Optic neuropathy is a dangerous pathology that can lead to vision loss. The disease is not independent and often becomes a consequence of other diseases. From this article you will learn all the details about this condition: its forms, causes of development, signs, as well as features of diagnosis and further treatment.
In this article
- What is optic neuropathy?
- Symptoms of optic neuropathy
- Anterior ischemic optic neuropathy
- Posterior ischemic optic neuropathy
- Diagnosis of optic neuropathy
- Treatment of optic neuropathy
General information
Ischemic optic neuropathy is a disease of mature adults. It most often occurs in patients aged 40-60 years, and most often in men. This is a fairly dangerous condition for health, which can cause serious loss of vision, even complete blindness. Ischemic neuropathy is not an independent disease; it occurs as a manifestation of various processes in the body. The cause of neuropathy can be both ophthalmological problems and cardiac, neurological, rheumatological, hematological and endocrinological abnormalities.
What is optic neuropathy?
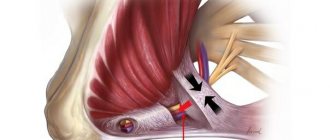
One of the most important elements of the structure of the eyeball is the optic nerve. Its anatomy is quite complex and is of great importance in ensuring clear vision. The optic nerve transmits nerve impulses from the eyes to the brain and back. The condition of the intrabulbar region plays an important role in this process. It is located within the eyeball from the vitreous to the outer layer of the sclera. Due to impaired blood circulation in the intrabulbar region, the optic nerve is damaged. Its tissues receive less nutrients that are necessary for normal functioning. The consequence of this is eye neuropathy.
Pathology usually develops in people aged 50-60 years. Most often, men are affected by this disease. This is a dangerous condition that can lead to decreased vigilance, impaired peripheral vision, “color blindness,” and the formation of scotomas—dark spots that impair visibility. The most serious consequence of the pathology is complete blindness. Optic neuropathy is not an independent ophthalmological disease. This is one of the manifestations of other diseases. Doctors include these:
- atherosclerosis;
- diabetes;
- cardiac dysfunction;
- rheumatoid arthritis;
- hypertension.
The second name for optic neuropathy is neuroopticopathy or ischemic neuropathy. This condition is easily confused with neuritis. In fact, these are different pathologies and it is very important to distinguish them. In order not to confuse ocular neuropathy with other disorders of the visual organs, it is important to know the reasons for the development of this condition, its characteristic signs, methods of diagnosis and treatment.
Causes
Anterior ischemic neuropathy is expressed in impaired blood flow in the posterior ciliary arteries and, as a result, ischemia of the retinal, choroidal and scleral layers of the optic disc develops. Posterior ischemic neuropathy occurs in the process of circulatory disorders in the posterior parts of the optic nerve and stenosis of the carotid and vertebral arteries.
The disease is caused by various lesions and associated disorders, striking changes in the vascular bed, and microcirculation disorders. Neuropathy develops against the background of common vascular diseases: atherosclerosis, hypertension, temporal giant cell arteritis, periarteritis nodosa, obliterating arteritis, diabetes mellitus, cervical discopathy with disturbances in the vertebrobasilar system, thrombosis of the great vessels.
In individual cases, the disease can manifest itself as a result of serious blood loss during gastrointestinal bleeding, surgical interventions, injuries, anemia, arterial hypotension, after anesthesia, hemodialysis, and blood diseases.
Origins and reasons
The occurrence of ischemic eye diseases is associated with the spread of hypertension, atherosclerosis, diabetes mellitus and coronary heart disease. Other existing problems of the visual analyzer may also play a role. However, despite its prevalence, there is still no classification of ocular ischemia. Systematization is difficult due to the very origins of the disease: it can appear in any person who is faced with damage to certain elements of the circulatory system. Thus, ischemic eye diseases are characterized by polyetiology (multi-causality), variability of clinical course, difficulty in determining the general properties and features of the processes that determine the occurrence, course and outcome of the disease.
Symptoms
When the disease develops, one eye is most often affected; bilateral impairment is observed in only a third of patients. As a rule, the second eye begins to be involved in the ischemic process after a period of time, from several days to several years. On average, the process takes from two to five years.
