Cerebral aneurysm - symptoms and treatment
Having an idea of the protrusion of the walls of the cerebral arteries, it is logical to assume that the main principle of treating a cerebral aneurysm is its exclusion from the general blood flow. It sounds quite simple: close the lumen of the aneurysm, thus eliminating the threat of rupture. But in reality everything is much more complicated.
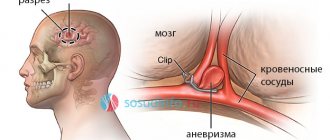
The vessels of the brain are located deep in the skull, dividing into branches, penetrating the brain and enveloping its surface. In combination with the high functional significance of the cerebral arteries, this factor significantly complicates and sometimes makes it impossible to completely shut off the aneurysm, especially in complex forms of the aneurysmal sac.
There are two fundamentally different methods of surgical treatment of patients with cerebral artery aneurysms: open or direct (i.e., through craniotomy) and endovascular (from inside the artery under X-ray control). Both options have their advantages and disadvantages.
In the case of open surgery, the first stage is to dissect the soft tissues of the cranial vault and perform trepanation (opening the cranial cavity). In patients in the acute, acute and subacute periods of SAH, the size of the trepanation window, as a rule, reaches large sizes. In patients with “silent” and “cold” aneurysms, when more than three weeks have passed since the rupture, it is permissible to use low-traumatic keyhole approaches (literally “keyhole”) with a trepanation size of up to 2.5-3.0 cm [11] .
Penetrating into the cranial cavity, the neurosurgeon, using an operating microscope and micro-instruments, opens the membranes of the brain, empties the subarachnoid cisterns (areas of expansion of the subarachnoid space in the area of divergence of the arachnoid and pia mater), washing out the cerebrospinal fluid along with blood clots. As a result, the severity and prevalence of vasospasm decreases.
Subsequently, the CSF flow paths are cleared, which reduces the risk of developing hydrocephalus. Then begins a delicate dissection (exposure) of the cerebral arteries and a step-by-step approach to the aneurysm along the artery on which it is located. In the case of a saccular configuration of the aneurysm, its neck (i.e., the very base) is highlighted. The final stage of the operation is the application of a vascular clip, which compresses the lumen of the aneurysm and stops the blood flow in it. Vascular clips are made from a medical grade titanium alloy and are clamps similar to small clothespins.
A description of the open method of surgical treatment is given in general terms. In practice, each operation on such patients is unique in its own way and requires the surgeon to use a large number of skills and techniques. The advantages of open surgery are visual control and the ability, in most cases, to completely block the aneurysm without leaving cervical areas (zones of growth of a new aneurysm). Also, during the intervention, bloody cerebrospinal fluid is removed, and it is possible to remove intracerebral hematomas if they are present. All this makes the postoperative period easier. The disadvantages of open surgery are traumaticity and the risk of inflammatory complications [2][4][5][10][13].
With the endovascular method, the femoral artery is punctured (pierced), an introducer (port) is installed into it, through which conductors are inserted to further advance them exactly to the location of the aneurysm. At all stages of such an operation, an X-ray contrast agent is supplied to the artery, due to which the position of the conductors and the anatomy of the arteries are monitored on the screen of an angiograph (special X-ray machine). Having reached the aneurysm, the x-ray angiosurgeon inserts platinum microspirals into the lumen of the aneurysmal sac, which, twisting, form a ball and tightly fill the aneurysm. Vascular stents fixed on balloons are also used in such operations. The stent is fixed inside the vessel and “switches off” the aneurysm from the bloodstream, taking on the blood pressure.
The advantages of this type of surgical treatment:
- low invasiveness (no need to perform traumatic craniotomy);
- the ability to reach an aneurysm of almost any location.
Disadvantages: high cost of consumables (coils, stents, etc.), lower percentage of radical exclusion of the aneurysm compared to the open method, inaccessibility of this type of operation (carried out mainly in large neurosurgical clinics at the federal level) [3][4][5 ][13].
Medicines
There is no drug treatment for cerebral aneurysm. An aneurysm is, in most cases, a sac-like protrusion of the vessel wall. It is not possible to eliminate this wall defect with any of the drugs. Another thing is to take measures to reduce the risk of aneurysm rupture (provide adequate treatment for hypertension, eliminate bad habits, be observed by specialists, conduct follow-up examinations, etc.).
Principles of first aid for a ruptured aneurysm
If a person experiences symptoms of subarachnoid hemorrhage (which were described earlier), you should immediately call an emergency medical team and briefly describe the main symptoms to the operator. While waiting for the ambulance to arrive, the patient must be laid on a flat surface in a position with the upper part of the body elevated 30 degrees (so that the head is above the level of the heart) - to improve venous outflow from the brain. You should also ensure maximum oxygen flow (open your airways, unfasten your clothes). Apply cold to the area of projection of the carotid arteries (the anterolateral surface of the neck) (any cooled objects at hand, including from the refrigerator) to ensure reflex vasoconstriction and accelerate blood clotting processes. If the patient is unconscious and vomiting occurs, turn him on his side and prevent vomit from entering the respiratory tract.
Is it possible to completely cure a cerebral aneurysm?
Modern methods of surgical treatment of cerebral aneurysms (both endovascular and direct surgical operations) in the overwhelming majority of cases make it possible to completely exclude the aneurysm from the bloodstream.
