General overview
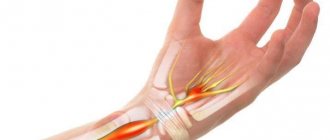
Carpal tunnel syndrome (carpal tunnel syndrome) is a set of characteristic symptoms that occur when the median nerve is compressed in the wrist, ICD-10 code: G56.0. Includes numbness, paresthesia and pain in the zone of innervation of the median nerve. These sensations may be accompanied by objective changes in sensitivity and strength in the hand.
Diagnostics
The first line of diagnosis for numbness of the fingers in our clinic is electroneuromyography, this is especially true for carpal tunnel syndrome. To make a diagnosis, a combination of characteristic clinical signs and deviations from the norm found during electroneuromyography is necessary. Electrophysiological testing can also exclude other neurological problems (for example, in the cervical spine). With this study, it is possible to assess the severity of nerve damage, which helps in choosing further treatment tactics and determines the prognosis of the disease. An ultrasound scan can reveal masses that are putting pressure on the nerve.
MRI for carpal tunnel syndrome is prescribed exclusively for preoperative planning in cases of significant joint damage or neoplasms.
Treatment
There is evidence of the benefits of aerobic exercise and weight control in carpal syndrome. A bicycle or exercise bike is not the best exercise option, as it puts constant stress on your arms.
Using physical therapy such as ultrasound may provide temporary relief.
Many people with incipient syndrome (as measured by ENMG) usually respond well to the use of a night splint to maintain a neutral hand position during sleep (minimum three weeks).
Injection (blockade) with glucocorticoids, such as diprospan, shows good results if more conservative means do not work.
Patients who do not respond to conservative methods, or those who initially present with severe disease, are referred for surgical treatment.
Surgery for carpal tunnel syndrome (CTS) involves cutting the palmar ligament, which is compressing the median nerve. The success rate is very high (more than 90%), and the risk of complications is minimal. Recurrence after complete dissection of the palmar ligament of the hand is extremely rare. Surgical success is less likely for patients with normal electroneuromyography findings.
Clinical picture
Considering the mechanism of traumatic effects on the nerve, the causes of neuritis of the radial nerve can be divided into three types.
A manifestation of radial nerve damage is a hanging limb. The process of moving the forearm, wrist, and fingers becomes difficult. Tingling, burning, numbness are felt. The hand where the radial nerve passes, from the shoulder to the dorsum of the ring finger, loses sensation.
The back of the hand swells due to inflammation of the stretched tendons.
The patient is unable to move his fingers and hand.
Ask your question to a neurologist for free
Irina Martynova. Graduated from Voronezh State Medical University named after. N.N. Burdenko. Clinical resident and neurologist of the Moscow Polyclinic. Ask a question{amp}gt;{amp}gt;
Causes and pathophysiology of the process
Before the invention of electroneurophysiological testing in the 1940s, numbness in the fingers was more often attributed to compression of the brachial plexus by the cervical ribs or other structures in the anterior cervical spine. Now we know for sure that the median nerve is compressed in the inextensible rigid carpal tunnel, demyelination occurs (damage to the sheath of the nerve ending), and then damage to the axon itself. Sensory fibers are damaged first, motor fibers later. The ultimate mechanism of injury is still a matter of debate. At the moment, it is believed that the main problem is increased pressure inside the carpal tunnel. This pressure blocks venous outflow, swelling increases and even greater compression occurs, which ultimately leads to ischemia (lack of blood supply) to the nerve. The risk of occurrence may be associated with many factors: genetic, medical, social, occupational and demographic. Various combinations of these risk factors lead to the development of carpal tunnel syndrome, but at the moment we cannot confidently name a simple and clear cause.
Functions
The radial nerve, innervating the above muscles, carries out motor functions, such as:
- Supination of the hand,
- Extension of the main phalanges of the fingers,
- Extension at the wrist and elbow joints,
- Abduction of the thumb.
Figure 2. Radial nerve. Author24 - online exchange of student work
The sensory fibers of the radial nerve are part of the nerves:
- posterior cutaneous nerve of the shoulder,
- posterior cutaneous nerve of the forearm,
- inferior lateral cutaneous nerve of the shoulder.
Sensitive fibers of the radial nerve innervate the skin on the radial side of the hand, the back surface of the shoulder and forearm, the dorsum of the first, second and part of the third finger of the hand.
Epidemiology
Disease frequency
The most accurate statistics are for the United States of America, where about 1–3 new cases of the disease are registered per 1000 people per year. On average, about 50 people out of 1000 suffer from carpal tunnel syndrome.
