The human body consists of a huge number of cells. They, in turn, are combined into larger units - tissues and organs. Organ systems are built from the latter, and from them the organism is formed. And at all levels, various interactions and complex biochemical reactions are constantly taking place. In order for all this to develop harmoniously from a fertilized egg and function smoothly, a special work scheme is required for all levels. Its role in the body is performed by organized genetic information.
It is the hereditary material that is entrusted with the task of preserving data about the general appearance of a person, the structural features of individual organs, the principles of regulation with the help of hormones, and even how proteins should be assembled. All data is recorded as a sequence of structural units - nucleotides. They, like the letters of the alphabet, form word groups that perform specific functions. Each group is called a gene. Together they form the DNA molecule. If you look at a higher level, you will notice that all the hereditary material in the form of chains of deoxyribonucleic acid is concentrated in special formations called chromosomes.
A person normally has 23 pairs of them. In each pair, information is stored in two copies. This is necessary so that when genetic information is transferred, each daughter cell receives its own copy. One pair of chromosomes is different from the rest and is responsible for determining sex. If it has two identical large chromosomes (XX variant), then the organism is female. If there is one large and one small chromosome, then we are talking about the male sex (XY variant). These two different chromosomes are called sex chromosomes. The remaining 22 pairs are found in all organisms, regardless of gender. They are called autosomes.
Anomalies of genetic material
Hereditary material consists of a huge number of nucleotides that form genes. Moreover, in each gene the nucleotide sequence is strictly defined, since it must code for a specific protein. In addition, the genes themselves, when forming chromosomes, are also arranged in a fixed order. Thanks to the preservation of this order, the body can function, and scientists can quickly and accurately indicate to each other which gene we are talking about.
Ideally, the system works without the slightest glitch, and genetic information is always transmitted unchanged. However, in practice, a large number of structural units and constant exposure to various factors (for example, ionizing radiation) leads to the fact that various anomalies arise from time to time. In particular, individual sections of the DNA sequence can be copied to a new location. In this case, they talk about duplication. If, instead of creating a new copy, part of the original chain was moved, then the modification is called translocation. In addition, sometimes part of the sequence is simply lost, removed from the genetic material. In this case, the change is called a deletion.
Since the interactions in the body have been honed over many millennia of evolutionary development, the result is a very coherent system. And anomalies, even the smallest ones, can cause an imbalance. In this case, one or another disorder develops in the body. If the cause is at the level of genes, then they speak of gene diseases. If an extra copy of a chromosome is lost or, on the contrary, gained, such disorders are called chromosomal diseases.
Treatment results in Germany
Tatyana (patient’s mother): “Our result: Violetta was diagnosed with Angelman syndrome (a genetic disease that was also confirmed by genetic research). After starting to take medication for sleep, the epileptic seizures, oddly enough, stopped, as my daughter began to sleep and her day-night routine was established.
We did not fly to Germany for the second time to select medications for epilepsy, because... There is simply no epilepsy now. They did an EEG - everything was quiet and calm in our daughter’s head. Our doctors said that it does not happen that the encephalogram changes so much within a month. Using GLORISMED, we sent the EEG results to the doctor in Berlin - the doctor also confirmed that there was no epileptic activity.
So much effort, nerves, money was spent in Russia... And here we were in Berlin for three days - and we were told how to continue to live and fight the now understandable disease!!!
Dear parents, do not waste time and money on examination and therapy in Russia or other (especially Asian) countries. Find the cause of the disease and then carry out the right therapy with the right doctors. Germany has the best doctors and diagnosticians. Believe me, when you know what exactly to treat, the treatment is cheaper and more effective!
About GLORISMED. I am very grateful to the staff. I'm glad I came across them. They answer all questions, organize and accompany you during your stay in Germany, constantly on the phone. They do everything competently and calmly in any situation.
