What is a cerebral aneurysm
An aneurysm, most commonly a saccular aneurysm, is a spherical or similar formation on an artery in the brain. An aneurysm, as I have already noted, can be saccular and fusiform. An aneurysm consists of three parts - the neck, body and bottom or apex.
Unlike a normal vascular wall, the apex of the aneurysm is not three-layered, but single-layered and is most vulnerable to rupture, especially since a shock flow of blood rushes into this place. Most often, the aneurysm is located in the anterior sections of the circle of Willis - in descending order - an aneurysm of the anterior communicating artery of the PSA, then an aneurysm of the internal carotid artery of the ICA, and an aneurysm of the middle cerebral artery. Less common are aneurysms of the vertebrobasilar region - aneurysms of the fork of the main artery of the OA, the mouth of the posterior inferior cerebellar artery of the PICA. Aneurysms of the pericallosal artery and other distal parts of the anterior cerebral and middle cerebral arteries are also quite rare.
How is endovascular surgery performed?
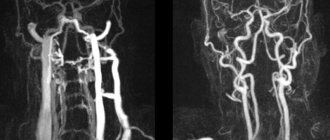
The intervention is performed by endovascular surgeons in a specially equipped X-ray operating room. The doctor needs to control the advancement of the catheter, his actions and the effect of the procedure; for this he uses fluoroscopy, angiography - an X-ray examination with the introduction of a radiopaque solution into the blood vessels.
Interventions are usually performed under local anesthesia. After anesthesia and treatment of the skin with antiseptic solutions, a small incision is made, access to the artery is gained and a catheter is inserted into it. When the tip of the catheter reaches the desired location, the necessary manipulations are performed. Then, as a rule, angiography is performed again for control. For example, after stenting, this helps to check whether the pathologically changed section of the artery has expanded and whether normal blood flow has been restored in it.
When the procedure is completed, the catheter is removed and a pressure bandage is applied to the puncture site to stop bleeding. Over the next few hours, the patient is prescribed bed rest, lying on his back.
Cerebral aneurysm photo
I present to your attention a photo of 2 aneurysms - the main artery and the bifurcation of the middle cerebral artery, which we encountered in our clinic over the past 2 weeks.
Saccular aneurysm of the bifurcation of the basilar artery
Saccular aneurysm of the bifurcation of the left middle cerebral artery. The aneurysm and branches of M2 are outlined with a ballpoint pen.
The aneurysm of the bifurcation of the basilar artery had to be transferred to another health facility for endovascular exclusion (filling with coils), and the MCA aneurysm was operated on in our clinic.
Treatment technologies at the Innovative Vascular Center
Vascular surgeons at our clinic have significant experience in open operations for abdominal aortic aneurysms. They have performed more than 150 operations for this pathology with success in 95% of patients. The approach of our clinic is to thoroughly prepare a patient with an aneurysm to exclude pathology of the heart and carotid arteries, which may affect the outcome of the operation. To prevent renal complications, we use prolonged hemofiltration in the postoperative period. To reduce blood loss, hemodilution (blood dilution) and blood return equipment are used. In order to prevent complications in the postoperative period, we practice early getting patients out of bed and active rehabilitation. In recent years, we have been gradually moving away from open operations for aneurysms in favor of less traumatic endovascular endoprosthetics operations.
Cerebral aneurysm causes of occurrence
The final genesis of the arterial aneurysm is not clear. Some argue that this is a congenital phenomenon - an undeveloped, blindly ending short vessel. Others say that this is an acquired condition - a protrusion in a weak spot of the hemangion - the structural unit of the vessel, between the circular areas of smooth muscle. As a result of the impact of the shock wave, this protrusion gradually grows. The formation of de-novo aneurysms confirms the presence of new aneurysms during control angiography in already operated patients. There is also an autoimmune inflammatory theory of the occurrence of arterial aneurysms, which is being actively developed at the University of Helsinki with the participation of Professor J. Hernisniemi. Thus, he believes that eventually a drug will be developed that can treat and prevent aneurysmal disease (he considers himself the last of the Mohicans - i.e. "aneurysmal" surgeons).
Cerebral aneurysm - symptoms
Most often, an aneurysm debuts with rupture - the most serious, often fatal complication. Hemorrhage can be subarachnoid, parenchymal and ventricular , and there are also all kinds of combinations of this trinity.