There is some lack of international statistics on this issue, but the prevalence of the syndrome in developed countries is similar to the United States, for example, in Holland there are about 2.5 new cases per year, and in the UK about 70-160 out of a thousand people ever seek help. Carpal syndrome is practically unheard of in developing countries, for example, among the indigenous population of South Africa.
Mortality/health threat
The disease is not fatal and cannot lead to a fatal outcome, but it can lead to serious irreversible impairment of hand function if correct treatment is not carried out.
It occurs more often in white Caucasian people.
It is believed that women suffer from carpal tunnel syndrome three times more often than men.
Peak occurrence occurs between 45–60 years. Only 10% of patients with this diagnosis are under 31 years of age.
Causes of radial nerve neuropathy
One of the main causes of neuropathy of the radial nerve of the arm is prolonged compression. This may happen due to the following factors.
– uncomfortable or incorrect posture during sleep;
– compression of the upper limbs with crutches;
– prolonged squeezing of the hand with a tourniquet;
– wearing handcuffs;
– prolonged sharp bending of the elbow while running;
– injections into the shoulder area. This is only possible if the nerve location is abnormal;
- fracture of the shoulder bone.
In some cases, radiation neuropathy of the arm is a consequence of:
– Alcohol poisoning during long drinking bouts;
– Hormonal imbalances in women and pregnancy;
– Intoxication of the body with lead;
– Past infectious diseases;
– Development of diabetes mellitus.
The cause of a violation of the radial nerve of the upper extremities can be a person’s professional activity. For example, among the sick there are a huge number of people whose activities involve physical manual labor.
Remember! There are cases where neuropathy of the radial nerve of the extremities occurs in professional athletes. Prolonged tension in the hands can lead to disruption of the functioning of nerve formations.
Symptoms of the disease
Often, the history and complaints of hand disease are more important than examination data when diagnosing carpal tunnel syndrome.
Numbness and tingling
Most often, people complain that objects fall out of their hands, their hands become “wobbly” and “weak,” needles and goosebumps can become frequent guests in their fingers.
Signs of carpal tunnel syndrome appear during certain jobs or activities:
- behind the wheel;
- when reading a book/newspaper;
- when working at a computer;
- while writing or drawing.
At night, unpleasant sensations force you to wake up and shake your brush. Some note that they need to walk around and put their hand in cold/hot water. Bilateral carpal tunnel syndrome is quite common, with the dominant hand usually affected earlier and more severely than the other.
Localization
Complaints should be focused on the palmar surface of the wrist and hand in the 1-2-3 and half of the fourth fingers, this is the zone of innervation of the median nerve. Numbness of the little finger and the back of the hand is the area of responsibility of other nerves and is not typical for carpal tunnel syndrome. Surprisingly, many patients cannot localize their symptoms and complain of numbness/weakness in the entire arm, which does not exclude this diagnosis.
Pain
Loss of sensitivity may be accompanied by burning pain in the palm, which often spreads to the fingers or along the forearm, sometimes to the elbow.
Pain in the area of the epicondyles of the elbow and higher in the shoulder or neck makes you think about other problems of the musculoskeletal system with which carpal tunnel syndrome can be combined. Identifying the causes of these pains requires a more detailed diagnosis.
Signs related to the autonomic nervous system
Patients often complain about the entire hand: a feeling of fullness, swelling of the hand and fingers; the hand may freeze or, conversely, feel hot. Many people react to the ambient temperature and do not tolerate cold well. Sometimes a change in skin color is noticed. In rare cases, there are complaints of changes in sweating in the palm. All this is associated with a violation of parasympathetic innervation, since the median nerve contains a considerable number of autonomic nerve fibers.
Weakness, lack of coordination
Decreased hand strength, especially when gripping with the thumb, often accompanies the disease. This may be due to loss of sensory response or pain. Objectively, weakness of the flexor digitorum longus and flexor digitorum profundus occurs when the median nerve is compressed above the level of the carpal tunnel. During the examination, the doctor will help determine the level of compression and choose the treatment necessary for you.
Symptoms of neuropathy of the radial nerve of the arm
The clinical picture of radial nerve neuropathies of the upper extremities will depend on the location of nerve compression.
The first type of neuropathy of the radial nerve of the arm
With this type, the armpit is damaged. The disease is popularly called “crutch paralysis.” The muscles of the forearm become immobilized and the process of impaired extension and flexion of the upper limb occurs. The triceps muscle atrophies.