Even when I am already in Russia, I constantly ask the employees questions about medications, communication with the doctor, etc. I receive answers quickly, and everything becomes clear. Just a low bow to the guys from GLORISMED, because we, mothers, have different moods, we need a solution here and now - and they are great at providing this solution!”
Epilepsy
Epilepsy. Epileptology. Treatment of children with epilepsy. Epilepsy belongs to the common neurological diseases of a special type that depress human life
Let us help you find the right solution in this difficult situation with your health.
Contact us in any way convenient for you: by phone , by email , by Skype online, by filling out the contact form .
Tell us your contact phone number, our employees will call you back and will gladly answer all your questions absolutely free of charge and guide you on the correct selection of a medical institution, recommend a competent specialist - a well-known doctor from one of the serious specialized German clinics, and also tell you the approximate cost treatment program that is required specifically for you or people close to you.
The consultation is absolutely free for you!
What is microdeletion syndrome?
The most minor changes (aka mutations) are called point changes. Their appearance affects a few units of genes. In some cases, the disorder relates to just one gene. However, if it provided the production of an important protein, the consequences for the entire body could be very serious. Such pathological changes belong to the group of microdeletion syndromes.
Each such disease is caused by a small change in genetic material that occurs in a strictly defined location. The exact mechanism of occurrence of such disorders has not been established to date, which does not prevent scientists from studying their effects on the body.
Thus, it was found that the development of the syndrome in this case can occur in several different ways. In particular, a number of diseases are characterized by the participation of oncogenes. In other cases, the effect of the deletion itself is superimposed by the effect of chromosomal imprinting and possible uniparental disomies.
The incidence of most microdeletion syndromes is extremely low: about 1 case per 50-100 thousand newborns. A set of clinical signs is usually expressed clearly. In order to make a diagnosis, only a combination of symptoms is enough. However, with this approach it is impossible to accurately predict the health of the offspring, so often, along with checking the usual signs, a molecular genetic diagnosis of the proband and his relatives (usually parents, in some cases also requires analysis of the genotype of brothers, sisters, aunts, uncles, and so on) is carried out.
Pathological manifestations vary greatly. In particular, their manifestation is determined by how much of the genetic material was lost as a result of the deletion. In addition, in some cases, the role from which parent the mutation was received (the influence of chromosomal imprinting) plays a role. A good illustration of the latter situation is the pair of Prader-Willi and Angelman syndromes. They are both caused by the presence of a deletion on chromosome 15. However, due to the different mechanism of action when transmitted from different parents, the clinical picture of these diseases differs significantly.
Pathogenesis and causes
This defect occurs due to deletion (loss of a piece of genetic material) of a segment of chromosome 15. Other causes are often cited as unipaternal disomy (inheritance of two paternal copies of a chromosome, instead of copies from both parents), translocation or mutation of a single gene.
The syndrome can also appear as a result of a mutation in a gene involved in ubiquitin metabolism.
Most patients with this pathology do not have a family history of genetic abnormalities. However, for a certain percentage of patients this syndrome is inherited. The risks become higher if the parents have chromosomal abnormalities. An interesting fact is that if a child with this syndrome is born in a family, then the probability of having another child with the same pathology is 1%.
The appearance of Angelman syndrome is quite spontaneous, and almost any family can have a child with this disease. There are no specific statistics on the number of children with this syndrome.
According to various estimates, the number of newborns with doll syndrome ranges from one in ten thousand to one in twenty thousand. Scientists suggest that in reality this number is much higher.
Positive effects of some deletions on viability
Small deletion changes can have a significant impact on the survival of the organism. For example, the loss of the gene encoding the CCR5-δ32 protein causes immunity to the human immunodeficiency virus. Scientists suggest that this mutation first appeared about 2.5 thousand years ago and over time spread across Europe.
The current distribution is uneven. According to statistics, about 10% of residents of European countries are resistant to HIV. However, in the Scandinavian countries this figure reaches 14-15 percent. Russians and Finns demonstrate a 16 percent level of resistance. For Sardinia, however, the frequency is a modest 4 percent.
