunity to realize his genetic program without restrictions. So, for example, you cannot keep a child in a playpen without allowing him to move around the apartment, on the grounds that there are dogs in the house and the floor is dirty. Enabling also means providing the child with an enriched sensory environment. Understanding the world in its diversity is what develops the child’s brain and forms the foundation of sensory experience that can form the basis for all subsequent cognitive development. The main tool that we are used to using to help a child get acquainted with this world is a toy, and a toy that develops the capabilities of movement and perception. A toy can be anything that can be grabbed, picked up, shaken, put in your mouth, or thrown. The main thing is that it is safe for the baby. Toys should be varied, differing from each other in texture (soft, hard, smooth, rough), shape, color, sound. The presence of small patterns or small elements in the toy does not matter. The child is not yet able to see them. We must not forget that in addition to toys, there are other means that stimulate the development of perception. These include different settings (walks in the forest and in the city), music and, of course, communication with the child from adults.
Treatment and rehabilitation of perinatal lesions of the nervous system in children in the first months of life
In recent decades, in connection with the achievements of the latest medical technologies (in vitro fertilization, prolongation of pathological pregnancy, neonatal resuscitation), the problem of improving the quality of life of children with perinatal pathology of the nervous system has become particularly relevant [1, 2, 3]. Significant disturbances: first of postnatal adaptation, then a decrease in the ability to assimilate social experience and, as a consequence, social maladjustment of the child - occur in the majority of children with severe lesions of the nervous system. According to leading neurologists [3], these lesions account for the bulk of the causes of childhood disability. In addition, children with mild forms of perinatal pathology in subsequent years often experience manifestations of minimal cerebral dysfunctions, which significantly complicate their learning and education [2]. Therefore, the problems of timely treatment and adequate rehabilitation of children with perinatal lesions attract the close attention of doctors of various specialties: pediatricians, neurologists, orthopedists, rehabilitation specialists, etc., as well as specialists in correctional pedagogy.
The basic methodological principles of rehabilitation of children with perinatal pathology of the central nervous system, developed over the past 10–12 years [4], can also form the basis for the treatment of these conditions, the objectives of which are both in the acute period and during rehabilitation, secondary prevention of delayed manifestations of the disease in essence same. Nevertheless, some neurologists understand rehabilitation in childhood as habilitation, i.e., the creation of opportunities for the progressive development of the child and the correction of gradually emerging developmental deviations [3]. Taking this into account, the general methodology of treatment and rehabilitation for perinatal brain damage is based on the following principles.
- Early start of correction. Optimally advanced (antenatal, intranatal, early postnatal) treatment.
- Individualization of treatment and rehabilitation effects - taking into account the nature and severity of the main and concomitant pathology, the degree of maturity of the child (gestational and post-conceptual age), individual constitutional and genetic characteristics. The use of protocols (formulas) for the management of newborns does not contradict an individual approach. Using “individual compensation potential” [3].
- An approach to a sick child from the standpoint of the integrity of the body, which involves the correction of not only and not so much neurological disorders as neurosomatic disorders [3, 5].
- Integrated use of various means of treatment and rehabilitation (pharmaceuticals, physical factors, aesthetic psychotherapy and conductive pedagogy).
- Stagedness and continuity in the rehabilitation of injured children, collegiality in prescribing therapeutic regimens and assessing their effectiveness.
- Humanization of diagnostic, treatment and rehabilitation procedures: in recent years, the extremely negative pathophysiological role of pain in newborns has been established [4, 6].
- Improving the environment (“environmental therapy”) and close interaction between doctors and the family of a sick child at all stages of treatment and rehabilitation [3, 4].
Each stage of providing care to a sick newborn and infant has its own leading tasks. Thus, at the first stage - in the maternity ward, intensive care ward and neonatal intensive care unit - in accordance with the order of the Ministry of Health of the Russian Federation No. 372 of 1995, the tasks of compensating for systemic disorders of vital functions - respiration, blood circulation, excretory function of the kidneys, energy balance and general metabolism.
At this stage, drug-instrumental therapy primarily involves correction of the acid-base state, hyper- or hypoglycemia, hypovolemia, arterial hypotension or hypertension, and cardiac output. According to indications, taking into account monitoring data and laboratory tests, osmotic and loop diuretics, antihemorrhagic, anticonvulsants are used (the drug of first choice is phenobarbital in a standard dose of up to 20 mg/kg body weight per day). The use of antioxidants and nootrophs (cerebroprotectors - piracetam, essentiale, GHB) at this stage is not always justified. Particular caution is necessary when prescribing vasoactive drugs: for example, some experts recommend instenon from the 4th day of life [3], while others talk about possible side effects of vascular drugs [5]. Adequate treatment in the early neonatal period (while creating the most gentle conditions for the child and thermal comfort) promotes adaptation processes of a sanogenetic nature and is the basis for subsequent rehabilitation.
