Brain neoplasms firmly occupy second place among oncological pathologies and causes of death in children with cancer, second in frequency only to lesions of the hematopoietic and lymphatic systems. Tumors of the third ventricle are a relatively rare group of brain tumors. According to a number of authors, they range from 1.5% to 2 – 5%. The most common neoplasms of the third ventricle in children are subependymal giant cell and pilocytic astrocytomas, neurofibromas, germinomas, gliomas, craniopharyngiomas, papillomas and pineal neoplasms. In adults, the most common are colloid cysts, metastases, lymphomas, meningiomas, gliomas and pinealomas. According to various authors, from 0.5 to 1% of all verified brain tumors are localized in the pineal region. The incidence of tumors of the pineal region in children is higher than in adults, and reaches 2–6% of all intracranial neoplasms. There is a clear regional dependence of the detection rate of germ cell tumors. Thus, in Asian countries, namely Japan, the highest incidence of these tumors is noted, reaching 5–15% of all detected tumors. There is no explanation for this phenomenon to date. Tumors from the pineal parenchyma account for 17%, germ cell tumors are diagnosed in 40–65% of cases, and glial tumors are found in 15% of tumors in this location. Parenchymal pineal tumors are more common in children in the first decade of life; germ cell tumors are more often diagnosed in adolescents, mainly boys. Astrocytomas of this localization have two age peaks: from 2 to 6 years and from 12 to 18 years.
Gliomas of the optic nerves and chiasm make up 3–5% of all intracranial tumors in children. More than 75% of tumors affecting the optic nerves occur during the first decade of life with a peak in the first 5 years and 90% occur by age 20 years; chiasmal lesions are more often reported in older children. Approximately 20% of children with optic chiasmal gliomas have neurofibromatosis type I, and some researchers argue that the prognosis for these children is better than for patients without neurofibromatosis type I. According to other data, the incidence of chiasmal gliomas is 5–10%. Histologically, these tumors are usually low-grade fibrillary or pilocytic astrocytomas. Their microscopic features are virtually identical to those of classic cerebellar astrocytoma and other midline pilocytic tumors. Signs of malignant growth are rare. Among all primary brain tumors in children, craniopharyngiomas account for 8.2% - 13% and are the most common (40%) supratentorial tumors, and approximately 1/3 of them are localized in the third ventricle (intraventricular and extra-intraventricular craniopharyngiomas). According to A. Yu Ulitin (1997), in St. Petersburg, craniopharyngiomas accounted for 1.8% of all verified brain tumors. Craniopharyngiomas are the most common tumors of the suprasellar region of nonglial origin in children and account for 54% of all tumors of the suprasellar region in children and 20% in adults. The highest peak incidence is at the age of 5–10 years, in adults at 40–50 years. There are no significant gender differences noted.
MORPHOLOGY OF TUMORS OF THE III VENTRICLE
The morphology of tumors of the third ventricle is different. In the anterior parts of the ventricle, colloid cysts are more often observed, which are classified as dysembryogenetic neoplasms. Previously it was believed that they are derivatives of the neuroectoderm (paraphysis - an embryonic structure that is a pocket between the telencephalon and the anterior parts of the midbrain), but more data indicate their endodermal origin. They have an epithelial lining and characteristic mucous contents and are more common in adults. Macroscopically, colloid cysts are round or oval-shaped formations, the diameter of which ranges from 0.3 to 4 cm. The cyst has a dense capsule with a smooth wall and viscous contents of a greenish-gray color. Recently, their endodermal origin has been established.
Ependymomas arise from the inner lining of the ventricles of the brain and account for 5–10% of all tumors of the central nervous system. Of these, 2/3 arise in the posterior cranial fossa, 10% in the spinal canal and the rest supratentorially in the lateral and third ventricles. Within the third ventricle, ependymal tumors are predominantly localized in its posterior sections; macroscopically they have the appearance of a node with a predominant localization in the ventricular cavity. They are well demarcated from the brain, but in some areas they grow into the medulla. The depth of germination depends on the malignancy. Ependymomas have well-visualized borders, and therefore their complete removal is possible. Implantation metastases of malignant ependymomas are rare. According to RI Ernestus (1996), in children the frequency of ependymomas is 18.6%, less than astrocytomas and medulloblastomas (sex ratio 6:5 with a predominance of men).
