There are a huge number of myths and misconceptions about psychiatry among people. As a practicing doctor, I encounter this phenomenon all the time. You can hear so many ideas and suggestions for treatment from patients and their loved ones!
Just a few days ago, the mother of a patient suffering from schizophrenia suggested that her daughter undergo an “intestinal drainage” in order to “get rid of the sludge that leads to hallucinations.” Another mother of a mentally ill patient insisted on massage of the prostate gland for approximately the same purpose. I am even afraid to count how many proposals I have listened to regarding the treatment of mentally ill patients with urine therapy, honey, mud, physical activity and diets.
More than once I was asked to “scare the patient more strongly” - “because stress will make the disease go away,” they insisted on immersing the patient in ice water on the feast of Epiphany. And the rituals of reprimand or exorcism of the most varied scale... I think that if I followed the lead of these well-wishers, I would risk ending up in the hospital or, what’s the best, behind bars. It would be difficult to explain to “competent comrades” why I immersed a sick person in wormwood against his will... A lot of myths and misconceptions are associated with schizophrenia. As often as not, “in the world” our patients are called “crazy”, “fools”, “seizures” - without even imagining the essence of the changes happening to them, and therefore without understanding the peculiarities of their behavior, views on life, the world around them. This is called stigmatization: in essence, people deny patients the same rights as others - only due to a lack of understanding of their illness.
I will try to lift the veil of misunderstanding a little and tell you what actually happens to mentally ill people, using the example of one of the most common and severe phenomena in psychiatry.
Kandinsky-Clerambault syndrome (mental automatism syndrome; external influence syndrome, influence syndrome, alienation syndrome, mastery syndrome) is a psychopathological symptom complex manifested by alienation or loss of belonging to one’s own mental processes (mental, sensory, motor) in combination with a feeling of influence some outside force; accompanied by delusions of mental and physical influence and (or) delusions of persecution, perceptual disorders. Mental automatism syndrome can be observed in various mental illnesses: alcoholic, traumatic, vascular, infectious psychoses. It is most characteristic of schizophrenia, especially its paranoid form, and almost always indicates an unfavorable prognosis for the course of the disease.
"Hunters" and victims
The first comprehensive description of the symptoms of this disorder belongs to the Russian psychiatrist Viktor Khrisanfovich Kandinsky (1849–1889), who in 1880 published a chronicle of his own illness, “On the Doctrine of Hallucinations,” where he gave a detailed description of the observed mental disorders. In 1881, a German translation of the book was published, which quickly received responses in Germany and France.
Almost 40 years later, Gaëtan Henri Alfred Eduouard Léon Marie Gatian de Clérambault (1872–1934), a French psychiatrist, compiled a classification of the symptoms identified by Kandinsky and combined them into a syndrome, which he received name: Kandinsky-Clerambault syndrome.
Thus, Kandinsky and Clerambault independently described the syndrome of mental automatism. It is noteworthy that both psychiatrists analyzed and described their own painful experiences. They were both sick, and both eventually led to suicide.
The problem of studying “altered forms” of mental illnesses and casuistic cases has always been of significant interest due to the possibility of a better understanding of the patterns of syndrome formation in psychosis [5]. We decided to bring to the attention of the psychiatric community a case of the development of Kandinsky–Clerambault syndrome in a patient with deaf-muteness acquired in early childhood.
Patient S., 23 years old. Disabled group 2 due to bilateral acoustic neuritis. He is being observed for mental illness at the GPND No. 3 in Kharkov.
From the anamnesis. At the age of 1 year 4 months. got sick with a cold. Pediatricians suspected diphtheria, and therefore the girl was given a course of antibacterial therapy, after which she lost her hearing and speech. She studied at a boarding school for the deaf and dumb. After receiving secondary education in 2000, she entered a sewing school. In December 2000, after a conflict between her mother and the school teachers, the patient developed persistent asthenic symptoms in the form of increased fatigue, emotional lability, tearfulness and dyssomnia.
In June 2001, after passing the exams, a conflict arose among the students of the school over the distribution of scholarships, into which the patient was also drawn. The conflict situation turned out to be psychogenic for her. After which, against the background of anxious-depressive affect, the patient developed peculiar delusional ideas of relationships and tactile haptic hallucinations: the patient felt that people passing by her were deliberately “closing her and tugging at her clothes.” In addition, hallucinatory images arose with a component of delusion of meaning and “unwinding” of memories. In the air in front of her, the patient began to “see words made of colored letters,” which “reminded” her of the events of her life, the plot of the films she watched, and “reported” the weather forecast.