A number of scientists have hypothesized that such a spread is determined by the bubonic plague epidemics that took place in the medieval period. It is likely that a mutation in the gene causes increased resistance to this disease. Therefore, in the countries where the Black Death took place, more people with this genotype survived.
The effect of deletions on the ability to fertilize
Deletions that occur on normal chromosomes (autosomes) can in some cases be compensated for by a normal copy of the gene. However, when it comes to sex chromosomes, especially the Y chromosome, the situation changes.
First of all, it should be noted that the genes localized on it do not have a second copy. With a normal number of chromosomes in the set, the Y chromosome turns out to be extremely vulnerable. Combined with a small number of genes, this leads to serious consequences for each change. Of particular interest are mutations affecting the AZF locus and the SRY gene.
Pathogenesis
Normally, a person inherits maternal and paternal copies of chromosome 15. In a part of the chromosome that is important for the development of Angelman syndrome, the process of converting hereditary information from maternal and paternal genes into protein or RNA (gene expression) is noticeably different.
The expression of these genes is associated with gender epigenetic imprinting, in which the transformation of certain genes depends on which parental allele was received. For most genes, both parental alleles are transformed, but with imprinting, only one parental allele is transformed (such genes account for less than 1%). Traits that are determined by these genes are not inherited according to Mendel's law.
Imprinting occurs due to the absence of changes in the nucleotide sequence of the DNA molecule when the molecule is modified. The sequence of DNA nucleotides is recognized by the enzyme RNA polymerase (carries out transcription).
Normally, on this section of chromosome 15, the expression of the mother's allele predominates, and the paternal allele is weakly manifested. When mutations or loss of the maternal copy of genes or defects in genomic imprinting occur, Angelman syndrome develops.
The development of the syndrome is also caused by a mutation in the UBE3A gene, which is necessary for ubiquitin metabolism. This gene is present on both parental chromosomes. The paternal copy of the gene is inactivated in the hippocampus and cerebellum, while the maternal allele almost always remains active. The syndrome is usually caused by the loss of the maternal copy of chromosome in the region 15 q11-13, which provokes a lack of conversion of the DNA nucleotide sequence of the parental copy of UBE3A in the brain. The lack of expression of the maternal copy of this gene leads to serious abnormalities in the activity of the hippocampus.
Abnormalities of the SRY gene (Sex-determining Region Y)
The SRY gene, as its name suggests, is responsible for a very important function. It is its presence in the chromosome set that triggers the process of formation of the body according to the male phenotype and stimulates the development of the corresponding genital organs.
The presence of even a small deletion in this gene disrupts the mechanism of sex differentiation. As a result, with a normal karyotype of 46XY, the embryo begins to develop as a female organism. For this reason, the SRY gene accounts for the largest number of mutations associated with underdeveloped gonads. In addition, changes in this gene cause sex inversion.
Preparing for your appointment
Call your doctor if your baby or child has not reached expected developmental milestones or has other signs or symptoms common to Angelman syndrome. Your doctor may then see a doctor who specializes in conditions that affect the brain and nervous system (neurologist).
Here's some information to help you prepare for your meeting.
What can you do
- Write down the signs or symptoms you notice in your child and for how long.
- Bring children's books and other records of your child's development to your appointment. Photographs and videos may be helpful.
- List your child's basic medical information, including other conditions for which your child is being treated and the names of medications, vitamins, or supplements he or she takes.
- Ask a family member or friend to join you in nominating your child. If your child's doctor mentions the possibility of developing a disorder, you may have difficulty focusing on anything the doctor says. Find someone who can offer emotional support and help you remember this information.
- Write down questions to ask your doctor.
Questions to ask your child's doctor include:
- What might cause my baby's signs and symptoms?
- Are there other possible causes for these signs and symptoms?
- What tests does my child need?
- Should my child see a specialist?
Questions asked by the specialist include:
- Does my child have Angelman syndrome?
- What are the possible complications of this condition?
