In this article we will tell you:
- Symptoms of anisocoria
- Classifications of anisocoria
- Physiological and pathological anisocoria
- Congenital and acquired anisocoria
- Diagnosis and treatment of anisocoria
Anisocoria is present in 20% of the world's population, however, in most cases it is a physiological disease. A person with this diagnosis has pupils of different diameters
. It looks unusual, but physiological anisocoria does not pose a health threat.
It’s another matter when the condition is accompanied by unpleasant symptoms: photophobia, double vision, pain, decreased visual acuity. In this case, consultation with an ophthalmologist and selection of effective therapy is indicated. Pupillary anisocoria may be an important diagnostic criterion indicating ocular or nervous system involvement. The disease can occur at any age, most often in young females. If a child suffers from the pathology, there is a high risk of developing various refractive errors.
About physiological and pathological anisocoria, signs, causes of anisocoria in adults and treatment methods - in our article.
So,
anisocoria
is an ophthalmological symptom in which a person’s pupils are asymmetrical (that is, they have different diameters)
. In this case, one eye functions normally, and the other reacts to light in a pathological way, not expanding or contracting as in a normal, healthy state.
Symptoms of anisocoria
Anisocoria can be asymptomatic, but can bring many unpleasant minutes, causing:
- dizziness, headaches;
- decreased visual acuity, appearance of spots before the eyes, diplopia (double vision);
- nausea leading to vomiting;
- motor dysfunctions: paresis and partial paralysis, hand tremors;
- impaired coordination of movements.
In addition, anisocoria leads to:
- increased eye fatigue, especially during exercise;
- drooping, drooping of the upper eyelid – so-called ptosis;
- corneal edema, pain;
- deterioration of eyeball mobility;
- protrusion of the eyeball forward. This phenomenon is called “proptosis”.
Symptoms
Depending on the cause leading to anisocoria, certain symptoms of damage to the nervous system are determined. Signs of pyramidal insufficiency, cerebellar damage, etc. may be detected.
In all cases of anisocoria, even if not accompanied by other symptoms, an MRI examination in vascular mode or MSCT with contrast enhancement of vessels is recommended, because the most common cause of anisocoria is an aneurysm or a brain tumor.
Also, only a neuroimaging study allows one to determine further tactics and help resolve the issue of the need for urgent neurosurgical intervention.
Classifications of anisocoria
There are several classifications of this condition.
Physiological and pathological anisocoria
With physiological anisocoria, the difference in pupil size is observed more often at rest, and the diameter of the affected pupil does not differ from the healthy one by more than 1 mm and does not depend on the level of illumination.
Physiological anisocoria is characterized by the disappearance of symptoms when using special drops that dilate the pupil.
Pathological anisocoria signals a malfunction in the body: ophthalmological or neurological diseases. The pupil can contract and dilate depending on the brightness of the light.
Congenital and acquired anisocoria
Congenital anisocoria is a consequence of genetic diseases, disorders in the embryonic development of the nervous or muscular apparatus of the eyes. Often accompanied by strabismus and may disappear with age. If the condition does not go away, it usually does not affect the quality of vision in adulthood.
Causes of acquired anisocoria:
- neurology;
- disturbances in the functioning of the nervous system;
- migraine (impaired pupil symmetry occurs as a result of swelling of brain tissue);
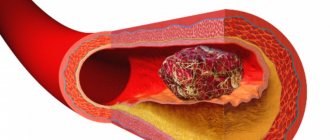
- vascular diseases of the brain, strokes, cerebral infarctions (in this case, anisocoria is one of the symptoms and is usually accompanied by increased blood pressure, vomiting, nausea, headache, impaired motor function, loss of coordination);
- injuries of the iris, ligaments of the eye apparatus, brain;
- foreign body getting into the eye;
- oncological diseases of the brain;
- eye surgery (for example, cataract removal);
- inflammatory eye lesions (iritis, iridocyclitis);
- brain infections (meningitis, encephalitis, etc. - with these diseases the functionality of the nuclei of the optic nerves suffers);
- taking certain medications;
- drug use;
- tuberculosis of the upper lungs;
- glaucoma;
- paralysis and paresis of the oculomotor nerve of various origins.
