Causes of ulnar nerve neuropathy
Ulnar nerve neuropathy is a lesion of the peripheral nervous system, accompanied by injuries in the elbow joint.
Causes of ulnar nerve neuropathy
Common causes of ulnar nerve neuropathy include:
- Traumatic nerve damage.
- Injuries to the ulnar nerve: bruise of the arm, dislocation of the forearm, fracture of the shoulder joint, shoulder, forearm, fracture of the ulna, dislocation of the hand.
- Inflammatory or anatomical changes in structures that cause compression of the nerve in the elbow.
Ulnar nerve neuropathy is observed in the following pathologies: osteoma, sprain, deforming osteoarthritis, rheumatoid arthritis, bursitis of the elbow joint, post-traumatic arthrosis of the wrist joint.
Causes
Ulnar nerve entrapment can be caused by trauma (post-traumatic syndrome) or compression (compression syndrome or compression-ischemic neuropathy).
The post-traumatic variant is provoked by injury or sprain of joints, muscle rupture, soft tissue bruise, etc.
As for the compression option, it is primarily related to the patient’s lifestyle.
Cubital:
- sitting for a long time, leaning on the elbow (pupils or students in classes, office workers, thus putting pressure on the antecubital fossa);
- specifics of driving (many people, when driving, lean on their elbow, which is exposed to the window);
- long-term invasive effects (drip);
- frequent movements in the elbow joint (possible in some athletes).
Guillain's syndrome:
- regular use of a cane while walking;
- riding a motorcycle;
- working with tools that cause vibration and radiate not only into the shoulder, but also into the wrist crease.
The condition for the formation of a compression variant of neuropathy in Guillain’s canal is compression or prolonged (same type) impact on the wrist.
Which nerve is responsible for what? Which nerve is responsible for what?
In addition, the reasons for the formation of neuropathy may be:
- rheumatoid arthritis;
- vascular aneurysm;
- swelling (thickening of a joint or muscle);
- tenosynovitis;
- osteodystrophy;
- osteoarthritis;
- demyelinating diseases (multiple sclerosis, multiple encephalomyelitis);
- post-traumatic arthrosis;
- thickening (enlargement) of lymph nodes.
Symptoms of ulnar nerve neuropathy
Symptomatic manifestations of the ulnar nerve are accompanied by weakness in the hand, which occurs when trying to pick up something in the hand (for example, lifting a pot, kettle, frying pan), when typing on a keyboard and various similar actions. Sensory dysfunction manifests itself in the form of a feeling of numbness in the little finger, ring finger and ulnar edge of the palm. Significant discomfort is felt in the elbow joint. Pain sensations are often transmitted to the forearm along the left edge. The described symptoms intensify in the morning when placing the hand under the head or under the pillow.
Upon examination, hypotrophy of the palm muscles is observed, the appearance of the fingers resembles a clawed paw. Ulnar neuropathy in Guyon's canal is caused by similar manifestations. The main difference is pain discomfort at the base of the hand, the presence of sensory disturbances on the surface of the little finger and ring finger, while the sensitivity of the base of the hand is fully preserved.
Diagnosis of ulnar nerve neuropathy
When conducting a diagnostic study, a neurologist reveals hypoesthesia, incomplete flexion of the fingers when trying to clench the fingers into a fist, and the presence of trigger points in the area of the radial joint and radial nerve. To correctly assess the movements of the hand, the patient is asked to place the hand on the table with the palm up and, holding it pressed to the table, try to move the little finger along the edge of this table. Difficulty performing these movements indicates the presence of ulnar nerve neuropathy.
To establish damage to the radial nerve, the specialist prescribes the patient to undergo electromyography and electroneurography. Ultrasound examination allows us to determine the etiological changes in the pathology and the degree of compression of the nerve in the elbow joint. The specialist analyzes the condition of the joints and bone structures based on the results of x-rays of the elbow joint, forearm and wrist joint. Depending on the results of the study, a CT scan of the joints may be additionally prescribed.
Diagnostics
Diagnosis of this disease is carried out using a comprehensive test. Which, in addition to standard neurological tests, also includes instrumental diagnostics.
The study of the disease is carried out by a neurologist, who, at the first visit, clarifies with the patient what is bothering him and the nature of the unpleasant sensations.
Neurological tests include:
- test for bending the fingers into a fist (negative result - if all fingers come together in a fist, and positive if the little finger protrudes slightly);
- test to assess range of motion (the hand is placed on a flat surface and the patient tries to scratch this surface with the little finger and spread the pressed fingers to the sides. If there is a nervous position, this will be quite problematic);
- image of the Okay sign with your hand (a sick person will not be able to complete this test).