- What treatments are available?
- What treatment do you recommend?
- What is the long-term outlook for my child?
- Should my child or I be tested for genetic mutations associated with this disease?
- What other specialists should my child see?
- How can I find other families coping with Angelman syndrome?
Feel free to ask other questions.
What to expect from your doctor
A doctor who sees your child as having possible Angleman syndrome will likely ask you a number of questions, such as:
- What are your baby's signs and symptoms and when did you notice them?
- Does your child have feeding problems?
- Is your child achieving expected age-related physical milestones?
- Have you noticed problems with balance, coordination or movement?
- Does your child laugh, smile, or express excitement more often than his or her peers?
- Does your child express excitement with unusual physical behavior such as holding a hand?
- Does your child communicate verbally?
- How well does your baby sleep?
- Has your child had seizures? If yes, how often?
- Have any of your child's first-degree relatives, such as a parent or brother, been diagnosed with Angelman syndrome?
Share link:
- Click to share on Twitter (Opens in new window)
- Click here to share content on Facebook. (Opens in a new window)
- Click to share on Telegram (Opens in new window)
Liked this:
Like
Similar
Abnormalities of the AZF locus
There is also a special region on the Y chromosome that controls the process of sperm production. This is what determines how effective spermatogenesis will be. In addition, the condition of this area affects the properties of sperm, such as the total number in the ejaculate, the ability to move, the presence of structural changes and the ability to fertilize. Only in the presence of well-formed motile sperm can male genetic material be delivered to the egg. In other words, a man’s ability to have children depends on the state of this small section of genetic code.
If there are abnormalities in the AZF locus, the process of sperm production is disrupted. As a result, azoospermia and oligozoospermia may develop. With these pathologies, the ejaculate either does not contain sperm at all, or their number is greatly reduced.
The AZF locus itself is divided into three parts with specific tasks. They are named by adding a suffix: AZFa, AZFb and AZFc. The resulting deletion can remove a fragment of a separate part, or its entirety, or capture two regions at once. With complete removal of the AZF, severe damage to spermatogenesis develops. Partial deletions can manifest themselves in different ways. At the same time, the degree of manifestation of pathology is influenced by the size of the lost fragment and its location in the locus. Therefore, for prognostic purposes, it is extremely important to know where the deletion occurred. In addition, this information can be used for proper family planning and in vitro fertilization.
If the deletion removed the entire locus or any of the regions with a/b indices, then the man cannot produce viable sperm. If the deletion can be described by the formula AZFb/AZFb+, then azoospermia develops due to severe disturbances in the process of sperm formation.
Deletions of the AZFc region lead to the manifestation of pathological symptoms of varying severity. It is also possible to develop oligospermia, which in principle allows conception. In 50-70 percent of the total number of such cases, it is possible to obtain sperm for further use in artificial insemination methods. Partial deletion of the AZFc region can be expressed in the form of various disorders from normozoospermia to azoospermia.
All deletions in the AZF locus that cause one or another pathological situation are the causes of male infertility. Determination of the mutation is possible by histological analysis of seminal fluid. In this case, it is necessary to stop sperm maturation or detect immature sperm. To obtain accurate data on deletions in the AZF locus, PCR of 6 markers is used, which relate to individual sections of the locus.
Angelman syndrome
With Angelman syndrome, a characteristic set of pathological changes develops. In particular, there is a delay in psychological development, accompanied by problems with sleep, frequent chaotic movements (mostly with the hands), constant smiling and laughter.
Pathology develops in the absence of certain genes located on chromosome 15. In this case, a mandatory condition is the transfer of a mutant copy of the gene from the mother. If the damaged chromosome is inherited from the father, Prader-Willi syndrome will develop. The karyotype is usually normal (46XX and 46XY for girls and boys, respectively). Various independent studies indicate that the disease is associated with the UBE3A gene, which normally produces an enzyme component in a complex protein degradation system.
The frequency of occurrence of the syndrome is approximately 1 case per 10-20 thousand newborns (indicators differ among different scientists).