Symptoms:
– Drooping of the hand when raising the arm;
– The first and second fingers are closed;
– There is difficulty in straightening the hand;
– Sensation in the fingers is lost and a state of numbness appears.
Type 2 radial neuropathy
Probably the most common radiation neuropathy of the hands. Occurs when a nerve is accidentally damaged:
– during deep sleep;
– with a shoulder fracture;
– prolonged uncomfortable position of the hand;
- when applying a tourniquet.
With strong pressure in the middle part of the forearm, there may be symptoms of neuropathy such as a feeling of numbness on the back of the hand. In addition, there is no way to straighten your fingers. However, extension movements in the forearm are preserved.
Third type of radiation neuropathy of the upper extremities
This disease involves damage to the posterior process of the nerve. This manifests itself in damage to the upper limb in the elbow area. Quite often one can observe a chronic course of neuropathy due to weakening of the joint ligaments and changes in the functioning of the hand muscles. If you straighten your elbow, you feel pain in the muscles of the forearm. Also, pain is felt when moving the hand.
There are also common symptoms of neuropathy of the radial nerve of the arm
Observing each type of neuropathy, accompanying and underlying symptoms may occur. The main symptoms have been listed above.
Associated symptoms:
– swelling at the site of the lesion;
– the occurrence of difficulties when performing motor actions with the hands;
– impaired coordination of hand movements;
– decrease in sensitivity;
– spasms and convulsions.
If you have similar symptoms and signs, you should urgently take action and begin treatment for neuropathy of the radial nerve of the hand.
What can be found during inspection?
Clinical examination is very important to exclude other pathologies of the musculoskeletal system or nervous system. Also, during the examination, you can identify characteristic signs of the disease to draw up a further examination plan.
Sensitivity tests
Changes in sensitivity can be observed along the palmar surface of fingers 1-2-3 and along the radial surface of the fourth finger. There is a Semmes-Weinstein test, a two-point discrimination test. The most commonly used test in practice is a prick test.
Sensory assessment confirms that areas outside the median nerve innervation are normal.
Strength tests
Weakening or loss of function of the following muscles: 1-2 lumbricals, oppons pollicis, flexor brevis, and abductor pollicis brevis indicate damage to the motor fibers of the median nerve distal to the carpal tunnel.
Special tests
There are no 100% reliable clinical tests to confirm carpal tunnel syndrome; a combination of them is evaluated.
- Tinel's sign. Gently tapping over the carpal tunnel causes shooting sensations in the fingers. It is the most common symptom in daily practice, despite its low sensitivity and specificity.
- Phalen's sign. Tingling/numbness occurs in the fingers when bending the wrist for 1 minute. The sensitivity of this test is 80%, the specificity is slightly lower.
- Wrist pressure test. When pressing on the wrist area with your thumb for 30 seconds, symptoms characteristic of nerve compression appear/intensify. Sensitivity 89%, specificity 96%.
- Palpation. The soft tissue surrounding the wrist is palpated for masses or other mechanical causes of nerve compression. Sensitivity reaches 90%, specificity 75% or more.
- Measurements to eliminate “square wrists”. If the thickness of the wrist in relation to its width has a proportion of more than 0.7, then the probability of developing carpal tunnel syndrome is about 70%.
Further prevention
To prevent radial nerve neuropathy, adhere to the following rules and recommendations:
- Take a comfortable position for sleeping.
- Promptly treat diseases that can provoke neuritis.
- Avoid injury to limbs.
- Lead a physically active lifestyle.
- Stick to a healthy diet and give up bad habits.
- Conduct a preventive medical examination annually.
By following all the recommendations of specialists, sensitivity and normal functioning of the radial nerve can be restored in a relatively short period of time.
Causes
It is worth mentioning from the outset that carpal tunnel syndrome can be associated with various factors. On the one hand, it can be noted that the symptoms are more pronounced after or during the load on the hand, on the other hand, it cannot be said that the load on the hand is the cause or causes the disease. Associated does not mean is the cause.
Demography:
- Elderly age
- Female
- Increased body mass index, especially after rapid weight gain
- “Square” wrist shape
- Brachymorphic type of body structure (short arms, short legs)
- Dominant hand
- White Caucasian
Many factors are inherited (“square” wrist, thick palmar ligament, body type). Also, conditions associated with carpal tunnel syndrome have a hereditary predisposition (diabetes, thyroid disease, nephropathy, neuropathy).