Later, again in the air in front of her, the patient began to “see” scenes from the cartoon “Tom and Jerry”, the characters of which she could control at will. These hallucinatory experiences occurred during periods of wakefulness, but more often in the evening hours.
From the end of July 2001, the patient began to see that words written in someone else’s hand began to appear inside and around her head (“bad people write with mistakes, remind of grievances”). At this time, the patient was either inhibited - she sat, staring at one point, then became stupid and gesticulated abundantly, then began to cry and complained to her mother about “these bad people.”
At the end of August 2001, psychotic symptoms increased: the patient stopped sleeping, closed the curtains and turned on the light, and told her mother that she “sees with her inner vision” the hands of some person who, using sign language [4] (“in dactyl”) tells her unpleasant news, “speaks badly and commands.” The patient has never seen this man’s face, but she “knows” that this is a “guy” and the hands belong to him. During this period, the patient stood for hours in the corner of the room, “talked to herself” in the alphabet of the deaf and dumb and “repeated her mother’s words in dactyl.” In addition, the patient experienced peculiar kinesthetic pseudohallucinations, accompanied by a feeling of influence (she felt that “a guy was writing with her hand”). The patient also had the feeling that “someone was writing bad words on her skin.”
The patient contacted the GPND, where she was prescribed haloperidol (5 mg/day), aminazine (50 mg/day) and cyclodol (4 mg/day). However, due to the lack of therapeutic effect and the development of neuroleptic akathisia, the patient was hospitalized in Kharkov City Clinical Hospital No. 15, where she remained for five months. On admission and during the first days of her hospital stay, the patient was disordered, foolish, impulsive, negative, and gesticulated profusely. Then an inversion of affect occurred: from manioform to depressive. Against the background of a depressive-apathetic mood, hallucinations continued to persist - the patient was constantly talking to someone using sign language. As a result of therapy with haloperidol, aminazine, azaleptin, cyclodol, vinpocetine and pantogam, depressive symptoms gradually smoothed out, and hallucinatory experiences became de-actualized and ceased to determine the patient’s behavior.
From additional research methods. General clinical tests revealed no pathology. The EEG shows signs of dysfunction of the midline structures. Echo-EG shows signs of liquor hypertension. CT scan shows signs of external and internal hydrocephalus. Consultation with an ophthalmologist: the fundus is normal. Consultation with a neurologist: consequences of organic damage to the central nervous system with liquor-hypertensive syndrome and vegetative-vascular dystonia. Consultation with a psychologist: no structural-logical thinking disorders were identified. Mild disturbances of thinking of the organic type were discovered in the form of uneven tempo of activity, speed of reactions and decreased switching of attention.
She was discharged with a diagnosis of “Organic schizophrenia-like disorder.”
After discharge from the hospital (in February 2002), over the next year and a half, the patient regularly visits the acute care hospital and takes haloperidol-decanoate 1.0 (once a month), azaleptin (25 mg/day), cyclodol (up to 8 mg/day ). Therapy with triftazine and rispolept turned out to be ineffective. He always comes accompanied by his mother, through whom he communicates with the doctor. Throughout this time, psychotic symptoms undulate with episodic intensification and weakening of the intensity of pseudohallucinations. The patient becomes sometimes hyperthymic and stupid, sometimes irritable and negativistic, sometimes hypobulic, inactive and passively submissive.
Upon inspection. Communication occurs with the help of the patient's mother using sign language. The patient cannot clearly describe her experiences. He “answers” a number of questions evasively: “it’s hard to say, I can’t understand.” He gazes intently, without blinking, into the doctor’s eyes, with a somewhat “sly” look in his eyes. Most of the information about the nature of hallucinatory and paranoid symptoms was obtained during a long and focused conversation with the patient herself and her mother. The patient’s facial expression is monotonous—hyperthymic, foolish and “playful.” During the conversation, emotional reactions of indignation, embarrassment, irritation, and shame are not revealed. Sits in front of the doctor in a monotonous position, with his hands on his knees, pantomimic reactions are scanty. He doesn’t take enough care of his appearance: he uses makeup excessively and tackily, the nail polish is peeling, the nails are cut unevenly, broken off and nibbled in places. During the entire lengthy conversation, the patient did not change her posture, her facial expression remained stereotypical. She showed no interest in the conversation, and by the end of the examination showed no signs of fatigue.
