Infectious myelopathy
Viral damage to the spinal cord is accompanied by specific types of myelitis. In the past, the most common spinal cord infection was polio. Currently, the most common cause of viral myelitis is herpes zoster, which initially produces radicular symptoms. The pathological process in herpes zoster affects not only the gray matter of the spinal cord, as in polio. Lymphocytes are always found in the cerebrospinal fluid (CSF, cerebrospinal fluid) of patients.
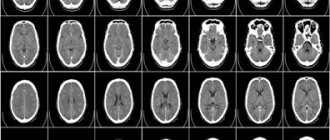
MRI of the cervical spinal cord in infectious myelitis: c — axial T2-weighted image shows that the spinal cord lesion occupies its central part; d — enhancement of the pattern of the spinal cord lesion on the axial T1-weighted image after administration of a contrast agent.
Intramedullary spinal cord abscesses have been described in systemic spinal cord infections of bacterial and mycobacterial etiology. Chronic lesions of the spinal cord membranes during syphilis can lead to sluggish secondary subpial myelitis and radiculitis. Severe granulomatous, necrotizing and inflammatory myelitis is typical of Schistosoma mansoni infestation. Granulomatous, necrotizing and inflammatory myelitis is caused by a local reaction to tissue-digesting enzymes produced by parasite eggs.
Magnetic resonance imaging (MRI) of the spinal cord for myelitis due to Zika virus infection. A - T2 MRI of the spine showing increased signal in the thoracic region T5-T8 (indicated by arrow) and enlargement of the cervical spinal cord. B, STIR MRI of the spine shows signal enhancement in the cervical spinal cord C4–C7 (arrowed).
Etiology
In some cases, the cause of myelitis cannot be identified. However, the disease has a classification based on etiological data:
- Infectious – occurs in 50% of cases. There are primary and secondary flow options. In the first case, the pathology predominantly occurs against the background of HIV infection, syphilis, CMV, enteroviruses, and herpes simplex. The main cause of secondary myelitis is osteomyelitis of the spinal column.
- Intoxication – inflammation develops during poisoning with poisons (acute intoxication with certain medications and psychotropics or prolonged exposure to harmful substances on the body, most often affecting patients with unfavorable working conditions).
- Traumatic - in case of spinal injuries, the main cause of the development of inflammatory processes is damage to the spinal column and disruption of its functions or the penetration of infection through an open wound surface.
Other causes include autoimmune pathologies affecting the myelin sheath of nerve fibers and immunopathological inflammation of the vascular walls. Sometimes myelitis occurs as a result of metastasis during cancer processes.
Spinal arachnoiditis
Spinal arachnoiditis is an inflammation accompanied by scarring and fibrous thickening of the arachnoid membrane of the spinal cord. Spinal arachnoiditis can lead to compression of the nerve roots and sometimes the spinal cord. Spinal arachnoiditis can also be a postoperative complication or aftereffect from the introduction of radiocontrast agents (for myelography), antibiotics and other chemicals into the subarachnoid space.
Anatomy of the membranes of the spinal cord and surrounding structures of the spinal canal.
Soon after an adverse effect, a large number of cells and a high concentration of protein can be detected in the cerebrospinal fluid (CSF, cerebrospinal fluid), but then the inflammatory process subsides. In the acute period of spinal arachnoiditis, the patient may have a slight increase in temperature. Bilateral asymmetrical radicular pain in the extremities may also be expressed. With spinal arachnoiditis, signs of compression of the roots are determined in the form of loss of tendon reflexes. Back pain and symptoms of root irritation are associated with lumbar arachnoiditis more often than should be the case. In addition, spinal arachnoiditis is not a common cause of spinal cord compression.
Approaches to the treatment of spinal arachnoiditis among neurologists and neurosurgeons are controversial. In some patients, improvement occurs after laminectomy (removal of part of the vertebral arch). Multiple meningeal arachnoid cysts located along the nerve roots may be a congenital anomaly. Increasing in volume, these arachnoid cysts cause deformation or stretching of the spinal nerve roots and ganglia, causing severe radicular pain in adult patients.
2.Symptoms and diagnosis of myelitis
Acute and subacute course of myelitis is characterized by general infectious symptoms:
- high temperature (38-39°C);
- weakness, increased sweating;
- chills;
- loss of strength, apathy.