In addition, the cause of different pupil sizes in an adult can be:
- Horner's syndrome. This symptom complex is characterized by lesions of the sympathetic nervous system. In addition to ophthalmological ones, it also causes vascular tone disorders and sweating.
- Argyle Robertson syndrome. The cause of the phenomenon in which the pupils stop responding to changes in lighting is often infection of the organ of vision due to neurosyphilis and neuropathy of diabetic origin.
- Holmes-Adie syndrome. With Adi syndrome, abnormal mydriasis (dilation) of the pupil is observed, accompanied by impaired sweating, twitching of the limb, and farsightedness. Occurs due to viral or bacterial inflammation of postganglionic fibers.
- Parinaud's syndrome. The cause of the disease is damage to the posterior parts of the midbrain due to tumors, injuries, and multiple sclerosis.
Causes
This pathology can occur due to injury to the eye, parasympathetic fibers that innervate the muscle that constricts the pupil, or sympathetic fibers that innervate the muscle that dilates the pupil.
Anisocoria occurs when the muscle that is responsible for constricting the pupil is damaged. The pupil first narrows, then dilates, and is no longer able to respond to accommodation and light. Typically, a shrinking pupil causes iritis (inflammation of the iris).
If anisocoria intensifies in the light, then this is the cause of parasympathetic excitation of the eye - mydriasis (dilation of the pupil) appears, and any reactions of the pupil decrease. In most cases, the main cause of this problem is damage to the oculomotor nerve, in which the manifestation of mydriasis can cause limited movement of the eyeball, double vision, ptosis, and divergent strabismus. The cause of damage to the oculomotor nerve can be an aneurysm, tumor, acute cerebrovascular accident and other severe brain lesions.
Another cause of parasympathetic denervation may be damage to the ciliary ganglion in the orbit due to infection (herpes zoster) or damage of another nature (including traumatic brain injury). In this case, the pupil loses its reaction to light, but a delayed reaction to convergence and accommodation remains. When looking into the distance, the pupil slowly dilates; doctors call this the “tonic pupil.” In the case of Eydie syndrome, a characteristic feature of which is the degeneration of parasympathetic neurons of the ciliary ganglion, such a pupil is combined with blurred vision, which means a violation of accommodation, and a diffuse decrease in tendon reflexes.
If anisocria increases while moving away from light or even in the dark, we can conclude that the patient has either simple anisocoria or Horner's syndrome. This syndrome occurs as a result of damage to the sympathetic innervation of the eye, most often with lesions of the brain stem, and is characterized by miosis and ptosis of the upper eyelid. The position of the eyelids gives the impression that the eye is deep in the orbit. The pupils react normally to accommodation, convergence and light. In most cases, the main causes of damage to sympathetic fibers are large lymph nodes in the neck, cervical “rib”, tumors at the base of the skull in the orbit, and thrombosis of the carotid artery. Simple anisocoria occurs most often and is characterized by a slight difference in pupils.
Diagnosis and treatment of anisocoria
An ophthalmologist will be able to make a diagnosis of “anisocoria” based on examination, studying the reaction of the pupils in the dark, in the light, studying the speed of their reaction, and symmetry under different conditions.
In addition, a biomicroscopic examination, diascleral transillumination using a diaphanoscope, and, if necessary, angiography, ultrasound, MRI and CT will be performed. The doctor can also use mydriatics - special drops that can cause artificial dilation of the pupil.
There are also special tests - tropicamide and phenylephrine and pilocarpine - to help make the diagnosis.
Physiological anisocoria, which does not cause any problems to the patient, does not require treatment. Only a cosmetic defect can cause inconvenience.
For anisocoria associated with diseases of the body, treatment consists of eliminating the underlying disease.
Pupil: what is it and why does it change size
The pupil is the hole in the iris of the organ of vision in humans and animals. It is through it that light streams enter the eye.