Diagnosis of PND: “Schizophrenia, hallucinatory-paranoid form.”
When analyzing the dynamics of hallucinatory phenomena, depending on the nature of syndromekinesis, we can distinguish four stages of their development. These stages were characterized by continuous syndromic complication with a distinct change in the structure, form and content of hallucinations.
At the first, initial stage of the syndrome, the patient developed tactile haptic hallucinations and delusional ideas of relation. They were almost immediately joined by true literal and verbal-visual hallucinations of narrative content with components of madeness and unwinding of memories.
The second stage of syndromekinesis was characterized by the presence of cinematic visual hallucinations of infantile content, which were accompanied by a feeling of accomplishment and “positive” ideational automatisms in the form of the patient’s “control” of the plot of her hallucinatory images. That is, the described structure is actually a hallucinoid.
At the third stage, the structure of the syndrome included abundant verbal-visual true and pseudohallucinations, which were accompanied by a feeling of accomplishment, unwinding of memories, delusional ideas of influence, individual catatonic and hebephrenic symptoms, as well as hallucinatory behavior. Thus, the described structure is a syndrome of true and pseudohallucinosis.
At the fourth stage of syndrokinesis, the patient experienced “visual gesture-speech” pseudo-hallucinations of imperative and blasphemous content, which were accompanied by a feeling of foreign influence. In addition, the patient developed kinesthetic automatisms, tactile-verbal hallucinations of blasphemous content with a distinct component of being made, as well as echo symptoms. At the “height” of psychosis, the described symptoms were joined by negativism, impulsivity, alternation of pronounced catatonic-hebephrenic arousal and substupor, affective symptoms and hallucinatory behavior.
Thus, “at the height” of psychosis, a polymorphic structure was formed, the basis of which was an expanded version of the Kandinsky–Clerambault syndrome, which included pseudohallucinations, kinesthetic, tactile (senestopathic) automatisms (and in the initial stages of the attack, ideational) and delusional ideas of influence.
When analyzing the dynamics of hallucinatory phenomena themselves, we identified three main patterns. Firstly, letter, verbal-visual, tactile-verbal and “visual gesture-speech” hallucinations are essentially verbal (verbal), and their unique visual and tactile form of manifestation is determined by a pronounced defect in the auditory analyzer. According to V. A. Gilyarovsky [1], such hallucinations are vicarious (substitute). That is, in a deaf-mute patient, due to damage to the auditory analyzer, its functions were taken over by the visual and tactile ones. Secondly, the dynamics of the development of hallucinatory phenomena - from true verbal-visual and cinematic hallucinations - to “gesture-speech” pseudohallucinations - indicates a “reverse” type of development of hallucinatory phenomena, which is a sign of organic “soil”. And thirdly, the development of Kandinsky-Clerambault syndrome in the described patient goes through the stages of hallucinoid and true hallucinosis. This pattern in the development of an endogenous process against the background of organic pathology was pointed out by M. I. Rybalsky [6].
Considering the syndromekinesis of psychosis in general, it should be noted that the disease began in adolescence with an asthenic pre-manifest period lasting about six months. The psychosis itself arose acutely against the background of conditioned psychogenicity and within 2.5 months reached its full development. At the initial stage of psychosis, its structure included peculiar visual and tactile hallucinations, delusional ideas of relationships, which were accompanied by a feeling of accomplishment, unwinding of memories and anxious affect. The next stage of syndromekinesis was the development of a specific hallucinoid with positive ideational automatisms. At the third stage, the structure of psychosis was characterized by specific hallucinosis with delusional ideas of influence and individual catatonic symptoms. The next stage, the fourth stage of syndrokinesis, was distinguished by polymorphism. Its “core” was Kandinsky–Clerambault syndrome with peculiar pseudohallucinations, kinesthetic and tactile automatisms. In addition, the structure of the polymorphic syndrome included catatonic, hebephrenic and affective symptoms. This stage was protracted and, under the influence of intensive therapy, it underwent only partial reverse development due to the reduction of the catatonic-hebephrenic register and the deactualization of hallucinatory-paranoid symptoms.
Over the past 1.5 years, the patient has been in a state of chronic psychosis, which is characterized by an undulating course with periodic exacerbations of pseudohallucinatory experiences, rudimentary catatonic symptoms and affective disorders. At the same time, the patient developed negative symptoms in the form of flattened affect, “negative” heboidity, infantilism, impoverished motor skills, facial expressions, and decreased activity.