Rehabilitation after surgery
Rehabilitation of patients who have undergone surgery to disconnect a cerebral aneurysm is carried out to varying degrees and depends on whether the patient was operated on in the acute period of hemorrhage or outside the rupture, whether there were complications during the operation or in the early surgical period.
Depending on the severity of neurological disorders (speech disorders, motor disorders, etc.), classes are prescribed with a speech therapist, exercise therapy instructor, massage therapist, etc. Simultaneously with these activities, medications from the group of nootropics are usually prescribed, vascular-metabolic complex in order to ensure maximum improvement and restoration of lost brain functions.
Can a cerebral aneurysm develop again?
Unfortunately, even after a successful operation to exclude a cerebral aneurysm from the bloodstream, there is a risk of a new aneurysm developing in the same place. This is due to the fact that the wall of the vessel on which the aneurysm formed is sometimes changed not only in the area of the protrusion (aneurysm) itself, but has a defective structure in the sections adjacent to the aneurysm. The degree to which the aneurysm is turned off during surgery is also important, since preservation of even a small fragment of the aneurysm neck can subsequently lead to the formation of a protrusion in this obviously weak spot of the vessel.
Are folk remedies used?
Folk remedies for the treatment of cerebral aneurysm are ineffective. Lack of timely adequate treatment for a ruptured aneurysm can lead to the death of the patient.
Causes of development of aortic aneurysm
The exact causes of pathological enlargement of the aorta have not yet been established. The generally accepted point of view is that congenital weakness of connective tissue is the main factor in the development of the disease. This theory is supported by the multiplicity of aneurysms in different parts of the arterial system. Other risk factors include:
- Atherosclerosis - damage to the aortic wall by lipid plaques weakens the vessel wall.
- High blood pressure, which greatly increases the load on the aortic wall. As a result of arterial hypertension, an aneurysm of the ascending aorta, root, thoracic and other parts develops.
- Diabetes mellitus damages blood vessels, leading to accelerated development of atherosclerosis, swelling of the vessel wall and the risk of developing an aneurysm.
- Aortic aneurysm sometimes develops with cystic medial necrosis, a congenital degeneration of the connective tissue of the artery wall. This occurs in a rare hereditary disease - Marfan syndrome. Sometimes a similar pathological process occurs during pregnancy.
- Mycotic aortic aneurysm is an infectious process in the wall of blood vessels. This pathology can develop when bacteria enter against the background of specific diseases (syphilis) or nonspecific sepsis.
- Inflammatory aneurysms - connective tissue diseases (vasculitis, rheumatism, psoriasis) can cause weakening of the vascular wall and the development of pathological expansion.
- Traumatic aortic aneurysms develop as a result of a contusion of the chest or abdomen, most often in car accidents or falls from a height. Damage to a section of the aorta may occur with incomplete rupture of the wall, and the weakened wall may stretch and lead to the formation of an aneurysm.
Forecast for life
The prognosis of the disease depends on the location of the vascular protrusion and its size. The initial condition of the patient also has a huge impact. The mortality rate in case of rupture of a cerebral aneurysm exceeds 30-50%. Surviving patients sometimes retain the consequences of the condition in the form of movement restrictions, cognitive impairment and a significant decrease in quality of life. Mortality after recurrent hemorrhage exceeds 70%.
Therefore, it is so important to carry out surgical treatment in time, turning to a qualified neurosurgeon. The operation is postponed only if there are certain medical indications.
Successful neurosurgical operations are carried out at the Burdenko Research Institute. Patients with signs of an aneurysm or suspected aneurysm are admitted here. At the Institute of Neurosurgery, it is possible to carry out comprehensive diagnostics using the latest technology and further treatment of identified diseases.
Preventive actions
- It is necessary to constantly monitor blood pressure and cholesterol levels.
- You should give up all bad habits.
- Nutrition must be correct.
- If possible, it is necessary to avoid stressful situations.
- If the patient has already been diagnosed with an aneurysm, then physical activity is contraindicated for him, and he also needs to take medications prescribed by the doctor. This measure is temporary and must be observed until the operation to remove the aneurysm is performed.
Complications
One of the most dangerous complications of an aneurysm, which often becomes fatal, is its rupture with subsequent hemorrhage.
· If the lesion is localized in the brain, the clinical picture will resemble a hemorrhagic stroke.
· Particularly massive hemorrhage, which can lead to rapid death, is observed when an aortic aneurysm ruptures.
· When the lesion is localized in the myocardium, cardiac arrest occurs.
Aneurysm rupture may be preceded by dissection of the arterial wall. Most often, dissection occurs in the aorta. In this case, a second (false) passage is formed, through which blood flow can continue. With large aneurysms, the development of thromboembolism is also possible.
Which method of diagnosing a fusiform aneurysm to choose: MRI, CT, angiography
Selection method
- DSA (CT angiography, MR angiography).
Is MSCT of cerebral vessels informative for fusimorphic aneurysm?
- Tubular hyperdense structure in a typical location
- Fusiform aneurysm of the basilar artery: prepontine localization
- Fusiform aneurysm of the middle cerebral artery: Sylvian fissure
- Calcification of the vessel wall
- Significant enhancement after CS injection (CT angiography).
What will MRI images of the brain show for a fusiform aneurysm?
- In addition to other factors, the signal depends on the speed and direction of blood flow and on the presence and “age” of blood clots.
In what cases is angiography of cerebral vessels performed for an aneurysm?
- Allows you to visualize only the free lumen, but not thrombosed areas.