In the pineal region there are: germ cell tumors - germinoma, teratoma (or epidermoid, dermoid), teratoma with malignant transformation, embryonal carcinoma, endodermal sinus tumor, choroid carcinoma and mixed germ cell tumors; tumors from the pineal parenchyma - pinealoma, pineocytoma, pineoblastoma; gliomas and tumors from the velum interpositum - meningiomas, hemangiopericytomas, angiomas, cysts, less often - pineocytomas.
Pinealomas and germinomas, according to the same author, could be located in the suprasellar-hypothalamic region and in other sections. Pineoblastomas have an invasive growth pattern, often metastasize and are close to medulloblastomas in their histological structure and degree of malignancy. Pinealocytomas are well-circumscribed benign tumors that often have a capsule and cysts. Choroid carcinomas and yolk sac tumors look like large infiltrating formations that early disseminate along the spinal canal and in 10% of cases metastasize beyond the central nervous system (to bones, lungs, lymph nodes).
Meningioma is a very rare neoplasm of this area, especially in childhood. Their frequency is 1.5 – 2.5%.
Craniopharyngiomas localized in this area are often cystic, located in the cavity of the third ventricle, penetrate into the lateral ventricles, extraventricularly and often reach gigantic sizes. In the world literature, there is one report on the diagnosis of craniopharyngioma of the pineal region, accidentally discovered at autopsy in a 58-year-old woman who died in a fire, and a second observation in our clinic. Germinomas originate from embryonic cells, 20% of them are located in the suprasellar region, involve the floor and walls of the third ventricle, and may primarily originate from the basal ganglia. Germinomas can metastasize to the walls of the ventricles and basal cisterns.
According to the histological structure of the tumor of the bottom of the third ventricle, almost all are astrocytomas, most often low-grade juvenile pilocytic and sometimes fibrillary astrocytomas. Our data support this statement. Astrocytomas of this localization are benign neuroectodermal tumors, the histological structure of which does not change in most cases over many years of growth before and after surgical interventions. Macroscopically, astrocytomas in most cases are poorly demarcated from the surrounding tissue and are homogeneous. Pilocytic astrocytomas have the appearance of a grayish nodule. The boundaries of the tumor are quite clear, and cysts are often found. Pilocytic astrocytomas have many papillae, and tumors with severe angiomatosis are sometimes found.
Hypothalamic hamartomas are rightfully classified as developmental defects, located between the pituitary infundibulum and the mamillary bodies, and histologically consist of tissue similar to the hypothalamus. There are hormonally active and hormonally inactive forms.
Choroid papillomas make up less than 1% (0.65% according to our data) of all intracranial tumors, and only less than 10% of them are localized in the third ventricle. Most often, these tumors arise as functioning intraventricular papillomas of the roof of the third ventricle, secreting cerebrospinal fluid. Tumors of the choroid plexus have a fairly slow growth rate and reach a large size. Macroscopically, they have the appearance of a node with a finely granular lobulated surface (cauliflower-like appearance), dark red in color, dense consistency, with a predominant localization in the lumen of the ventricle. Choroid plexus carcinoma is a more aggressive tumor, accounting for 10–20% of all choroid plexus tumors. It is rightly believed that choroid carcinomas can invade the medulla over a large area. This tumor is characterized by features characteristic of anaplastic tumors and has a tendency to diffuse extracranial spread. Although choroid plexus papillomas can spread beyond the skull, their deposits are benign and, as a rule, asymptomatic. Choroid carcinomas tend to form implantation metastases, which usually become clinically apparent during the first months after surgery.
There are reports in the literature of 23 cavernous malformations of the third ventricle.
Hemangioblastomas, metastatic medulloblastomas, glioblastomas, and epidermoid cysts can also be found in the third ventricle.
CLINICAL MANIFESTATIONS OF TUMORS OF THE III VENTRICLE
Clinical diagnosis of tumors of the third ventricle is extremely difficult due to the presence in the clinical picture of the disease of very sparse focal symptoms and the development of almost only general cerebral symptoms (hydrocephalic-hypertensive phenomena, headaches, congestive optic discs).
In 1910, the first generalized work on tumors of the third ventricle appeared, in which Weisenburg analyzed 30 observations (27 from the literature and 3 of his own, of which 5 were children). And he comes to the conclusion that there are no specific symptoms for tumors of the third ventricle, and the diagnosis in all cases was established at autopsy. The most significant work on this problem was the monograph by W. Dandy, published in 1933, in which the author, based on 68 observations (21 his own and 47 literary ones), analyzes the clinical course and methods of surgical removal of tumors of the third ventricle.