Thus, after a short-term asthenic pre-manifest period, the patient developed Kandinsky–Clerambault syndrome, accompanied by catatonic, hebephrenic and affective symptoms. The course of the disease is characterized by a chronic wave-like character with periodic exacerbations of positive symptoms related to the hallucinatory-paranoid, catatonic and affective registers. Negative symptoms refer to the infantile-heboid and hypobulic types of personality changes.
Taking into account the characterized syndromeotaxis of the disease, the presence of specific negative symptoms, our own clinical experience, as well as authoritative literary information [3, 8], it should be considered that the expanded version of Kandinsky–Clerambault syndrome is nosospecific in relation to the schizophrenic process. Therefore, we believe that the described case should be qualified as “Schizophrenia, hallucinatory-paranoid form, continuous course. Kandinsky–Clerambault syndrome. Personality changes according to infantile-heboid and hypobulic types.”
In addition, it should be noted that the described patient has a number of pathoplastic factors. Firstly, as a result of deaf-muteness, which arose as a result of toxic damage to the auditory nerves in early childhood, the patient experienced retardation, which led to the puerile content of painful experiences and an infantile personality change. Secondly, the toxic factor in early childhood led to the formation of an “organic soil”, which determined the prevalence of hallucinatory symptoms over delusional ones, and also led to the “reverse” dynamics of hallucinations: from true to pseudohallucinations. Thirdly, the pathoplastic factor is the very fact of “deaf-muteness”, as a result of which essentially verbal hallucinations arise in a substitutive manner in intact systems of the visual and tactile analyzers.
In conclusion, we would like to note that the described clinical case is unique. It confirms the position that the syndrome is not a random combination of symptoms, but a stable, regular structure caused by preformed response mechanisms [2]. In the above clinical observation, even such a significant organic defect as deaf-muteness did not transform a verbal pseudohallucination into a visual one, but only “transferred” it to the system of another analyzer. Kandinsky–Clerambault syndrome requires verbal pseudohallucinations, and therefore our patient experienced them in the form of unique “gesture-verbal false-visual pseudohallucinations.”
We also consider it necessary to briefly discuss one theoretical problem. It is known that a certain “nozos” causes the occurrence of preformed, relatively type-specific syndromes [7]. Thus, the schizophrenic process, in contrast to the organic one, is characterized by syndromes with verbal rather than visual psychopathological phenomena. One such syndrome is Kandinsky–Clerambault syndrome. In the described case, in the absence of an auditory analyzer, the patient still produced “verbal” hallucinations using the sign language and tactile analyzer available to her. Based on this, we formulate the debatable problem as follows. Isn’t the above clinical observation a confirmation that the schizophrenic process is an anthropogenic, actually human mental illness, which, first of all, affects the thinking (ideational) and speech, phylogenetically the youngest structures of the psyche.
Literature
- Gilyarovsky V. A. Psychiatry. - Kiev: State Medical University, 1936. - P. 25–36.
- Gohe A. The importance of symptom complexes in psychiatry // Current issues in psychiatry / Ed. T. I. Yudina. - Kharkov, 1940. - P. 7–20.
- Gulyamov M. G. Diagnostic and prognostic significance of Kandinsky syndrome. - Dushanbe: Irfon, 1968. - 257 p.
- Defectological Dictionary / Ed. A. I. Dyachkova. - M.: Pedagogy, 1970. - 474 p.
- Zhislin S. G. Essays on clinical psychiatry. - Medicine, 1965. - 313 p.
- Rybalsky M.I. Illusions, hallucinations, pseudohallucinations. - M.: Medicine, 1989. - 368 p.
- Snezhnevsky A.V. Symptomatology and nosology // Schizophrenia: clinic and pathogenesis / Ed. A. V. Snezhnevsky. - M.: Medicine, 1969. - P. 5–28.
- Khokhlov L.K. On the clinical boundaries and nosology of the Kandinsky–Clerambault syndrome of mental automatism // Social and clinical psychiatry. - 2004. - No. 2. - P. 97–102.
Symptoms of Kandinsky-Clerambault syndrome
This is a feeling of alienation from one’s own mental processes, of mastery by someone from the outside. Arises as a result of delusional ideas about the imaginary impact on the patient (for example, radiation or ultrasound).