As a rule, the disease develops completely suddenly. The trigger, most often, is quite ordinary actions: after waking up, physical activity, or a hot bath. Visual function sharply decreases (even to the point of blindness). This happens in a short period of time, from several minutes to hours. Often preceded by warning symptoms, such as systematic blurred vision, pain in the area behind the eye, and severe migraines.
The pathology also manifests itself in serious impairment of peripheral vision. Individual defects may also appear, such as loss in the lower, temporal and nasal half of the visual field, narrowing of the visual fields.
Acute ischemia lasts about four to five weeks. Next, swelling of the optic disc begins to gradually subside, hemorrhages gradually resolve, and then optic nerve atrophy occurs.
Symptoms of optic neuropathy
Pathology is characterized by rapid development. It comes suddenly. The main symptom of this disease is decreased vigilance. Visual impairment resulting from neuropathy is usually temporary. Visibility problems can last from 10-15 minutes to several hours. In many people, neuropathy causes impairment of light perception, the main function of the rod apparatus of the retina. This usually happens with mild lesions of the optic nerve. If the damage is more serious, then complete blindness can suddenly occur. The main symptoms of this condition include:
- Pain in the eyes;
- blurred vision;
- color vision impairment;
- tunnel vision;
- headache.
Narrowing of the visual field, loss of parts of the image, impaired color perception - all these are symptoms that characterize neuropathy. Integrity is very important to the optic nerve. If it is disrupted, a condition such as atrophy may occur. This is the name for complete or partial destruction of the optic nerve fibers. With incomplete atrophy, vision is not completely reduced. This is due to the fact that the nerve tissue is affected only in a certain area. This condition often leads to problems with peripheral vision - vision outside the focus of attention is impaired. The completeness of the image is interrupted by scotomas - “blind” areas in the field of view.
Treatment
Treatment of ischemic optic neuropathy is extremely necessary to begin from the first hours from the onset of the pathology, since long-term circulatory disorders necessarily cause massive death of nerve cells. Primary, immediate care in case of sudden development of ischemia includes the urgent administration of aminophylline solution intravenously, taking nitroglycerin under the tongue, as well as inhaling vapors of medical ammonia. Further treatment of neuropathy is carried out inpatiently.
Treatment in a hospital is aimed directly at relieving swelling and subsequent normalization of the functionality of the optic nerve by creating bypass pathways for blood flow. Of great importance in successful treatment is solving the problem of the underlying disease, normalizing the parameters of the coagulation system and lipid metabolism, and correcting blood pressure levels.
In the event of ischemic optic neuropathy, a course of diuretics such as diacarba and furosemide, nootropic and vasodilators, anticoagulants and thrombolytic drugs, corticosteroids, and a course of vitamins B, C and E are mandatory. Next is electrical stimulation, magnetic therapy, laser stimulation optic nerve fibers.
Modern methods of treatment of chronic ischemic optic neuropathy of vascular origin
Vascular diseases of the optic nerve are one of the most important problems in ophthalmology. Despite the undoubted successes achieved in recent decades in the diagnosis and treatment of ophthalmological diseases, the number of patients with damage to the optic nerve of vascular origin is increasing. The article analyzes modern methods of treating chronic ischemic optic neuropathy of vascular origin.
According to foreign and domestic data, impaired blood circulation in the vessels supplying the eyeball is associated with pathology of the cardiovascular system. Often this condition is accompanied by chronic cerebral failure, coronary heart disease, arterial hypertension, that is, diseases whose pathogenesis is based on ischemia [1–3].
The lack of timely prevention and treatment of pathologies of the cardiovascular system leads to ischemia and hypoxia of the eye membranes and, as a consequence, to impaired visual functions [4, 5].
Despite significant progress in the prevention and treatment of cardiovascular diseases, 17.9 million people died from this pathology in 2021. Moreover, 85% of deaths were caused by a heart attack or stroke [6]. At the beginning of 2014 in Russia, partial atrophy of the optic nerve (ON) in visually impaired people, not the result of glaucomatous optic neuropathy, was 14% [7]. Therefore, the issue of chronic vascular insufficiency of the optic nerve remains extremely relevant.
In 1991 I.A. Eremenko proposed to classify chronic vascular optic neuropathies into chronic vascular insufficiency of the optic nerve, simple sclerotic atrophy of the optic nerve and sclerotic atrophy of the optic nerve with pseudoglaucomatous excavation [8].