Neurological manifestations begin with mild back pain and progress to motor, sensory and pelvic disorders. A characteristic sign of myelitis is the irradiation of pain to areas of the body adjacent to the spine. The development of symptoms often occurs rapidly within 1-3 days. The nature and intensity of the disorders depend on the location of the source of inflammation in the spine (thoracic, upper cervical, lumbar, and sacral myelitis are distinguished). Damage to the upper parts of the spine is especially dangerous, as it threatens to stop breathing. The following clinical picture is possible:
- peripheral paraparesis or paraplegia of the lower extremities;
- lack of deep reflexes;
- convulsions;
- retention or incontinence of urine and feces;
- spastic paralysis of the legs;
- bulbar and respiratory disorders;
- hypoesthesia and anesthesia.
With the development of acute transverse myelitis, regardless of the location of the source of inflammation, the phenomena of diaschisis with a general decrease in muscle tone are observed.
Diagnosis of myelitis is mostly traumatic, since the clearest picture is given by lumbar puncture. Additional diagnostic techniques include MRI, CT of the spine and myelography. Often, a visible symptom complex allows a preliminary diagnosis to be made. Additional studies only confirm it, allowing it to be differentiated from epiduritis, acute Guillain-Barré polyradiculoneuritis, tumor diseases, and acute cerebrospinal circulatory disorders.
Visit our Neurology page
Recovery prognosis
According to clinical practice, the prognosis for spinal cord myelitis largely depends on the cause and severity of the disease. In the vast majority of cases, purulent myelitis has an unfavorable outcome. An extremely negative prognosis is observed in ascending forms of the disease, when the inflammatory process spreads to the brain stem. Mechanical ventilators offer the opportunity to save some of the patients.
The prognosis is aggravated by the spread of the infectious process to other organs, forming purulent foci (abscesses) in them. In uncomplicated forms of spinal cord myelitis, approximately 30% of patients with a favorable course and adequate treatment can expect a complete recovery. As clinical experience shows, if neurological disorders do not go away for more than 90 days, then the prognosis for complete recovery is quite doubtful.
With timely diagnosis and persistent treatment, improvement in the patient’s condition occurs after 2-3 months, and maximum restoration of the body’s functioning occurs after 1-2 years. With paralysis of both legs, the patient is assigned the first disability group, and with residual paralysis of the legs and weakness of the sphincters - the third disability group. Partial paralysis of the legs and gait disturbance are the reasons for recognition of the second disabled group with a ban on employment.
Course of the disease
Researchers talk about three options for the development of the disease. In acute transverse myelitis, neurological symptoms are observed within two weeks. After this comes the recovery stage. Later, for an indefinite period, residual effects persist or gradually disappear.
In the second option, the main symptoms remain for life.
The third type, like many other neuromuscular pathologies, is characterized by the gradual development and ascending spread of the inflammatory process with subsequent damage to the trunk. Demyelinating lesions appear in the brain.
Myelitis of the spinal cord
Myelitis is a neurological disease in which several types and types of disease are distinguished. Each type of spinal cord myelopathy has its own characteristics of the course of the disease, symptoms and severity of their manifestation, as well as methods of treatment and further prognosis. The disease may appear after the virus and its toxic substances have penetrated the spinal cord. Inflammation can affect the body of the spinal cord, its processes, nerve endings and roots, as well as various membranes.
Treatment of myelitis in Samara
Treatment in the acute phase of the disease is carried out in a hospital neurological department. A treatment regimen for myelitis is developed by a neurologist, taking into account the etiological data and individual characteristics of the development of the disease in a particular patient.
The basis of therapy is broad-spectrum antibacterial agents in large dosages, glucocorticosteroids, and analgesics. In some cases, medications are used to reduce the tone of skeletal muscles, uroseptics (antiseptic drugs to kill infections in the genitourinary organs). For problems with urination, catheterization of the bladder is indicated.
During the rehabilitation period, exercise therapy, therapeutic massage and physiotherapeutic treatment are prescribed. In the First Neurology clinic, the following methods are used in the treatment of myelitis:
- Peripheral magnetic stimulation,
- High top on the affected limbs,
- Injection of botulinum toxin type A into tense muscles,
- Magnetotherapy using the Multimag device,
- Injectable forms of medications and ILBI are prescribed.