Ideatorial, or associative, automatisms are the result of an imaginary influence on thinking processes and other forms of mental activity.
These include:
Mentism is a violent influx of thoughts and images beyond the patient's control.
A symptom of openness of thoughts is the feeling that thoughts are known to others.
“Thought withdrawal,” in which the patient’s thoughts “disappear” from the head.
“Made thoughts” is the belief that his thoughts belong to strangers, most often his persecutors, and are put into the patient’s head.
“Unwinding of memories”: patients, against their will and desire, as if under the influence of an outside force, are forced to remember certain events of their life; Often, at the same time, the patient is “showed pictures” illustrating memories.
The phenomenon of “made moods, feelings, dreams”: patients claim that their moods, feelings, likes and dislikes are the result of external influences. For example, there is a feeling that emotions do not arise independently, but under the influence of an outside force (“they laugh at me,” “they cry at me”).
Sensory or sensory automatisms usually include unpleasant sensations that also arise as a result of the imaginary influence of an outside force. They manifest themselves as a feeling of sudden heat or cold, painful sensations in the internal organs, head, and limbs. Most often they are unusual, pretentious: patients talk about extremely peculiar sensations in the form of twisting, pulsation, bursting of internal organs and body parts. For example, I heard from patients that “from radiation, the heart swells and buzzes like a bell” or “a plasticity has formed in the head... the brain has frozen, hardened...”; “My intestines are tied in knots - this is causing constipation...” The intestines were turned off, the brain was preserved, stopped - violence! In this case, there may be no real problems from the authorities at all.
Motor, or motor, automatisms include the feeling of external imposition of the movements performed by the patient. Patients believe that their actions are controlled, they move their limbs, tongue, cause a feeling of immobility, numbness, and deprive them of the ability to voluntarily move. Motor automatisms also include speech motor automatisms: patients claim that their language is spoken; the words they utter belong to strangers. So, a patient who has just scolded the doctor with the last words sharply begins to apologize: “Sorry, it’s not me... You are a good doctor, but your tongue moves in your mouth by itself...
What is this
It consists of the three most important things that do not occur to the average person and are a set of productive symptoms:
- Pseudo-hallucinations are hallucinations within one’s subjective world, i.e. “music playing behind the wall” is a true hallucination, and “music playing in the head” or perceived by the “spiritual/internal” sense is a pseudo-hallucination. The voices in my head are here too.
- Ideas of influence (mental and physical) - a feeling of the influence of force from the outside: as if they are “putting” thoughts into your head, “speaking” with your mouth and “walking” with your feet. Someone's invisible influence and the action of the cosmos, extraneous forces, persecution are also here.
- The very phenomena of mental automatism: the feeling of one’s thoughts/movements/actions/feelings as if made, unnatural, alienated. This can also be called forced thinking, as if someone is forcing
you to think.
That is, the patient feels the influence of his sick consciousness and hears his thoughts, as if it were a separate part of him - this is not a split personality, this is precisely a “ split of the mind”
" - what is included in the very name of the disease
schizophrenia
.
Pathological automatisms are the most characteristic feature of those patients with schizophrenia who are under the influence of an otherworldly extraneous force, which is most clearly manifested by impulsive actions against the patient’s wishes. This behavior can be dangerous.
Pseudohallucinations
These phenomena are characteristic specifically of Kandinsky-Clerambault syndrome. These are visual, auditory, olfactory, gustatory and other deceptions of perception, distinguished by patients from real objects (i.e., the patient seems to “see them with his inner eye” or “hears them inside his body”) and have the nature of being made, artificial.
For example, the patient “sees” “made images”: faces, entire panoramas (similar to watching a movie), which are “showed” to the patient by his “persecutors” with the help of certain “apparatuses”. Auditory pseudohallucinations - noises, words, phrases “transmitted” by radio, through various equipment; they are most often localized in the head and body; have an imperative and commentary nature, belong to familiar and unfamiliar persons; can be men's, women's, children's.
For example, one of the patients very colorfully (at the peak of an acute condition) described to me “pictures of the future” that “alien angels” were “transmitting” into his brain. It looked, he said, like a filmstrip or slides that were shown to his inner “brain” eye. He described the contents of the “pictures” in detail, but due to other thinking disorders, he could not complete the description to the end, slipping into other topics.
We also constantly have to ask patients - where exactly do they hear “voices”? If a person reports that orders or swearing are heard inside the head, even in complete silence around, this is a serious sign of our syndrome.