In chronic vascular optic neuropathies, the disease begins gradually, often unnoticeably. The initial stage of the disease - chronic vascular insufficiency of the optic nerve is ophthalmoscopically manifested by mild pastosity of the disc of the optic nerve with a slight blurring of its borders. Peripapillary choriofibrosis is noted in the form of an atrophic rim. At the same time, retinal angiosclerosis and sclerotic macular degeneration (usually dry) are determined. Visual functions are high: in 50.6% – from 0.6 to 1.0, concentric narrowing of the visual field by 20–30° [9]. Gradually (over several years) the process moves into the next stage – sclerotic atrophy of the optic nerve, which is accompanied by a progressive decrease in visual functions [9–12]. Simple sclerotic atrophy of the disc is characterized by the appearance of monotonous pallor of the disc and the clarity of its boundaries. Peripapillary choroid atrophy is observed in 81.8% of patients, often sclerotic macular degeneration. Visual acuity is within 0.3 ± 0.09, the field of view is narrowed to 40–25° [9, 10]. Sclerotic atrophy of the optic nerve with pseudoglaucomatous excavation resembles the picture of glaucoma: the disc acquires a grayish tint, there is extensive, up to 1/2–3/4 PD, undermined excavation and a shift of blood vessels to the nasal side. In 75.3% of cases, severe sclerosis of the choroid is observed in the posterior pole, paraequatorially and around the disc. Visual acuity, as a rule, does not exceed 0.1–0.3, concentric narrowing of the visual field reaches 30–15° [9]. Testing for glaucoma rules it out. At the same time, as with simple sclerotic atrophy of the optic nerve, a decrease in the diastolic pressure of the central retinal artery, rheoencephalo- and ophthalmographic coefficients is observed [9, 10]. Apparently, for the occurrence of pseudoglaucomatous excavation, the decisive role is played by the degree of hemodynamic disturbances in small postlaminar vascular branches and the imbalance between the blood supply to the optic disc and the level of intraocular pressure (even when the latter is normal) [12–14].
Conservative methods of treating chronic ischemic optic neuropathy have been known for a long time and are aimed at reducing local ischemia and hypoxia. Currently, metabolic, vasoactive drugs, neuroprotectors, angioprotectors and microcirculation correctors, antioxidants and nootropic drugs, as well as antioxidant vitamin-mineral complexes are widely used [4]. However, conservative treatment does not allow full and stable restoration of lost visual functions.
The ephemeral nature of conservative therapy and physiotherapeutic methods has prompted ophthalmologists to search for the most effective ways to improve ocular circulation. Various surgical methods have been developed to correct ocular circulatory disorders, which have contributed to the improvement of retinal hemodynamics and optic nerves.
Modifications of choroid revascularization operations aimed at creating additional collateral blood supply to the inner membranes of the eye have become widespread. The operations were performed using extraocular muscles, an episcleral flap, pieces of donor sclera, viscoelastic, with the introduction of neuroprotective and vasoactive drugs, and sub-Tenon implantation of a collagen infusion system [15–17]. The duration of the therapeutic effect reached six months.
A.I. Eremenko [18] used long-term intracarotid infusion of drugs for chronic vascular optic neuropathy: through a catheter inserted into the superficial temporal artery (STA) before the bifurcation of the carotid artery, a multicomponent infusate was infused around the clock for 5–7 days (the daily dose included 1000.0 saline solution, 15.0 - 2% trental, 15,000 units of heparin, 15.0 - 2.4% aminophylline, 40 mg prednisolone, 150.0 - 0.5% novocaine). Against the background of such infusion, an increase in visual functions was noted in 92.3% of patients (with simple sclerotic atrophy of the optic nerve: Vis - by 0.15 ± 0.02, visual field - by 68.8 ± 14.9°; with atrophy with pseudoglaucomatous excavation : Vis – by 0.11 ± 0.03, field of view – by 65.1 ± 18.2°; in the control group: Vis – by 0.05 ± 0.01 and field of view – by 22.5–25, 1° in 47.1% of observations). However, it is difficult to judge the effectiveness of this method, since there are no long-term results of monitoring patients in this group.
Yu.K. Kiiko et al. [19], Yu.I. Kiiko and T.Yu. Amaryan [20] used cervical vagosympathetic blockade according to A.V. in clinical practice. Vishnevsky. It has been shown that this method has a positive effect on visual functions in patients with impaired blood circulation in the optic nerve and its sclerotic atrophy. Nevertheless, it would be inappropriate to speak unequivocally about the advantage of the method in chronic optic neuropathy, since the effectiveness of the method was assessed in a mixed group of patients.