The characteristic features of patients with Angelman syndrome are the following:
· nutritional problems that begin during breastfeeding, as children do not gain weight well (prevalence of the symptom is about 75 percent);
· inhibited development of general motor skills, that is, children begin to sit and walk later than others;
· All children are characterized by speech development disorders;
· patients usually understand more than they are able to express using a limited vocabulary;
· often the disease is accompanied by attention deficit and hyperactivity;
· problems with learning in a regular school;
· 80% of patients develop epilepsy, accompanied by disturbances noticeable on electroencephalography; Scientists believe that epilepsy is a secondary (symptomatic) disease.
· performing unusual movements, which include random chaotic movements of the limbs, small tremors;
· occurrence of attacks of laughter in the absence of visible reasons;
· characteristic walking on stiff legs, which gave rise to comparisons with puppets;
· a head reduced in comparison with the average size, often with a flattened occiput;
· in some cases, there are peculiar memorable facial features - a wide mouth with sparsely spaced teeth, a protruding chin with a protruding tongue;
· various sleep disorders;
· in approximately 40 percent of cases, strabismus develops;
· about 10% of patients also suffer from spinal curvature;
· high temperatures are perceived with increased sensitivity;
· the greatest comfort is usually achieved in water (for example, in a bath)
As a rule, the syndrome is determined using molecular genetic diagnostic methods using chromosome 15. An indication for testing for a newborn is decreased muscle tone (hypotonia), a noticeable delay in the development of speech and fine motor skills. In addition, the disease may be indicated by small tremors, jerky, erratic movements, and walking on stiff legs.
The analysis can be carried out through fluorescence in situ hybridization, DNA methylation in the 15q11-q13 region. You can also check for mutations in the imprinting center and in the UBE3A gene.
Since the disease is caused by a genetic disorder, there is no adequate and effective treatment for it. Carrying out therapeutic measures, such as massage for patients with hypotension, can improve the quality of life.
treatment
There is no cure for Angelman syndrome. The research focuses on targeting specific genes for treatment. Current treatment focuses on addressing medical and developmental issues.
A team of health care providers will likely work with you to manage your baby's condition. Depending on your child's signs and symptoms, treatment for Angelman syndrome may include:
- Anti-adhesive drug to combat seizures
- Physical therapy to help with walking and movement problems
- Communication therapy, which may include sign language and image transmission
- Behavioral therapy to help overcome hyperactivity and short attention span and aid development
Prader-Willi syndrome
This disease is determined by the same genetic mutation as for Angelman syndrome. The difference is that in this case, a violation of the hereditary material occurs on the father’s side. The karyotype is normal (46XX or 46XY). The prevalence (1 case per 12-15 thousand newborns) approximately coincides with the prevalence of Angelman syndrome.
Characteristic signs of Prader-Willi syndrome are the following symptoms:
· in the prenatal period, low fetal mobility;
· incorrect position of the fetus is common;
Possible hip dysplasia;
· by the age of two, a tendency to eat a lot (more than normal) may appear, which leads to obesity;
· low muscle tone (hypotonia), combined with impaired coordination of movements;
· feet and hands are usually small, and short stature is also characteristic;
· formation of strabismus and scoliosis;
· note increased drowsiness;
· bone density is at a lower level than in healthy people;
· saliva is thick, teeth are usually in poor condition;
· insufficient function of the gonads, ultimately causing infertility;
· later puberty compared to peers;
· patients learn to speak later and lag behind in mental development;
· external signs include a pronounced bridge of the nose, a narrow and high forehead, almond-shaped eyes, and narrow lips.
In most cases, a person with the mutation will have one to five signs of the disease.
Diagnosis of the disease is carried out by molecular genetic testing, for which children with reduced muscle tone are referred. Often, instead of a correct diagnosis, the more common “Down syndrome” is determined. An experienced geneticist who often encounters manifestations of Prader-Willi syndrome is able to diagnose it based on a set of external signs.