Causes
Kandinsky syndrome is a pathological condition that occurs along with an existing mental disorder:
- schizophrenia;
- psychoses of various nature;
- compulsive disorder.
Among the risk factors influencing the development of mental automatism are the following:
- head injuries (especially traumatic brain injuries);
- taking strong narcotic and toxic substances;
- excessive abuse of alcoholic beverages;
- stroke;
- tumors and hemorrhage in the brain;
- Wilson's disease, when copper accumulates in the body. Due to its improper distribution, many organs suffer: the liver and kidneys, brain cells, and the visual system.
- reasons related to genetic predisposition.
Delusions of influence or persecution
The patient can explain his painful sensations by influencing him using a variety of methods - from witchcraft and hypnosis to modern means (electricity, UHF waves, radio waves, radiation, atomic energy, laser beams). The influence is carried out by both individuals and organizations, often with the goal of causing harm to the patient. For example, in my practice, which began in the late 90s of the last century, the most common complaints were about the “mafia or racketeers” (everyone remembers the dashing 90s !), as well as aliens from other planets and psychic sorcerers (remember the craze for parapsychology and ufology in the 80s and 90s!).
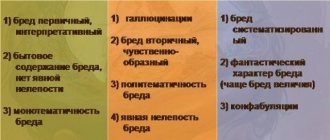
It is Kandinsky syndrome within schizophrenia that is characterized by delusions of persecution, interpretation, and influence. Other types of delusions are also inherent in other mental illnesses.
It is possible to develop an inverted version of Kandinsky-Clerambault syndrome: the patient himself supposedly has the ability to influence others, recognize their thoughts, influence their mood, feelings, and actions. These phenomena are usually combined with ideas of overestimation of one's personality or delusions of grandeur.
One of my regular patients, a fairly young girl, at the height of a schizophrenic attack, believed in “enormous magical power” emanating from her. She felt like “an all-powerful healer, connected by energy fields to the entire world,” and was unstoppable in her attempt to heal literally everyone who came into her sight. I must disappoint lovers of mysticism and energy therapy. The patient only seemed to be “guessing” the diagnosis, and she could not help anyone. But she made an excellent recovery and is now practically healthy.
First manifestations
In paranoid schizophrenia, positive symptoms are more often observed than negative ones. This means that delusions, hallucinations and thought disorders predominate, and not apathy and lack of will, as happens with other types of pathology before attacks. At the very beginning, the patient begins to have delusional ideas and thoughts. He may say that he expects something bad, scary or destructive. It happens that he is unable to calm down until, for example, he counts to 100.
Along with such thoughts, hypochondria worries me. A person is very concerned about his health and is afraid of getting sick or infected. Senestopathies often occur when there are unusual and unpleasant sensations in the body: a hoop squeezing the head, stabbing pain in the heart, as if a needle was stuck into it, etc.
At the initial stage of paranoid schizophrenia, a person’s sleep is disturbed, which affects his daytime state. His emotional background is characterized by scarcity and inflexibility, emotions are dulled. He looks like a rigid and uninterested individual who absolutely does not care what happens around him. In this case, aggression towards loved ones is possible. Your social circle is narrowing, and it becomes more difficult to establish relationships with people.
Symptoms depend on each specific case. Some patients, although few, can be violent in the initial stages. They have sadistic tendencies. They abuse animals, especially cats and dogs.
Almost all patients experience increasing fear and anxiety. Because of this, the patient turns into a confused person who cannot fully navigate the new situation. He has difficulty making decisions.
Sometimes the listed signs appear 10 or even 25 years after some injury.
This stage can continue for several years. Gradually, the number of symptoms increases as the pathology continues to progress.
Flow
Hallucinatory-paranoid syndrome within the framework of schizophrenia can develop acutely or become chronic. The acute form develops quickly, is characterized by a paroxysmal course, vivid, figurative, but poorly systematized delusions; variability, inconsistency of symptoms, intensity of emotions (not only fear, suspicion, hostility, but also high spirits), severity of mental automatisms.
The chronic form develops gradually, sometimes unnoticeably; can last for years. Usually the clinical picture becomes more complicated due to the accumulation of various automatisms. Delusional ideas are often systematized and directed. The patients’ sensations and imaginary sources of influence take on fantastic content (for example, their stomach was taken out, their intestines were blocked: they are being influenced from other continents with the participation of CIA employees, aliens).