In case of sclerotic atrophy of the optic nerve, electrophoresis with ganglerone on the upper cervical sympathetic nodes was used as an alternative method [19]. A short-term positive therapeutic effect was noted. The authors also proved that phlebodestruction operations are ineffective and cannot be performed in cases of pathology of the internal carotid artery.
E.I. Sidorenko [21–23] observed an improvement in visual functions in 76.2% of patients when using carbogen in the complex treatment of acute and chronic optic neuropathy. Carbogen therapy eliminates metabolic acidosis and is considered a good auxiliary method in the complex treatment of chronic vascular neuropathy.
In addition to trophic therapy, light therapy [24], ultrasound therapy [25], phonophoresis with tauphone [26], amplipulse electrophoresis [27], and acupuncture [28, 29] are successfully used for atrophy of the optic nerve. However, these methods also do not provide an effective and long-term therapeutic effect.
O.I. Karushin [30] noted an improvement in visual functions in 64.1% of patients during complex treatment of optic nerve atrophy, which included optic revascularization surgery, transcutaneous electrical stimulation of the optic nerve, and psychophysiological methods of vision correction. In addition, transcutaneous electrical stimulation of the ON has been used as a separate method for the treatment of ON atrophy. However, improvement in visual function was recorded in only 30% of patients [31].
N.F. Korosteleva et al. [32] performed an operation to intersect the SVA for dystrophic retinal pathologies of various origins, amblyopia, ischemic, glaucomatous and traumatic optic nerve atrophy. The result was a positive effect. At the same time, according to A.I. Eremenko et al. [33], transection of the SVA did not lead to an increase in visual function in any of 140 patients with vascular optic neuropathy. In addition, G.A. Shilkin et al. [34, 35] found that improvement in blood circulation in the choroid in 76% of patients after transection of the SVA is not always accompanied by improvement in hemodynamics in the ophthalmic artery (confirmed by Doppler ultrasound), which, in our opinion, may be a consequence of concomitant drug therapy.
The use of novocaine blockade of the sinocarotid zone (SCZ), as well as novocaine blockade of PVA, leads to improved blood circulation in the brain and eye. However, SCZ blockade should not be used in cases of severe cardiac changes with decompensation of general hemodynamics [36].
A number of publications have reported that carotid endarterectomy (CE) is most effective compared with conservative treatment in patients with clinically significant carotid artery occlusion and concomitant ocular ischemic syndrome (OIS). CE was accompanied by a statistically and clinically significant improvement in the condition of the visual organ. This conclusion was made by A.V. Gavrilenko et al., who compared the effectiveness of surgical (CE) and conservative treatment in patients with atherosclerotic occlusion of the carotid arteries and acute visual impairment (acute type of GIS).
The results of this study demonstrated functional improvement of the visual organ after surgery in patients with carotid artery occlusion and acute visual impairment [37].
In another study, the authors compared the effectiveness of surgical (CE) and conservative treatment of patients with atherosclerotic occlusion of the carotid arteries and chronic visual impairment (primary chronic type of GIS). The study recorded a decrease in ophthalmological and neurological symptoms after CE, which was reflected in a statistically significant decrease in symptomatic patients [38]. After performing CE, there was also a cessation of attacks of transient monocular blindness (amaurosis fugax).
A.V. Gavrilenko et al. analyzed the results of treatment of patients with transient monocular blindness (amaurosis fugax) due to carotid artery occlusion. A significant improvement in the condition of the organ of vision against the background of occlusion of the carotid arteries after CE was shown [39].
Reconstructive surgery on the carotid arteries in patients with pathological tortuosity of the carotid arteries is characterized by high efficiency. After the operation, improvement in visual acuity, expansion of the boundaries of the visual fields, disappearance of scotomas and stopping the processes of macular degeneration are observed [40].
In a recent study, Y. Yang et al. [41] evaluated the clinical effect of enhanced external counterpulsation (EECP) in combination with drugs in patients with carotid artery stenosis and concomitant ischemic ocular damage. In patients receiving EECP in combination with drugs, in contrast to patients taking drugs only, visual acuity significantly increased, visual fields and optical hemodynamics improved. This suggests that EECP can reduce symptoms and improve vision.