It is generally accepted that tumors of the third ventricle are asymptomatic for a long time and only as they grow and fill the cavity of the third ventricle, compression of paraventricular formations creates occlusion of the cerebrospinal fluid pathways and manifests characteristic clinical symptoms. Although the clinical picture of tumors of the third ventricle depends on the localization of the tumor within the ventricle, the leading clinical picture of the disease is the syndrome of intracranial hypertension. And the onset of the disease in most cases is characterized by the appearance of general cerebral symptoms (paroxysmal headaches, vomiting, congestion in the fundus), which in most cases remain leading in the clinical picture of the disease.
Features of the clinical course depend on the starting point of tumor growth, its direction, the degree of occlusion of the cerebrospinal fluid pathways and the effect of the tumor on the formations of the third ventricle, as well as on the paraventricular and stem parts of the brain. Craniobasal symptoms of damage to the cranial nerves are caused by hydrocephalic stretching of the lateral and third ventricles with pressing of the cranial nerves to the bones of the base of the skull and large vessels of the base of the brain. Chronic basal arachnoiditis, often accompanying tumors of the third ventricle, is also sometimes the cause of damage to individual cranial nerves.
To a certain extent, the clinical picture of tumors of the third ventricle depends on the location of the tumor within the ventricle; however, many similarities can be noted for the entire group of these neoplasms. They are characterized by intracranial hypertension syndrome. The onset of the disease with tumors of the third ventricle is largely characterized by the appearance of general cerebral symptoms (headaches, vomiting, congestive optic discs), which in most cases remain leading in the clinical picture of the disease. Meningeal symptoms caused by tonic reflexes are observed quite often. Characteristic is the dissociation between constant and severe Kernig's sign with weak neck rigidity. Some authors note a forced position of the head or torso, which appears later in the disease, especially during attacks of headaches. We did not encounter any manifestations of a disease of this nature in our material.
Characteristic of tumors of the posterior sections of the third ventricle is a combination of hypertensive and quadrigeminal syndromes. The first and leading symptoms in this category of patients are symptoms of intracranial hypertension with the early development of occlusive hydrocephalus. Pathognomonic for tumors of the posterior sections of the third stomach and pineal region is the quadrigeminal syndrome, observed in 50–87% of cases. Often these tumors present with cerebellar symptoms, indicating caudal spread of the tumor. There are also endocrine disorders, which are most often represented by the syndrome of premature sexual development.
The clinical picture of tumors of the third ventricle bottom consists of endocrine hypothalamic disorders, chiasm lesions, hypertension syndrome and sella turcica lesions. The first signs of the disease can be either these symptoms alone or in combination, or they can vary significantly. With craniopharyngiomas of the third ventricle, there is a decrease in visual acuity, hypothalamic-pituitary disorders, adiposogenital syndrome, growth retardation, diabetes insipidus, sleep disturbance, etc. With gliomas of the visual pathways, ophthalmological symptoms come to the fore (decreased visual acuity, nystagmus, exophthalmos 43 – 88 %), endocrine and metabolic disorders (growth retardation, premature sexual development, diabetes insipidus, 20 - 26%), hypertensive headaches (15 - 28%), even less often - convulsive syndrome, mental disorders, paresis, (5 - 10% ), and association with neurofibromatosis (13 – 29%). Hypthalamic hamartomas, divided into two types according to MRI (parahypothalamic and intrahypothalamic), are characterized by symptoms of precocious puberty in parahypothalamic and difficult to treat seizures with mental retardation and behavioral disorders in intrahypothalamic hamartoma.
The main manifestations of the disease in tumors of the anterior sections of the third ventricle are symptoms characteristic of occlusion of the cerebrospinal fluid tract (symptoms of intracranial hypertension), in the form of increasing intensity headaches, vomiting, congestion in the fundus, and in some patients - hypertensive crises, which can be extremely difficult and even cause death. Colloid cysts are characterized by a long course of the disease and a slow increase in their volume.
All the variety of clinical symptoms in primary tumors of the third ventricle V.A. Legkonogov (1973) reduced it to the following syndromes: hydrocephalic-hypertensive, paroxysmal, periventricular, mesos- and rhombencephalic and the syndrome of mental disorders.