- Ozonation of blood.
The goal of therapy is to restore damaged nerve fibers, which will lead to improved motor activity, reduced pain, and restoration of pelvic organ function.
Pathogenesis
Causes:
- Acute disseminated encephalomyelitis: acute inflammatory process in the brain and spinal cord; occurs after infection (post-infectious), immunization (post-vaccination) or suddenly.
- Infectious: viral (herpes, herpes zoster, cytomegalovirus, enterovirus, Epstein-Barr virus, HIV, influenza, rabies), bacterial (mycoplasmosis, syphilis, borreliosis, tuberculosis).
- Systemic diseases: systemic lupus erythematosus, Sjogren's syndrome, sarcoidosis.
- Multiple sclerosis.
- Paraneoplastic syndrome.
- Vascular causes (arteriovenous malformations, vasculitis, thrombosis of the spinal arteries).
- Radiation myelopathy.
- Idiopathic.
- Allergic.
Treatment tactics
Urgent measures:
- Intravenous administration of high doses of glucocorticoids.
- Plasmapheresis.
- Antibacterial therapy in case of infectious etiology of the disease.
- Anticoagulant therapy in patients with systemic lupus erythematosus and antiphospholipid syndrome.
- If indicated, neurosurgical intervention is performed.
Subsequent treatment:
- Rehabilitation.
- Analgesics.
- Muscle relaxants.
Read also
Herpes zoster
Varicella zoster first enters the human body at an early age and manifests itself as chickenpox, most often in children.
Then follows the latent phase of circulation of the pathogen in the body and under certain conditions... Read more
Hepatic encephalopathy
Hepatic encephalopathy is a brain lesion that occurs against the background of liver pathology and is caused by liver failure. There is acute hepatic encephalopathy, which occurs on…
More details
Rehabilitation after stroke
It is very important to begin rehabilitation after a stroke as early as possible, since further recovery and the ability to avoid disability depend on this. For rehabilitation after a stroke in the clinic “First...
More details
Ankylosing spondylitis/ankylosing spondylitis
Ankylosing spondylitis (ankylosing spondylitis) is a chronic inflammatory disease of the spine and joints, accompanied by progressive pain, stiffness and limited movement at the beginning...
More details
Pelvic pain
Pelvic pain is pain in the muscles that form the pelvic floor and organs located in the small pelvis, caused by microtrauma, chronic deformation of the sacrococcygeal region due to anatomical…
More details
Myelography
According to the literature, “in all doubtful cases of acute and chronic myelopathies, myelography data play a significant role...” (Bersnev V.P. et al., 1998)
Before myelography, all animals were administered antibiotics and methylprednisolone at a dose of 30 mg/kg. Thanks to myelography, it is possible to accurately assess the size of spinal cord edema. Sometimes this test can reveal the cause of myelitis in cases where myelitis developed as a complication of instability or as a result of compression of the spinal cord by an intervertebral disc or tumor. It is necessary to begin myelography with atlanto-occipital puncture. At the same time, a sample of the cerebrospinal fluid is taken. If the contrast does not penetrate the thoracic and lumbar spine, a lumbar puncture is mandatory to contrast the entire subdural space, even if it seems that the diagnosis is obvious. From our experience, the following sequence of punctures is important: first, the atlanto-occipital one is performed, and then the lumbar one. This is due to the fact that with myelitis, significant swelling of the spinal cord develops, this causes a decrease in the subdural space, which makes it impossible to obtain cerebrospinal fluid. With atlanto-occipital puncture, it is almost always possible to obtain cerebrospinal fluid, even if the cervical spine is affected. The study of cerebrospinal fluid in myelitis can be crucial.
Visual assessment of the spinal cord during surgery can be decisive in some cases. When performing a hemilaminectomy or laminectomy with significant swelling of the spinal cord, a durotomy must be performed. After opening the dura mater, in some cases the spinal cord leaks out. In this case, we can talk about the impossibility of restoring the spinal cord. To confirm necrotizing myelitis, an imprint can be taken for cytological examination.