Many ophthalmologists pay special attention to improving old and developing new methods of surgical treatment of ischemic processes in the eye. The use of a number of techniques in the complex treatment of ischemia and its consequences can improve the hemodynamics of the eye and preserve visual functions.
Thus, an analysis of the literature data concerning the treatment of chronic ischemic diseases of the optic nerve shows that there are a number of issues in this area that require further study.
The search and analytical work was carried out at the personal expense of the team of authors.
The authors declare no conflict of interest.
Prognosis and prevention
Despite timely and correctly prescribed treatment, the prognosis is most often unfavorable. Often there remains a strong decrease in visual function and persistent defects in the periphery of vision caused by atrophy of the optic nerves. An increase in visual acuity of only 0.1-0.2 can be achieved only in 50% of cases. If both eyes are affected at once, there is a high probability of developing low vision or complete blindness.
Prevention of ischemic optic neuropathy is important and involves the treatment of vascular and systemic diseases. A patient who has suffered ischemic optic neuropathy in only one eye urgently needs follow-up with an ophthalmologist with appropriate preventive therapy.
Anterior ischemic optic neuropathy
Doctors distinguish several types of eye neuropathy. The most common is the ischemic form of this pathology. This condition develops due to damage to the optic nerve, which is a consequence of impaired blood supply. The nerve bundles in the eye area are compressed, which leads to a deficiency of nutritional components. This form of pathology is considered secondary. Usually its development is associated with cardiovascular diseases. Optic neuropathy is often caused by disturbances in the functioning of the endocrine and central nervous systems. Doctors call deterioration of hemodynamics in the area of the eyeballs “anterior neuropathy.” Blood flow disturbance occurs in the anterior segment of the optic nerve.
There are two types of pathology. They differ depending on whether a person suffers from arteritis - inflammation of the arterial walls - or not. Nonarteritic ocular neuropathy usually occurs suddenly. It develops against the background of diseases such as:
- sleep apnea;
- coagulopathy;
- diabetes;
- microscopic polyangiitis;
- microangiopathy;
- hypertension.
A person usually has vision loss in one eye. Only the top or bottom of the image is clearly visible. Damage to both eyes at the same time does not occur often - in approximately 15% of cases. But vision in the second eye may not deteriorate immediately. Sometimes this happens within 5-7 years. Pathologies are more common in people over 50 years of age. This disorder is extremely rare in children. Against the background of arteritis, this disease develops less frequently. Its symptoms are similar to those of non-arteritic neuropathy. People over 50 years of age who suffer from headaches, jaw muscle spasms, myalgia, alopecia, and loss of appetite are at risk for this pathology. Any changes in the shape of the optic nerve head are also the cause of the development of pathology.
Diagnostics
Since ION develops against the background of various diseases, consultation with an ophthalmologist, hematologist, neurologist, cardiologist, rheumatologist and endocrinologist will be required.
The following laboratory tests are carried out:
- measurement of erythrocyte sedimentation rate;
- C-reactive protein level;
- complete blood count and platelet count.
Together, these tests are highly predictive for biopsy-proven giant cell arteritis with a combined sensitivity of 97% for erythrocyte sedimentation rate and C-reactive protein levels.
To determine the disease, ophthalmoscopy is performed. If the patient does not have symptoms of giant cell arteritis, a magnetic resonance imaging (MRI) or computed tomography (CT) scan of the brain is done to make sure the optic nerve is not being compressed by the tumor.
Additional tests may be needed depending on the likely causes. For example, if someone has symptoms of obstructive sleep apnea (such as excessive sleepiness during the day or snoring), a polysomnography is performed. Patients who have had blood clots have their blood tested to diagnose clotting disorders.
Symptoms of glaucomatous neuropathy
As the disease progresses, the patient begins to experience the following symptoms:
- pain, stinging and sensation of a foreign body in the eyes;
- limited field of view;
- rapid eye fatigue;
- blurred vision at night;
- incorrect color perception;
- decreased pupil reaction to light;
- headache and dizziness;
- the appearance of rainbow stains before the eyes when looking at a bright light.
Glaucomatous optic neuropathy can be complicated by problems with heartbeat, attacks of nausea and vomiting, general weakness and chronic fatigue.