Miller-Dieker lissencephaly syndrome
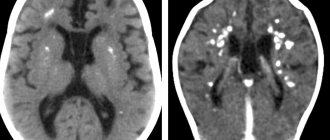
In Miller–Dieker lissencephaly syndrome, the cause of pathological changes is the deletion of certain genes in the 17p13 locus. In this case, the central nervous system suffers the most. Along with lissencephaly (smoothing of the convolutions located on the surface of the brain due to disruption of the PAFAH1B1 gene), there is a reduction in the number of cortical layers. If normally there are 6 of them, then in patients only 4 can be found. Associated signs are a noticeable change in facial shape. In addition, patients grow slowly. Attempts to integrate into society are complicated by multiple pathologies of the heart, gastrointestinal tract, and kidneys. If the disease causes a deletion of the 14-3-3 epsilon gene, the syndrome becomes much more severe.
Aniridia
With aniridia, the normal structure of the eye is disrupted: the organ of vision lacks the iris. In addition, concomitant pathological changes often develop, such as macular hypoplasia and optic nerve hypoplasia, corneal changes, and cataracts. Visual acuity noticeably drops, attempts at correction do not bring significant results. Photophobia and horizontal nystagmus develop. In some cases, congenital glaucoma appears.
The cause of the disease is a dysfunction of the PAX6 gene from the short arm of chromosome 11. The protein it encodes leads to the launch of a number of processes that control the process of proper formation of the visual organs and a number of other structures. It is noteworthy that the gene is very conservative: the difference between the forms of PAX6 in humans and zebrafish is less than 5%, despite the divergence of evolutionary lines approximately 400 million years ago.
The disease belongs to the group of autosomal dominant pathologies. In the case of homozygosity for a mutant copy of the PAX6 gene, the negative effect on the body increases, which causes multiple disturbances in the functioning of the visual organs. In addition, the central nervous system is affected, which leads to death.
Treatment is aimed at relieving symptoms. To visually imitate the pupil, it is recommended to use specially colored lenses. It is possible to restore the pupil through reconstructive plastic surgery.
DiGeorge syndrome
With DiGeorge syndrome, patients have a congenital form of aplasia of the parathyroid glands and thymus. It is a type of idiopathic isolated hypoparathyroidism. It is quite rare.
In this disease, pathological changes concern the parathyroid (parathyroid) glands, which exhibit dysgenesis or agenesis. The thymus gland (thymus) is absent from birth. As a result of the combination of such pathologies, a sharp decrease in the number of T-lymphocytes occurs, and immunological deficiency is formed. In addition, this syndrome is accompanied by the formation of congenital anomalies of large vessels.
The disease is autosomal and is determined by the presence of a mutation on chromosome 22. In most cases, the cause is a sporadic deletion of 22q11 (less commonly, microdeletion of 22q11.2). Inheritance occurs according to the dominant principle and is not related to gender. Some authors do not agree with this characterization and argue in favor of an autosomal recessive type with varying expressiveness.
The disease is characterized by disruption of the process of embryogenesis of 3-4 gill pouches, which leads to disruption of the thymus and parathyroid glands.
In the clinic, the most constant symptoms are candidomycosis and hypoparathyroidism, quite often accompanied by disruption of the formation of the mouth, nose and ears.
The thymus remains undeveloped due to developmental disorders in the embryonic period. The thymic epithelium does not support the normal development of T cells. As a result, a specific form of immunodeficiency is formed, in which the humoral immune response and the response at the cellular level are weakened. If a child has such a pathological disorder of immunity, he will have increased sensitivity to infections of bacterial, viral and fungal origin.
The syndrome can occur in the form of a genetically determined absence of the parathyroid glands or isolated insufficiency of the parathyroid glands - accompanied by hypocalcemic seizures that begin from birth. Immunological deficiency leads to the appearance of various infectious diseases. Typically, a combination of symptoms causes heart failure. In addition, infectious diseases cause death.