Diseases/medical problems:
- Fractures of the distal radius
- Acute wrist injury (sharp flexion/extension)
- Neoplasms, injuries occupying a place in the carpal tunnel (tenosynovitis of the flexors, hygromas, hematomas, aneurysms, abnormal muscles, various tumors, edema)
- Diabetes
- Thyroid disorders (usually myxedema)
- Rheumatoid arthritis and other inflammatory diseases of the wrist joint
- Recent menopause
- Hemodialysis
- Acromegaly
- Amyloidosis
Carpal tunnel syndrome due to specific stress on the hand:
- Long power grip
- Prolonged stay in an extremely uncomfortable position
- Repeating the same movements multiple times
- When using the mouse and keyboard for a long time
- Prolonged exposure to vibration/cold
Other development factors:
- Lack of aerobic exercise
- Pregnancy and breastfeeding
- Using crutches/walkers/canes
Radial nerve. Anatomy
Note 1
The radial nerve (in Latin - n. radialis) is mixed in function. The radial nerve includes motor fibers that innervate the extensor muscles of the forearm.
Figure 1. Radial nerve. Author24 - online exchange of student work
From an anatomical point of view, these muscles include:
- Muscle of the hand (extensor of the little finger, supinator, extensor of the fingers, extensor carpi radialis: long and short, long muscle that abducts the thumb),
- Elbow muscle,
- Triceps.
Are you an expert in this subject area? We invite you to become the author of the Directory Working Conditions
Instrumental/laboratory diagnostics
Laboratory tests
There are no blood tests to diagnose carpal tunnel syndrome, but they may be ordered to screen for underlying conditions (such as diabetes or rheumatoid arthritis).
Radiation diagnostics
Radiation diagnostics is not used in routine practice.
MRI of the wrist may be useful in preoperative preparation to identify the causes of mechanical compression of the median nerve. Changes in the MR signal can be observed with chronic nerve compression, but they do not yet have practical significance for determining treatment tactics for the disease.
Many specialists now use ultrasound in addition to electrophysiological research methods. Ultrasound can reveal pathological processes that occupy space in the carpal tunnel, confirm changes in the median nerve (increase in cross-sectional area), which really help in diagnosis.
Electroneurophysiological studies
Electroneuromyography is the first-line diagnostic tool for carpal tunnel syndrome. Abnormalities found on ENMG in combination with specific symptoms and tests are the key to the correct diagnosis. Electroneuromyography can also exclude other neurological disorders.
Electrophysiological studies can also determine the extent of nerve damage, which is an objective criterion for prognosis.
Carpal tunnel syndrome is usually divided into mild, moderate and severe. The ranges for these groups may vary depending on the laboratory. In general, patients with isolated sensory disorders belong to the mild group, and if motor dysfunction occurs, they move to the moderate group. Confirmation of axonal damage (markedly decreased or absent sensory/motor response distal to the carpal tunnel) indicates severe disease.
Tracking the dynamics during ENMG helps determine the further approach to the disease.
Other quantitative tests, such as thermography or vibrometry, are less informative compared to ENMG and are not recommended for practical use.
Diagnosis of neuropathy of the radial nerve of the hand
The main method for treating radial nerve neuropathy is a neurological examination. However, in order to diagnose the disease as accurately as possible, a comprehensive examination is required.
To determine the correct treatment, it is necessary to find out exactly where the injury to the upper limb occurred. At this stage, it is worth determining which nerve was damaged.
When the specialist determines that he is dealing with the radial nerve, he will prescribe the necessary set of measures, which will be aimed at determining the location of the lesion.
What is used for diagnosis?
Instrumental diagnostic measures include:
– electromyography;
– electroneurography;
– CT and MRI;
- X-ray of the affected limb.
When making a diagnosis, the attending physician takes into account the nature and causes of the disease, among which toxic, ischemic, post-traumatic, and compression lesions can be highlighted.
Additional consultations with such specialists as: orthopedist, endocrinologist, traumatologist. The doctor gives a referral to take tests for the biochemical composition of the blood, and also checks the blood sugar level.
Laboratory tests may include:
– hormonal tests;
- general blood analysis;
– blood biochemistry;
– general urine analysis.
Treatment
Physical therapy
Since carpal tunnel syndrome has been shown to be associated with obesity and low mobility, correcting these factors will help improve the condition. An exercise bike, a bicycle and other exercises requiring prolonged grip are not indicated for this disease.
The use of physiotherapy devices may provide temporary relief. For example, short-wave diathermy provides significant temporary improvements compared with placebo, including reduction in symptoms and pain, and improvement in hand function.