The size of the pupil directly depends on the functioning of the autonomic nervous system and is determined reflexively under the influence of various factors. First of all, this is the brightness of the lighting: the darker the room, the more the pupil dilates. Also, its diameter can be affected by pain or emotional sensations, or taking certain medications.
The pupil contracts and dilates due to the coordinated functioning of the iris muscles, which receive appropriate signals from the oculomotor nerve. Normally, they act synchronously (for example, if you direct light to one eye, the pupils of both will decrease in diameter equally) - this is a feature of the human organ of vision. The size of the pupil changes dynamically; over the course of a minute it is capable of making from 30 to 120 vibrations, and the diameter can vary from 1.1 to 8 mm.
A difference of within 1 mm is normal for human pupils. This is physiological anisocoria, it is observed in approximately 20% of the population (the vast majority of them note that the right pupil is wider than the left).
to contents ^
How is anisocoria treated?
There is no pathological process underlying physiological anisocoria, so no treatment is required.
Treatment for pathological pupillary asymmetry depends on the cause that provoked this condition. For inflammatory (both ophthalmological and extraocular) pathologies, local and systemic antibacterial agents, corticosteroid drugs, as well as agents that normalize water-salt balance are prescribed.
If tumor processes or brain hemorrhages are detected, surgical intervention may be required.
With anisocoria, it is unacceptable to self-medicate by prescribing eye ointments and drops for yourself and using folk remedies. The therapeutic regimen is determined by the doctor based on the results of diagnostic procedures.
to contents ^
Anisocoria in children and adults
At different age stages, the causes of pupillary asymmetry may differ.
In children, anisocoria is often congenital, especially if this has been observed in someone in the family: in this case, they speak of a genetic predisposition. This condition is often observed from the moment of birth and may be accompanied by strabismus.
An acquired form of anisocoria in childhood can develop due to underdevelopment of the autonomic nervous system. If this is the reason, then by the age of 4-5 years the difference in pupil diameter is gradually leveled out.
It happens that uneven pupils in a child appear as a result of falling and hitting their head on a hard surface, as well as due to birth trauma.
Different pupils can become a reaction of the child’s body to the use of eye drops, poisoning with toxic substances, or intoxication after an insect bite (tick-borne encephalitis).
Anisocoria in children can accompany infectious diseases (meningitis, meningoencephalitis).
A child with a visually noticeable difference in pupil size should be shown to a doctor to exclude the possibility of serious pathologies. Sudden anisocoria should be especially alarming.
In adults, ophthalmological and neurological diseases come to the fore as causes of pathological pupillary asymmetry. If anisocoria appears in adulthood, it is important to be vigilant, as it may indicate problems with the brain.
to contents ^
Ophthalmic diseases
Among eye diseases, iritis or iridocyclitis are common causes of the development of anomalies. In this case, the work of the oculomotor muscles is disrupted, their spasm occurs, which affects the normal reaction of the pupil.
Glaucoma can lead to miosis (narrowing), since by reducing the opening, the outflow of fluid from the anterior chamber improves, which reduces the pressure inside the eyes. With a tumor or neoplasm in the area of the visual center, it can compress the nerve fibers, which leads to two consequences: miosis, if sympathetic innervation is weak, or mydriasis (dilated pupil), if parasympathetic innervation is insufficient.
Diagnosis of anisocoria
Your ophthalmologist will examine your pupils in both a bright room and a dark room. This allows the ophthalmologist to see how your pupils react to light. This in turn can help them figure out which pupil is abnormally sized.
The ophthalmologist will also analyze the visible parts of the eye using a slit microscope (slit lamp). This tool will allow your eye doctor to examine your eyes in detail and detect the problem.
Slit lamp examination can provide additional information about concomitant or coexisting eye diseases. Congenital, traumatic, and surgical causes of anisocoria are often associated with other structural defects. The anterior chamber may be examined for signs of iritis or uveitis. Abnormal gonioscopy and tonometry results may indicate angle-closure glaucoma. The clinical picture of Adi's tonic pupil when examined with a slit lamp may show paralysis of the iris sector and vermiform movement of the iris.