Diagnosis of the syndrome involves identifying pathologies typical of the syndrome: distortions of the shape of the face and skull, the presence of immunological deficiency, thymic aplasia, dysgenesis or agenesis of the parathyroid glands. The most pronounced manifestations of the disease are candidomycosis and hypoparathyroidism.
Reasons for development
The causes of Angelman syndrome are the absence of certain genes on chromosome 15. This syndrome occurs when there is a mutation in the maternal chromosome (defects in the paternal chromosome cause Prader–Wili syndrome).
In most cases, the disease is associated with the loss (deletion) of part of a chromosome.
The cause of the disease may be a spontaneously occurring defect of the 15th chromosome, which is associated with the absence of a large adjacent region in the q11-q13 region of DNA consisting of 3-4 million base pairs.
A mutation in the UBE3A gene can also cause Angelman syndrome.
Retinoblastoma
Retinoblastoma is a malignant tumor of the retina. The development process usually begins in childhood, and the starting material is tissue of embryonic origin. The peak phase occurs at two years of age.
Almost all known cases are detected during the first 5 years of life.
The cause of the disease in most cases is a mutation in the genetic material. In this case, it is necessary to have a genetic condition due to the presence of a mutant version of the Rb gene, obtained by inheritance. The second tumor-causing mutation occurs in the retinoblast.
There is a small chance that parents who have had retinoblastoma may have children with no pathological changes.
There are unilateral and bilateral cases of retinoblastoma. According to statistics, for the bilateral form the probability of hereditary origin is noticeably higher.
Symptoms of the disease include eye pain, glowing pupils, and loss of vision. It is very, very difficult to identify them in a small child.
Diagnosis usually takes the form of an examination under anesthesia using ultrasound, CT and MRI. A fairly common procedure is a red bone marrow biopsy and spinal puncture. There are 5 groups based on the severity of symptoms.
There are two effective treatment methods. With cryotherapy and photocoagulation, it remains possible to preserve both vision and the eye itself. Complications with their use rarely occur. However, if a relapse occurs, the treatment will need to be repeated in the same form. Typically cryotherapy is used in cases where the anterior retina is damaged. For the posterior region, photocoagulation appears to be the preferred option.
Arrival in Germany for diagnosis of epilepsy
Tatyana (patient’s mother): “Just 10 days after our first visit, we flew to Berlin. The next day after our arrival we went to the clinic. There we met with a translator - a very friendly girl.
We spent about 3 hours with the doctor. She looked at the MRI, observed the child’s behavior, asked in detail about the history of life and illness - from pregnancy to the present day, clarifying all the details (even the smallest), and we also had an EEG (the process itself is also very different from what we did in Russia, in a much better direction).
The doctor immediately made it clear to us what we could expect in Violetta’s life. And just two days later we were called for a detailed analysis of the child’s condition during this period and clarification of information on the diagnosis. The diagnosis was preliminary, since a genetic examination was still required (which we had already done in Russia).
We were honestly shocked when we were given a preliminary diagnosis: Angelman syndrome and epilepsy. For comparison: in Russia, doctors (there were many of them in different cities) kept repeating for 4 years that we had an atypical case of cerebral palsy (we had different forms!), epilepsy, they say, was not the same as everyone else’s (they didn’t say it frankly, but we they understood from their looks that they simply did not know how to treat). And in Germany, after three hours of communication and then reviewing the tests and examinations done during the day (in total it took 2 days), an accurate diagnosis was made!!!
It was all a shock for us. Many thanks to the doctor and the translators of GLORISMED for correct, understandable translations - this is also very important (I speak from my own experience, because I was in China and know first-hand how they translate there)! A German clinic prescribed medicine for sleep and just for the child’s normal well-being.
To select medications for epilepsy, we wanted to come later for a longer period. Due to the fact that Violetta had a very severe reaction to therapy in Russia, the selection of medications had to be carried out under the supervision of German specialists.”