Ergonomics and hand therapy
Wrist braces, which keep the hands in the correct position, have been shown to be effective as an at-home treatment when used at night for a minimum of 3 to 4 weeks.
They are inexpensive and safe, so in the initial diagnosis of the disease, a neutral night splint should be considered first.
Specific muscle strengthening programs and gliding exercises have not been shown to be effective. Massage and manual techniques that improve nerve glide have no proven therapeutic effect. Changes in the ergonomics of the workplace (table, chair, body position settings), changing equipment or tools are not effective in cases where the syndrome has already been confirmed.
Making a custom tire
Most people with early stage hand tunnel syndrome respond well to conservative therapy, which primarily consists of using a night brace for three weeks. Ready-made splints from orthopedic stores can provide improvement, but individual ones are more convenient and more effective, and therefore are preferable. It can be said that a special plastic splint molded to the patient's hand (orthosis) is the best choice for the initial treatment of carpal tunnel syndrome.
Drug therapy
Steroid injections into the carpal tunnel have been shown to be effective over the long term when other treatments have failed. Blockades can be indispensable in case of contraindications to surgical treatment, for example, during pregnancy. Ultrasound measurements of the median nerve of the arm predict the effectiveness of steroid blocks. Ultrasound navigation when performing a blockade does not lead to a reduction in complications or an increase in the effect of the blockade.
Anticonvulsants such as gabapentin or pregabalin, which are prescribed for various neuropathic pain, may also be used for carpal tunnel syndrome.
Nonsteroidal anti-inflammatory drugs (NSAIDs) and/or diuretics sometimes have some effectiveness in patients with special conditions (fluid retention or flexor tendon tenosynovitis)
However, in general, for all patients with carpal tunnel syndrome, the effectiveness of gabapentin, diuretics, or NSAIDs is controversial. According to the American Orthopedic Association guidelines, systemic medications (pills, intramuscular injections, IVs) are no more effective than placebo for treating carpal tunnel syndrome. In addition, it is worth noting that supplements with B vitamins (B-6 and B-12) also do not provide proven benefits.
Treatment of neuritis
Treatment must be comprehensive. It is necessary to fight both the damaging factor and restore the damaged nerve trunk.
In treatment I use the following groups of drugs:
- Vascular;
- Anti-inflammatory;
- B vitamins;
- Improving the conduction of impulses along the nerve, etc.
Non-drug treatment methods are also used:
- Acupuncture - exposure to biologically active points of the skin leads to signal transmission along the nerve trunk to the spinal cord and brain, resulting in a complex cascade of reactions, which includes improved blood circulation, release of biologically active substances, and hormonal response, which in turn accelerates restoration of nerve fiber.
- Physiotherapy is designed to locally influence reflex zones. The main effects achieved after physiotherapy are: analgesic, anti-inflammatory, antispasmodic, fibrinolytic.
- Massage (improves microcirculation, reduces swelling).
- Therapeutic exercise (by working out muscle groups using a feedback system, the recovery period is accelerated).
To relieve pain and accelerate the recovery of nerve fibers, local injection techniques are used - therapeutic and diagnostic blockades, pharmacopuncture - with various mixtures of drug solutions, if necessary, together with ultrasound navigation. Due to the local administration of drugs (vitamins, anti-inflammatory drugs, anesthetics), it is possible to quickly relieve pain, reduce swelling and the inflammatory reaction, and restore the nerve trunk.
Surgery
Sign up for a consultation
In patients for whom conservative therapy has failed, or for those who initially come to the appointment with a severe degree of carpal tunnel syndrome (according to ENMG), there are indications for surgery. Surgical dissection of the palmar ligament is highly likely (more than 90%) to lead to significant improvement with a low complication rate. The success of surgical treatment is reduced for people with normal electromyography.
Carpal tunnel decompression surgery is performed under local anesthesia in an outpatient operating room. This operation does not require hospitalization or the participation of an anesthesiologist.
The operation can be performed using a classic wide approach, as well as minimally invasive with or without the use of endoscopic equipment. The long-term results of a correctly performed operation are comparable for different methods of intervention.
The details of the surgical intervention and its necessity in your case should be discussed with a hand surgeon.
Diagnosis of neuritis
The symptoms of neuritis are in many ways similar to the clinical manifestations of various diseases, including non-neurological ones. Therefore, the doctor should conduct a thorough differential diagnosis to make an accurate diagnosis.