Treatment of elbow neuropathy
Treatment of ulnar nerve neuropathy depends on the etiology of damage to the peripheral nerves in the elbow area. Surgical intervention is required when removing tumors, neoplasms, hematomas that compress the nerve trunk or are caused by compression of the musculoskeletal canal in which it is located. Surgical treatment is also used in the absence of positive dynamics from the therapeutic measures taken.
Therapeutic treatment includes taking anti-inflammatory drugs (diclofenac, ketorolac), painkillers (metamizole sodium, anesthetic injections), nicotinic acid, B vitamins. Drug treatment is combined with physiotherapeutic procedures: UHF, magnetotherapy. To eliminate muscle atrophy, a course of massage and electrical myostimulation is prescribed.
In acute cases of ulnar nerve neuropathy, it is not recommended to perform dynamic exercise, which aggravates the pathological state of the disease. During night sleep, patients should bandage a rolled towel to the bend of the elbow joint. With a decrease in pain and a decrease in the activity of the inflammatory process, a specialized complex of exercise therapy is prescribed.
Treatment of carpal tunnel syndrome
What is the disease
Carpal tunnel syndrome is one of the little-known but quite common diseases of the peripheral nervous system.
This is a pathology of a neuralgic nature, belonging to the group of so-called “tunnel neuropathies”. The reason for its occurrence, in simple words, is pinching of a bundle of nerve fibers, which can be caused by compaction of the periarticular muscles and tendons passing close to the corresponding nerve (for example, the median or radial nerve), which can lead to its thickening or swelling. The localization of this pathology is mainly observed in the joints.
The basis for traumatic, inflammatory and degenerative changes in the joint area is most often increased motor activity. Manifestations of the disease include: prolonged pain and numbness of the damaged segment. The risk group for developing the disease includes people engaged in professional, sports or everyday activities associated with constant monotonous loads on certain areas.
Causes of pathology
The most common reason for the appearance of this neuropathy is long-term compression of the median nerve passing between the bone and tendons of a particular anatomical structure. Compression, in turn, is a factor in the disruption of blood supply in the corresponding area: arterial blood is delivered to the tissues in smaller quantities, and sometimes its flow stops altogether. Organs that have undergone trophic changes begin to go numb, and in some situations it can even lead to complete loss of sensitivity.
Risk group
Office workers, transport drivers, cashiers-controllers, musicians, hairdressers, etc. most often suffer from carpal tunnel syndrome. That is, persons whose professional and everyday activities are accompanied by prolonged homogeneous movements. The first “bells” in the form of pain and stiffness can occur in cases where the hand is in a “hanging” state for a long time (for example, among programmers or gamers when constantly working with a computer mouse). These people are susceptible to the most common type of neuropathy, such as carpal tunnel syndrome. Also, the disease can be provoked by therapeutic fasting and long-term diets, since one of the functions of the subcutaneous fat layer in the human body is shock absorption. Depletion of shock absorber fiber can lead to malfunctions of the entire anatomical structure. The provoking factors of this pathology (but of a secondary nature) are such primary diseases as various types of diabetes, gout, arthritis, kidney failure, blood diseases, as well as alcoholism, substance abuse and drug addiction. The appearance may also be caused by the consequences of medical intervention (for example, the ulnar and median nerves may be damaged as a result of frequent intravenous interventions).
The disease can also develop as a result of endocrine disorders (in particular the thyroid gland), pregnancy, during lactation and menopause in females, as well as with prolonged use of contraceptive medications. In some cases, pathology can develop as a result of hereditary predisposition (for example, due to genetically determined narrowness of the channels and increased vulnerability of nerve fibers). It should be especially noted that in women the disease occurs much more often than in men.
Types of disease
Depending on the location of the peripheral nerves affected by the pathological process, doctors distinguish the following types of syndromes:
- Muscle beds. Develops in the fascial sheaths of the extremities due to impaired blood flow in tissues compressed by muscles under external influence:
- applying plaster, splints, tight bandages;
- soft tissue bruises;
- allergic edema;
- hypothermia;
- gunshot and other wounds.
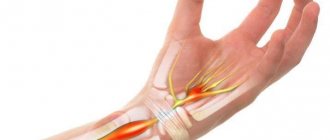
- Carpal syndrome of the wrist is a symptom complex related to the area of the hands and associated with compression of the fibers of the median nerve inside the carpal tunnel. It occurs as a result of tissue growth and narrowing of the opening of the tunnel running from the wrist to the hands. In cases of constant and strong pressure on these areas, cubital tunnel syndrome can form.