Newborns not only with severe, but also with moderate manifestations of perinatal pathology of the central nervous system are transferred, as a rule, to the “second stage” department (department of pathology of newborns, department for premature infants). The objectives of this stage are further optimization of adaptation processes, treatment of concomitant (usually infectious-inflammatory) diseases and the beginning of rehabilitation itself, i.e. correction of neurological disorders. The third stage of rehabilitation includes specialized hospitals (department of early childhood neurology, rehabilitation center for low birth weight and premature babies, correction center), outpatient rehabilitation departments of children's clinics (inpatient replacement technologies). At all stages of rehabilitation of perinatally injured children, the active participation of the family of the sick child is necessary; according to indications, at the end of the first - beginning of the second year of life, it is possible to involve specialized preschool institutions (correction groups in nurseries and kindergartens, correction centers). At the second and third stages of rehabilitation, almost the same means and methods are used, although their choice depends on the individual pathokinesis of the disease and the effectiveness of correction at the previous stage.
In the practice of most doctors, pharmacotherapy for perinatal brain lesions takes a leading place, which is not always justified. In the last decade, in the context of the “pharmaceutical boom,” new drugs appear annually, which from the field of adult neurology, often without sufficient testing from the standpoint of evidence-based medicine, end up in the arsenal of drugs used by the neonatologist [5, 6, 7]. When prescribing a drug to a newborn, the doctor must take into account its possible immediate and long-term side effects (including the risk of sensitization), choose the least traumatic route of drug administration: if injections are necessary, provide pain relief with local anesthetics such as the EMLA patch or metabolites [4, 6] . To avoid iatrogenicity, it is necessary to take into account possible synergism or antagonism of pharmacological drugs (do not prescribe more than 3-4 drugs at the same time), strictly individually select dosages (principle of minimization, control of individual pharmacokinetics). Particular care is needed when choosing an algorithm for the treatment of very premature infants with extremely low body weight. One of the ways to prevent iatrogenism in neonatology is the use of homeopathic preparations [8], since they contain microdoses of mild plant and mineral substances. The mechanism of action of these drugs is not entirely clear (explanations are possible from the standpoint of Ukhtomsky’s theory of dominance or the theory of biological resonance), however, the chemical effectiveness of some of the homeopathic drugs in neonatology has been fully proven [4].
Pharmacological drugs used in the rehabilitation of both full-term and premature newborns can be conditionally divided into those used syndromously (symptomatic) and means of predominantly pathogenetic correction, although some drugs have both effects. Let's take a closer look at them.
Drug rehabilitation of children with perinatal lesions of the central nervous system - late neonatal period, beginning of the recovery period
Mainly syndromic (symptomatic) drugs: anticonvulsants: phenobarbital, GHB, droperidol, relanium, valproate - for seizures that cannot be controlled by other drugs and careful monitoring of liver functions and hematopoiesis; dehydration: diacarb (from 2–3 weeks of life, later in very premature infants), triampur, veroshpiron, homeopathic preparations (heliborus, apis, magnesia phosphorica), herbal teas - decoctions and infusions; sedatives (magnesium sulfate, herbal teas - decoctions and infusions, medicinal baths, Relanium, Radedorm, homeopathic medicines - Valerianahel, Nervohel, Viburkol), essential oils, aromatherapy (anise, chamomile, lavender); antispasmodics and prokinetics (for vegetative disorders): no-shpa, cerucal, riabal, motilium, homeopathic drugs (nuksvomika, gomacord, viburkol, hapel).
Pathogenetic agents: neuroprotectors (nootropics, nootrophs, inhibitors of neural apoptosis) - piracetam (WIS), Cortexin, Semax, Minisem, Cerebrolysin, Pantogam, gliatilin, glycine, amino acid composites, stem cells; vasoactive drugs (normalizers of general and cerebral hemodynamics) are prescribed in the absence of a threat of bleeding under Doppler ultrasound control: Cavinton, cinnarizine, Sermion, dimephosphone, quercetin, homeopathic drugs (Aesculus compositum, Traumeel); synaptic conduction modulators: mydocalm, dibazol; antioxidants and antihypoxants: tanakan, mexidol, tocopherol, soybean oil, kudesan, dimephosphon, biolan, actovegin; metabolites and multivitamin complexes: glycine, biotredin, limontar, essentiale, elcar, kudesan, corilip, quercetin, beta-carotene, kinder biovital, polivit baby, cerebrum compositum, multi-tabs, Beresh Plus drops.
As follows from the above, the choice of drugs is limited and truly “sniper” accuracy is needed when prescribing them; in addition, clinical and laboratory non-invasive monitoring of effectiveness is necessary. Attention should be paid to the possibility of relatively non-traumatic administration of drugs - cutaneous (soybean oil), inhalation (essential oils in aromatherapy), rectal suppositories (many homeopathic remedies). In neonatology, it is important to use the most “pure” drugs, for example, it is advisable to choose from piracetam drugs produced by the company WIS (Belgium, Switzerland). In the list of pathogenetic agents, stem cells are conventionally classified as inhibiting neural apoptosis (in the strict sense, this is not a pharmacological drug), the degree of therapeutic effectiveness of which still requires further research. At the same time, the use of fetal transplants [3] should be decisively abandoned for reasons of universal human and medical ethics.