Characteristic pathologies
The syndrome of mental automatism is most characteristic of schizophrenia, especially its paranoid form[5], and has an unfavorable prognosis. Cases of the occurrence of individual automatisms in somatogenic diseases and intoxications have been described; thus, this syndrome is not pathognomonic for schizophrenia[6].
In most cases, the appearance of this syndrome is associated precisely with schizophrenia, which is especially characterized by ideational automatisms, which in ICD-10 are considered as one of the most important signs of this disease [6].
Diagnostics
The presence of Kandinsky-Clerambault syndrome is determined by signs of the unconscious emergence and development of mental disorders with an ever-increasing feeling of alienation and awareness of their violence.
In addition, as part of the diagnosis of schizophrenia, we pay attention to other mental disorders that are characteristic of the disease itself. Indeed, with schizophrenia, specific disorders of the emotional-volitional sphere, behavioral disorders, memory and intellectual disorders occur. Of great importance is the history of the development of the disease process, its stages, the role of heredity and the premorbid personality of the patient.
All this allows the psychiatrist to separate Kandinsky syndrome from other externally similar mental phenomena.
Treatment and rehabilitation measures
Treatment of Kandinsky-Clerambault syndrome includes a set of measures, including the use of special medications (neuroleptics, antidepressants) in combination with psychotherapy sessions, and subsequently a long period of rehabilitation.
If there is a concomitant pathology in the form of psychosis, treatment is carried out in a specialized place under the constant supervision of medical staff.
The rehabilitation period is long. During this period, it is necessary to conduct regular psychotherapeutic sessions, engage in physical therapy, and strictly adhere to a diet (reduce the amount of foods containing copper).
It is also recommended to spend more time outdoors and go swimming. For successful rehabilitation, a patient with mental automatisms needs the attention of loved ones, their support and understanding.
Treatment and prevention of mental automatism syndrome
To prevent the development of Kandinsky-Clerambault syndrome, timely treatment is necessary, usually in a psychiatric hospital. Complex therapy, as part of the treatment of the underlying disease - schizophrenia:
- medicinal (neuroleptics: haloperidol, trifluoperazine, clozapine, olanzapine, risperidone and other drugs);
- biological therapy - electroconvulsive, insulin comatose;
- psychotherapy (with the positive effect of psychotropic drugs) followed by social rehabilitation (at the stage of recovery and awareness of the disease).
Paranoid syndrome
Paranoid syndrome is the next stage of paranoid schizophrenia, which is characterized by the presence of a mild form of systematic delusions. This means that the patient can interpret and explain it well. Typical crazy ideas:
- Reformative - the patient is convinced that he has invented or created something brilliant that can change the structure of the world.
- Erotic - the conviction of the existence of a maniac who constantly pursues.
- Belief in one’s own chosenness, high origin, in belonging to the royal family or representatives of “blue blood”.
- Kverulyantskie - constant slander, filing complaints and incessantly fighting for their rights.
In paranoid syndrome, delusions are structured and systematized. The patient can logically justify arguments and provide evidence of his theories. He is not tormented by hallucinations or automatisms, so he does not consider himself sick. This aggravates the situation, since he will be met with misunderstanding from people. This will lead to depression and further development of the disease.
Stages of accepting a delusional thought:
- Expectation is an internal anxiety, a feeling that something incredible is about to happen.
- Insight - suddenly a person understands where his fear comes from, he begins to see everything differently, looks at the world with “new eyes.”
- Systematization - everything fits into one picture, which the patient can rationally explain and describe.
If the disease is detected at this stage, a diagnosis of paranoid schizophrenia will be made.
Clinical picture
Symptoms of motor automatism manifest themselves in the form of constrained movements, disturbances in the functioning of the speech apparatus and atypical gestures or facial expressions. Mental disorder is the main reason for the emergence of thoughts that a person’s life proceeds under the constant control of external forces that control the patient’s behavior. At a certain stage of pathology development, changes in the functioning of the speech and musculoskeletal system are observed. Many patients often encounter situations where the disease “forces” them to utter negative and offensive words towards others. Those who are ill try to justify such behavior by the influence of external forces.
Ideatorial automatism is closely related to disturbances in the mental perception of the surrounding world. Many patients are firmly convinced that people around them hear their thoughts, steal ideas, or closely monitor their internal dialogue. The development of the disease leads to a gradual loss of control over one’s own behavior and feelings. Patients try to justify their negativity by the influence of extraneous voices that control their movements and thoughts. According to experts, many patients experience the presence of obsessive thoughts, which the patient feels belong to outside forces.