A detailed neurologic examination is also important to localize lesions, look for associated signs of cranial nerve involvement, and evaluate focal neurologic deficits in sensory, motor, and deep tendon reflex pathways.
A thorough history to ascertain the onset and chronicity of anisocoria will also be helpful in determining its etiology.
Chronic anisocoria without associated symptoms may indicate a benign process such as physiological anisocoria, whereas sudden anisocoria with the onset of other symptoms may be more concerning. For example, anisocoria with headaches, confusion, altered mental status, and other focal neurologic deficits suggests an underlying mass effect and may require further neurologic evaluation and intervention.
If you have other symptoms along with changes in pupil size, your ophthalmologist will do further tests to learn more about your condition.
TREATMENT
How to treat anisocoria? Since anisocoria is not an independent nosological entity, there is no protocol for its specific treatment. In this case, we are talking about eliminating the factors that led to the loss of the pupil’s ability to expand or contract. In many cases, patients require the help of an experienced neurologist, especially if the difference between the diameter of the pupils of both eyes is more than 2 mm.
Perhaps, after analyzing the data obtained during the examination, doctors will consider it necessary to perform an operation
, and the patient should decide to do so. Usually, misalignment of the eyes in this case is accompanied by other severe symptoms - severe headaches and mental disorders, which indicates dangerous processes occurring in the brain. This situation occurs with serious head injuries, possibly with a violation of the integrity of the skull.
More often, doctors limit themselves to prescribing medications:
- corticosteroids;
- anti-inflammatory;
- antibacterial agents.
In this case, the main efforts are directed towards combating the underlying disease, which thus affects the pupils and can cause even more harm.
If the results of all examinations indicate ocular anisocoria associated with eye trauma, ophthalmological treatment is carried out. Experts prescribe medications to relax the iris muscle
, for example, anticholinergic substances used in the treatment of iritis and iridocyclitis.
At the same time, when treating anisocoria, doctors fight inflammation, which together gives good results.
With congenital anisocoria, everything depends on the intensity and severity of the mismatch. In many cases, the problem can be corrected with surgery. But sometimes it doesn’t make sense, and then the patient has to regularly use eye drops prescribed by the doctor. In this case we are also talking about a rare phenomenon.
How to treat anisocoria
Physiological anisocoria does not affect vision or eye health. Therefore, it does not require treatment.
With pathological anisocoria, the cause of the appearance of different pupils is first identified. Then they carry out treatment.
For example, for a brain infection, treatment is carried out in a specialized hospital. A course of antibiotics and antiviral drugs is prescribed.
Head tumors and aneurysms of the head vessels require surgical treatment.
For glaucoma, treatment is aimed at normalizing eye pressure and preventing the development of glaucoma attacks.
In case of inflammatory eye diseases, a course of treatment with antibiotics is carried out.
For eye tumors, surgical treatment is indicated.
Symptoms
A slight difference in the pupils is only a cosmetic defect and does not in any way affect the condition of the eyes or vision function.
If the difference is pronounced, the following symptoms appear:
- decreased visual acuity;
- distortion of the visible image;
- impaired orientation in the area as a result of a failure of spatial perception;
- headaches, dizziness, sometimes migraines, which can only be eliminated temporarily;
- rapid eye fatigue when working at a computer, while reading, watching TV;
- motor activity of the eyeballs, worsening general well-being.
Clinical signs are individual and depend on the cause of the disease. In neurological syndromes, signs of visual impairment are more pronounced in poor lighting conditions, darkened rooms, and twilight. From the pathological side, the iris is noticeably lighter. With simultaneous paralysis of the oculomotor nerve, double vision appears in the eyes, and the eyelids close with difficulty. Severe pain occurs in the orbit.
What is anisocoria?
Simply put, anisocoria is a difference in the size of the pupils of the right and left eyes. One pupil may be larger than normal or smaller than normal. This results in different pupil sizes. In general, the reaction of the two pupils to light may or may not be normal.
In most cases, anisocoria is a benign condition, so there is no cause for concern. However, if your pupils suddenly become different sizes, you have a rare type of anisocoria that may be a symptom of a serious medical condition.