Primary diagnosis consists of a thorough collection of patient complaints, identification of possible preceding factors, and direct examination of the patient. Most symptoms of neuritis are specific, so depending on their severity, the doctor can make a preliminary diagnosis.
Stimulation and needle electroneuromyography are used to diagnose peripheral nerve damage. This study makes it possible to answer the questions - which nerve is damaged, in what place it is damaged, what percentage of nerve damage, as well as give a prognosis for its recovery and monitor its recovery.
Diagnostic methods
Electroneurography is used to measure the speed of passage of nerve impulses through the fibers of peripheral nerves from their exit point to the nerve endings in ligaments and muscles. The technique allows you to determine the damaged nerve, determine the location and extent of damage, and identify the severity of the process.
Electromyography – used to study the bioelectrical activity of muscles. This method allows us to answer the question: what is the problem - damage to the nerve or damage to the muscle itself? EMG allows for differential diagnosis of neuropathy with muscle pathology (myasthenia, myotonia, myoplegia, polymyositis).
Ultrasound is a method for diagnosing damage to peripheral nerves. Evaluates changes in nerve diameter, continuity, and deterioration of sound conduction. Ultrasound clearly shows swelling of the nerve trunk and surrounding tissues
MRI – visualizes nerves and soft tissue structure, detects malignancies and provides information about muscle atrophy and nerve damage. With the help of MRI diagnostics, it has become possible to detect nerve damage in areas that are difficult to examine using electrodiagnostics or ultrasound.
Make an appointment
What to do after detection?
When conservative therapy for carpal tunnel is initially prescribed, a follow-up consultation with a specialist is required within 4–6 weeks to assess effectiveness.
Patients who have not achieved the desired result with conservative treatment should be referred for surgical decompression of the carpal tunnel.
If symptoms persist after surgery, ENMG monitoring is required.
Re-appointment of the study should be done no earlier than 3 months after surgery.
Prevention
There are no proven effective methods of prevention for carpal tunnel syndrome.
Complications
Without treatment, the median nerve continues to be damaged, leading to permanent impairment of hand function and helplessness. If left untreated for a long time, some people develop constant pain in the wrist and hand.
Forecast
Carpal tunnel syndrome usually progresses over time and can lead to permanent damage to the median nerve. Whether a conservative approach can prevent progression is currently unclear.
Even after surgical decompression of the carpal tunnel, partial return of CTS symptoms after several years is possible (about a third of patients within 5 years).
If detected early, up to 90% of patients experience improvement with conservative treatment, which does not preclude the need for surgery in the future.
Patients with comorbidities (diabetes or radius fracture, etc.) have a relatively worse prognosis compared to those who do not have such factors.
Patients with normal ENMG findings are less likely to improve after surgery compared with those with confirmed median nerve compression.
Patients with confirmed axonal injury have a poorer prognosis for complete nerve recovery.
Exercises at home
Any of the stretching or strength-building exercises listed above can be incorporated into a home recovery program. At home, patients can also use ice packs or apply heat. After completing the training, patients can also perform self-massage at home.
To date, there have been no high-quality studies examining the effects of conservative treatment as a stand-alone intervention. The literature primarily describes the effects of corticosteroids and other injections compared with placebo. Studies that showed injections were better than splinting did not examine long-term results.
A Cochrane review states that there is “silver-level” evidence that corticosteroid injections are superior to splinting for pain relief. The authors, however, acknowledge that "the evidence is based on a short-term, very small, controlled clinical trial of low methodological quality that included only pregnant and breastfeeding women."
Walker presented a case study that examined the use of manual techniques in a patient with radial wrist pain. Although de Quervain's disease was immediately ruled out, the report advocated an approach using manual techniques. Particularly for the relief of pain and dysfunction in radial, radiocarpal, intercarpal and first metacarpal joint pain.
Ashurst described a case in which a patient diagnosed with de Quervain's disease was prescribed oral anti-inflammatory drugs, a brace, and relative rest. The patient wore the orthosis at night and was instructed to text as little as possible (a series of messages always preceded the onset of pain). This case supports the prescription of relative rest, in which the patient avoids aggravating movements but remains active.
Viikari-Juntura presented a literature review and found that wearing an orthosis is an essential component of the treatment of tenosynovitis. It was found that the use of an orthosis that allowed some movement was preferable to complete immobilization of the thumb. Rest from work, according to the survey, is neither necessary nor desirable. It was also found that heat, massage, and electrotherapy were not effective in improving the patient's physical capabilities.