Sensory disorder manifests itself in the form of clinical symptoms that are pseudohallucinatory in nature. The vast majority of patients experience pain attacks for which there is no rational explanation
It is important to pay attention to the fact that patients have difficulty indicating a clear location of pain. According to patients, pain is expressed as a feeling of pulsation, squeezing or burning and often changes location, smoothly flowing throughout the body. Many patients believe that attacks of pain are caused by the influence of otherworldly forces
Many patients believe that attacks of pain are caused by the influence of otherworldly forces.
The syndrome can develop in two forms: acute and chronic
Etiology and pathogenesis
Since Kandinsky-Clerambault syndrome is detected primarily in schizophrenia, much less often in exogenous-organic psychoses, and even less often in epilepsy, the cause of its occurrence is associated with the etiology of these diseases. Psychogenetic point of view on K.—K. pp., shared by certain French. and domestic psychiatrists, was refuted by V. X. Kandinsky and M. Clerambault and continues to remain a subject of debate.
The modern explanation of the mechanism of mental automatisms is based on the teachings of I. P. Pavlov about pathodynamic changes in. n. d. According to him, the entire hallucinatory-paranoid picture with the phenomena of alienation, violence, phenomena of influence and mastery is regarded as a reflection of a pathologically inert irritable process in c. n. p., which either, according to the law of generalization, concentrates everything abnormal around itself, then, according to the law of induction, repels everything that is normal physiological and psychological. From this follows the hypothesis of A. A. Mehrabyan (1972) about the violation of Gnostic feelings in the general structure of thinking, speech, activity and self-awareness, leading to the functional disintegration of the psyche - through deautomatization to depersonalization.
Treatment
Treatment of paranoid schizophrenia is a complex process that does not stop even during remissions. After relief of all symptoms, the diagnosis remains. It is not a fact that they will ever appear, but a person remains at risk forever.
Depending on the stage of the pathology, the following types of therapy may be prescribed:
- Medication - the use of psychotropic substances, antipsychotics and antidepressants. In severe cases, insulin comatose treatment is prescribed.
- Psychotherapy - regular sessions with a psychotherapist, not only for the patient, but also for his relatives, who will have to learn how to interact correctly with a schizophrenic.
- Electroconvulsive. It is used in exceptional cases when the patient is resistant to medications or has contraindications to them. The therapy is based on exposing a person to electric current until convulsions occur. It is believed that seizures trigger certain neurochemical processes in the brain and enable short-term memory.
During the period of remission, maintenance therapy is carried out, which includes taking medications, abstaining from alcohol and periodic conversations with a psychologist. This helps prevent an attack and improve the patient’s quality of life. Sometimes it is possible to relieve him of all symptoms forever or for many years.
In general, it is important to start treatment as early as possible for schizophrenia. Then the prognosis will be relatively favorable. There is also the following pattern - the younger the age the first signs of pathology appear, the more destructive its impact on the psyche and personality.
History
| Having the misfortune of suffering from hallucinatory insanity for two years and retaining after recovery the ability to cause a certain kind of hallucination at will, I was naturally able to notice in myself some of the conditions for the origin of sensory delirium. |
| - psychiatrist Kandinsky. |
The syndrome is named after Viktor Kandinsky, the second cousin of the artist Wassily Kandinsky. In 1876-1877 Victor served in the navy as a ship’s doctor, participated in the Russian-Turkish War and suddenly felt that he had been “subjected” to the mental attack of the Tsarist secret police. But he seized control in time and went to psychiatry himself, where he was able to describe his experiences in the critical-clinical study “On Pseudohallucinations,” which was highly praised in his works by the luminary of psychiatry, Jaspers. In addition, he is considered the father of Russian forensic psychiatry.
To stop external “influence” on his brain, he committed suicide in the name of conspiracy at the peak of one of the attacks in 1889. through overload with substances.
There is not much interesting about the second half of the syndrome, about Clerambault: he was a similar schizophrenic psychiatrist-schizophrenic from France, “controlled” by Surte (this is a French FSO) and, independently of Kandinsky, described his symptoms of mental automatism.
He also came up with erotic delusions (Clerambault syndrome), the law of his name, and then fell into depression with delusions of guilt and shot himself.