- Cubital. This is a pathology in the area of the hands, the cause of which is a disruption of the work of the hand muscles responsible for the movement of the ring and little fingers, due to pinching in the cubital canal.
- Radial nerve neuropathy is a lesion of the nerve bundle passing in the area of the elbow joint.
- Leg tunnel syndrome is a compression-ischemic lesion in the hip area.
- Piriformis muscle is a neuropathy of the sciatic nerve caused by involuntary contraction of the muscle tissue connecting the pelvic bones.
- Peroneal nerve - acute trauma to the nerve fibers located between the fibula and the muscle.
- Tarsal (Richet's syndrome) is a consequence of compression of the distal part of the tibial nerve in the internal ankle fibrous canal, which connects the ankle joint to the plantar region.
Symptoms and manifestations of the disease
In the initial stages of the disease, after prolonged monotonous movements, a weak aching painful sensation occurs, which disappears after a short break in work. If you do not pay attention to this and do not consult a specialist in time, the following symptoms may appear over time:
- constant debilitating pain;
- muscle weakness, stiffness;
- burning in the corresponding area;
- electric sensation;
- trembling in the limbs;
- decreased muscle tone;
- painful reaction upon palpation at the site of nerve projection;
- numbness;
- swelling;
- bluish tint.
Pain and paresthesia may worsen at night and can sometimes lead to sleep disturbances.
Diagnosis of the disease
Diagnosing types of tunnel syndrome is the specialization of a neurologist. During the examination of the patient, the sensitivity of the fingers and muscle strength is assessed primarily.
In addition to the appropriate tests: Phalen, Tinel, Durkan and opposition test, the following procedures are additionally performed to make an accurate diagnosis:
- electroneuromyography is an examination method that allows you to identify the degree of bioelectrical activity of muscles and nerve endings at rest and movement, as well as areas of muscle damage,
- Ultrasound to evaluate peripheral nerves. The integrity of the nerve trunk, its structure and the condition of the surrounding tissues are analyzed. Ultrasound makes it possible not only to identify voluminous neoplasms causing damage, but also to evaluate the mobility of the nerve in the tunnel during dynamic tests, the presence of scar-adhesive changes, inflammatory edema or atrophy.
Therapy for carpal tunnel syndrome in our clinic
To effectively treat the pathology, it is necessary to understand the cause and mechanisms of compression and apply an integrated approach.
A neurophysiological study is required to confirm nerve damage - electroneuromyography (ENMG) or ultrasound.
Conservative therapy
This method consists, first of all, of fixing the limb in a functionally advantageous position in order to eliminate physical impact in the area of compression and achieve maximum unloading. For this, there are special devices, such as polymer bandages, tight bandages and orthoses.
Along with orthopedic correction, drug therapy is used, including NSAIDs, anti-inflammatory drugs, analgesics, B vitamins, antioxidants, and substances that improve blood circulation. Chondroprotectors or symptom-modifying drugs containing glucosamine and chondroitin sulfate are widely used. They have an analgesic and antiseptic effect, which develops slowly, but are devoid of the side effects characteristic of non-steroidal analgesics, since the mechanism of their work is associated with blocking nuclear factor kB, which is an important link in the breakdown of cartilage. Treatment with chondroprotectors allows you to gradually significantly reduce the doses of prescribed analgesics, up to complete abandonment of them.
The fastest and most effective way to relieve pain is to inject glucocorticoids directly into the canal or tissue surrounding the nerve. Glucocorticoids have an anti-inflammatory and anti-edematous effect in tissues, and also have a remyelinating effect in cases of damage to nerve fibers. The interval between such administrations should be at least 2 weeks. The choice of medications and treatment methods depends on the cause of the syndrome and the stage of its development.
Of the physiotherapeutic techniques, the most effective are laser therapy, ultrasound with glucocorticoids on the area of compression, electrophoresis with lidase for adhesions and shockwave therapy. They can be used both during drug treatment and for rehabilitation after surgery. Manual therapy methods are also used to influence the mechanism of hyperfixation of the nerve by reducing the scar-adhesive process in the tunnel.
In persistent cases of this syndrome, or when conservative methods are of little effectiveness, surgical intervention is performed: expanding the lumen of the canal and releasing the ischemic branch by dissecting the compressive structures.