Early (starting from the first stage) inclusion of non-drug influences in the comprehensive rehabilitation program helps ensure the minimization of drug therapy. At the second and third stages of rehabilitation of children with perinatal pathology, these methods should be recognized as a priority [1]. Undoubtedly, in ensuring successful rehabilitation, an important role belongs to adequate feeding and optimal organization of the environment (therapeutic and protective regime), but these issues are not discussed in this article. Nevertheless, some aspects of the organization of nursing for seriously ill children (limiting sensory load in the acute period of brain damage, thermal comfort, limiting electromagnetic influences, nursing on swaying mattresses or on the wool of lambs) can be classified as non-drug rehabilitation methods [1, 5, 6].
Let us list the means of non-drug treatment and rehabilitation, very roughly dividing them into physical and psychological-pedagogical, since any physical impact on a small child presupposes mandatory psycho-emotional contact with him.
Non-drug rehabilitation of children of the first year of life with perinatal lesions of the central nervous system
Physical rehabilitation: a variety of therapeutic massage, therapeutic gymnastics, “position” treatment (layouts, splints, “collars”, etc.), Voight therapy; exercises in water and hydromassage; dry immersion (imitation of weightlessness); use of the Saturn crib (zero-gravity effect + vibration massage); physiotherapy (alternating magnetic field, sinusoidal modulated currents, electrophoresis, paraffin therapy, laser therapy, light and color therapy).
Psychological and pedagogical correction and psychoaesthetic therapy: correctional (conductive) pedagogy; psychotherapeutic correction in the mother-child dyad (skin-to-skin, kangaroo contact) and in general in the family of a sick child; music therapy, aesthetic therapy; tactile-kinesthetic stimulation.
Most of the above techniques are not new. In the last 3–5 years, new developments include the method of soft vibration massage in conditions of weightlessness (domestic crib "Saturn", LLC "Rhythm", Yekaterinburg), light therapy and color therapy using a linear polarized visible light lamp "Bioptron" ("Zepter") ", Switzerland), tactile-kinesthetic stimulation of the palms and fingers, used in children with low and extremely low body weight [4]. In recent years, for premature babies, a combination of two or three “soft” methods of physical influence with psychoemotional and psychosensory correction has been especially recommended, which helps simulate the effect of the so-called “sensory rooms” used in the rehabilitation of older patients [9].
The music therapy technique for full-term and premature newborns, developed at the clinic of the Scientific Center for Children of the Russian Academy of Medical Sciences, includes both individually selected programs recorded on a tape recorder and the singing of nursing mothers [4]. Mothers learn complex soft psychosensory stimulation of the child, hum lullabies and other recommended songs, learn to carry out melorhythmic effects (movement and tactile stimulation combined with singing and reading poetry) - elements of eurythmy therapy according to R. Steiner, who proved the beneficial effect of rhythmic movements on the child’s body to the music [10].
In recent years, it has been established that it is necessary to begin communication with a child during the period of intrauterine ontogenesis; Today, perinatal psychology and perinatal pedagogy are actively developing. For children with perinatal pathology of the central nervous system, the early start of pedagogical correction (elements of conductive pedagogy) is the most important component of rehabilitation, since soft sensory and emotional influences are non-drug “nootrophs” for the developing brain [1, 4, 5, 6]. The daily influence of parents (primarily the mother) is directed by a specialist - a psychologist (teacher), who forms an active position in parents to overcome psychoneurological defects, teaches them various forms, techniques and means of interaction with the child and the ability to evaluate his reactions.
The goal of early pedagogical correctional work is to create conditions for the progressive psychosocial development of the child, to use his individual “compensation potential.” At each age stage, the teacher solves certain developmental tasks: first, this is the stimulation of the child’s interest in the environment, the formation of exploratory behavior, then the strengthening of inter-analyzer connections, expanding the range of sensorimotor skills and abilities, increasing commutative activity, developing and enriching play and object-based activities, as well as social child activity [11].
This article does not address some special aspects of rehabilitation (correction of visual impairments in retinopathy of prematurity, sensorineural hearing loss, orthopedic pathology).
The use of a wide range of non-drug interventions in the second and third stages of rehabilitation of sick children allows (according to the clinic of the Scientific Center for Children of the Russian Academy of Medical Sciences) to reduce the dosage and duration of courses of pharmacotherapy (for vasoactive drugs - by 15–20% and 3–3.5 days; for diuretics (diacarb) - by 20–30% and 2–3 days; for sedatives — by 30–40% and 4–5 days).
The effectiveness of complex rehabilitation was assessed in the clinic when children reached 1.5–2 years of age. Functional compensation of neurological and neurosensory disorders occurred in almost all children with moderate and mild forms of perinatal brain damage and in 80% of children with severe (as assessed in the neonatal period) disorders. In addition, even in children who had a disability due to a sensory or motor defect at the end of the observation period, it was possible to achieve some mitigation of motor or sensory disorders and, accordingly, a slight improvement in the quality of life. E. P. Bombardirova, Doctor of Medical Sciences, Professor G. V. Yatsyk, Doctor of Medical Sciences, Professor A. A. Stepanov, Candidate of Medical Sciences SCCD RAMS, Moscow
For questions about literature, please contact the editor.