The dynamics of the development of clinical symptoms may indicate the initial location of tumor growth. If, for example, the disease begins with the appearance of quadrigeminal syndrome, then we can assume that the tumor comes from the pineal region, if from ophthalmological symptoms, then we can assume that the site of initial growth of the tumor was the chiasm itself. In cases where the disease manifests itself as diencephalic and endocrine metabolic disorders, it can be assumed that the tumor primarily arose in the bottom of the third ventricle.
As the tumor grows and fills the cavity of the third ventricle, the clinical picture of the disease may reveal motor and sensory disturbances, cerebellar and brainstem symptoms. With tumors of the third ventricle, certain mental disorders associated with increased intracranial pressure and tumor localization may be observed. Although typical epileptic seizures do not occur with tumors of the third ventricle. Occasionally, epileptic seizures develop, which are more often observed with neoplasms arising from the bottom of the third ventricle. They are manifested by loss of consciousness or accompanied by tonic convulsions (diencephalic seizures). W. Dandy (1933) calls these seizures “intermittent seizures.” Characteristic components of the attacks were phenomena of sensory irritation or vasomotor disturbances (chill-like tremors in the form of short-term paroxysms, profuse sweating, increased body temperature to 38 - 390 degrees).
The duration of the disease from the appearance of the first symptoms to admission to the clinic ranges from several days to 15 years.
Y. Sawamura et. al. (1995) reports on asymptomatic cysts of the pineal region in women with a peak at the age of 21 - 30 years, measuring >5 mm, accidentally detected during MRI of the brain, and at autopsy the frequency of such cysts reached 25 - 40%.
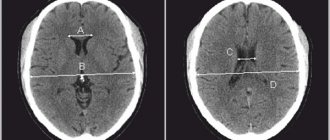
Colloid cyst of the third ventricle
A colloid cyst of the third ventricle in itself does not pose a danger to the patient’s health. Clinical manifestations depend solely on its size. This explains the fact that small cysts that a person has from birth do not affect their health. The danger of neoplasms lies in their progressive growth.
All clinical manifestations of the pathological process can be divided into 3 groups: symptoms of acute blockage of the cerebrospinal fluid circulation pathways; symptoms of a gradual increase in intracranial pressure - hydrocephalic syndrome; disturbances of higher brain functions - short-term memory, mental abilities, as well as the development of metabolic disorders.
Symptoms of acute blockage of the cerebrospinal fluid ducts
represented by an acute increase in intracranial pressure. It is characterized by a sudden unbearable headache, tinnitus, loss of consciousness, convulsions, and in some cases the patient may fall into a coma.
To gradually increase intracranial pressure
The following symptoms are typical: headache, vomiting, blurred vision, convulsions.
Headache with hydrocephalic syndrome has the following features: it intensifies in a lying position, after sleep in the morning, is not relieved by popular painkillers, is accompanied by nausea, vomiting, and, less often, depression of consciousness (drowsiness).
Vomiting with increased intracranial pressure, as a rule, is uncontrollable and does not bring relief, which distinguishes it from vomiting, for example, with food poisoning; often occurs at the height of a headache attack.
Edema of the optic discs develops as a result of the pressure of the cerebrospinal fluid accumulated in the subarachnoid space. This leads to visual impairment: the patient complains of shadows (floaters) before the eyes, flickering flashes of light. Visual acuity in the initial stages of the disease is not changed, but if the increase in intracranial pressure is chronic, then gradual atrophy of the optic nerve develops, manifested by a progressive decline in visual acuity up to blindness.
Convulsions can be either generalized, when the patient’s entire body shakes, or partial, when twitching is observed in individual muscles, for example, isolated cramps of the arm or leg. A prolonged increase in intracranial pressure has a negative effect on the cerebral cortex, which leads to disruption of higher brain functions: decreased intelligence, loss of short-term memory.
Frequent manifestations of colloid cysts of the third ventricle are occlusive crises - short-term blockage of the cerebrospinal fluid ducts. This can be observed when the body of the cyst suddenly shifts in the cavity of the ventricle of the brain and the outflow of cerebrospinal fluid is blocked. After a short time, normal circulation is restored and the symptoms disappear. Occlusive crises are characterized by a sudden sharp headache, accompanied by redness of the face, palpitations, increased breathing, fever or, conversely, chills, arrhythmic pulse, and surges in blood pressure. All this can occur against the background of sudden weakness and loss of muscle tone in the arm or leg.