Preventive actions
Preventing the occurrence of differences in pupil size through any preventive measures has not been established.
People at risk should pay special attention to their eyes, namely:
- people actively involved in sports, especially those types where there is direct contact (boxers, hockey players, tennis players, etc.);
- people who, due to the nature of their professional activities, often have to be in situations where the face, skull, and cervical vertebrae may suffer (builders, firefighters, miners, etc.).
They must not neglect personal protective equipment for the body, especially the head and neck.
And, of course, the main preventive measure is maintaining a healthy lifestyle and getting rid of drug and alcohol addiction.
The conclusions to be drawn from this article are based on a simple rule. You should always take your health seriously. The body often sends us calls about some failures in the coordinated work of all organs. They cannot be ignored. Otherwise, irreversible consequences of our inattention to ourselves will occur. Of course, manic concern for one’s health is an extreme. But how many times, banal professional examinations, revealed diseases in people that they did not even suspect. This fully applies to anisocoria. Take care of your eyes.
What to do if anisacoria is detected?
What should be done if eye asymmetry is noticed? Regardless of the age of the patient, whether he is an infant or an adult, the causes of anisacoria are first identified.
It is necessary to clearly understand that no medicinal herbs or other methods of self-medication will help correct different pupil sizes. After a thorough examination of the eye, if necessary, the doctor may prescribe the following examinations to exclude serious diseases:
- blood test;
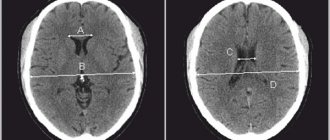
- CT scan of the brain;
- cerebrospinal fluid examination;
- magnetic resonance imaging;
- X-ray.
What diagnostic methods are used if the pupils are of different sizes? In order to prescribe the correct treatment, you need to make an accurate diagnosis. If it is difficult to find out under what circumstances a given pathology occurred, old photographs of the patient are sometimes used in diagnosis to approximately understand the duration of the disease.
There is also a diagnostic method for unilateral anisocoria, during which the sensitivity of the pupil to light and its reaction in the dark are detected.
This examination reveals the following: if anisocoria is more pronounced in the dark, this means that the patient has a smaller pupil, since its ability to dilate is impaired.
With anisocoria, which manifests itself in the light, the pupil that is larger in size is pathological, since its ability to narrow is impaired.
For example, if a person has unequal iris openings and complains of pain in the eyes, the doctor may conclude that there may be a problem with the cranial nerves.
To do this, you need to refer the patient for an examination of the brain and skull. If one pupil is larger than the other and the eyeball protrudes forward (proptosis), then treatment will be aimed at correcting hormonal disorders in the body.
What are pharmacological tests? These are tests that are carried out using special solutions to clarify the diagnosis.
- Cocaine test. For adults, a 5% cocaine solution is instilled into the eyes, and for children - 2.5%. If there is no pathology, then the pupils will dilate evenly to 1 mm. When the hole in the iris is affected, expansion occurs up to 1.5 mm. The holes are measured before the test and then after instillation one hour later.
- Tropicamide and phenylephrine tests. For the procedure, 1% solutions of these drugs are used. The result of this test is visible within 45 minutes. Pathology is considered to be both pupil dilation up to 0.5 mm and more than 1.2 mm.
- Pilocarpine test. After instilling Pilocarpine, the result is visible within half an hour. A healthy pupil should not react to the solution.
Treatment will be effective if you pay attention to the problem at the initial stage. Very often, the ophthalmologist carries out treatment together with a neurologist and neurosurgeon
When should you not worry? It is considered common practice that the pupils should be symmetrical. And when, to great surprise, people notice iris holes of various sizes, they attribute this to pathology.
But such a phenomenon may simply be an individual feature, such as far or close-set eyes. If there is a slight difference in the size of the pupils, but the person sees normally, then this cannot be considered a pathology.
So, to be completely confident in your or your child’s health, if you notice differences between your pupils, get examined by an eye doctor. If an infectious disease of the body is detected, antibacterial therapy will be prescribed. If a tumor is detected, treatment is surgical.