Among the atypical manifestations is pseudotumor ; with a gigantic size of the aneurysm, it can behave like a tumor and compress the brain and nerves, causing focal neurological symptoms.
A migraine-like course is manifested by hemicranialgia.
Pseudoradicular simulates radiculitis - pain in the legs, which is caused by blood flowing into the terminal cistern of the spinal cord.
Meningitis-like - in this case, patients with suspected bacterial meningitis can be admitted to an infectious diseases hospital, where SAH and suspected aneurysm rupture are diagnosed only with a lumbar puncture.
Psychotic - the name speaks for itself.
Treatment methods for cerebral aneurysm
Surgical
Aneurysm can only be treated surgically - by direct intervention, disconnection by clipping, wrapping with various materials (rarely) or by the endovascular method. Only milliary aneurysms can be observed in patients without risk factors for rupture. Aneurysms without previous hemorrhages are also subject to surgical treatment. It is easier to prevent a rupture than to treat its fatal consequences - vasospasm and clipping the aneurysm in the acute period.
Intraoperative photo of a clipped left middle cerebral artery aneurysm.
CT angiography the next day after surgery. Aneurysm is turned off. The M2 segments of the left MCA are contrasted.
The red circle marks the intervention area where 2 clips are installed. There are signs of vasospasm.
In the area of surgery on a native CT scan of the brain along the Sylvian fissure there is a small amount of blood - impregnated surgicell.
On a CT scan in bone mode, the clip is clearly visible.
Carotid endarterectomy
What is arterial stenting?
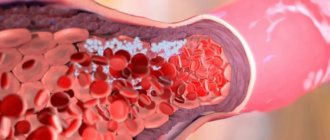
Atherosclerosis is a systemic process that affects the blood vessels of the entire body.
Cholesterol plaques form under the intima of the arteries, become more voluminous over time and narrow the vascular lumen. The basis of this disease is a violation of the patency of the vessels supplying blood to the brain (carotid and vertebral arteries). Most often, the patency of arteries suffers as a result of the development of atherosclerotic plaques on their walls, narrowing the lumen. As a result, the brain receives less blood, and the first symptoms of the disease appear. Significant narrowing of the lumen of the arteries, under certain conditions, can cause a stroke.
At the site of maximum narrowing of the artery, a stent is installed - a special wire frame of a cylindrical shape and a cellular structure. With its help, the vessel is no longer blocked, and cerebral blood flow is normalized.
Stenting of the carotid (carotid) arteries is an operation that restores the patency of the arterial bed and helps prevent the development of ischemic stroke. This is a modern and effective method of surgical treatment of carotid artery stenosis caused by atherosclerotic lesions.
Carotid artery stenting is the most advanced and least traumatic method of treating carotid artery stenosis in the world.
Its advantage is that it is less traumatic, since it does not require incisions on the skin, as in open operations, but only a small (about 2 mm) puncture at the site of catheter insertion.
Methods of surgical treatment:
- Open endarterectomy performed by vascular surgeons;
- Stenting of the carotid arteries is a modern, minimally invasive, x-ray surgical operation;
Preparing for surgery
Before surgery, it is necessary to perform such diagnostic research methods as:
- duplex ultrasound scanning;
- spiral computed tomography with bolus contrast;
These methods make it possible to determine the location of the atherosclerotic plaque and the nature of blood flow in the artery.
Progress of the operation
The technique is as follows: under local anesthesia, a thin needle is used to puncture a vessel on the thigh through the skin and a special device is installed - an introducer. A special catheter (2 mm in diameter) is inserted into the vessel through the introducer. It is advanced along the vascular bed to the point of narrowing of the artery. A special trap is installed to prevent small atherosclerotic plaques from entering the lumen of the arteries supplying the brain. Balloon angioplasty and stenting of the artery are then performed.
With balloon angioplasty, a special instrument with a balloon at the end is inserted into the artery. The balloon is brought to the site of narrowing and inflated. In this case: the atherosclerotic plaque is pressed into the walls of the artery, blood flow is restored, and the brain receives enough oxygen.
A stent is a metal frame installed at the site of narrowing using a special instrument. It strengthens the artery wall and prevents it from narrowing again. All manipulations are monitored using x-rays using special high-tech equipment - an angiograph.
Postoperative period
Immediately after surgery, the introducer site is pressed with a pressure bandage to prevent bleeding. After surgery, it is recommended to stay in bed for at least 12 hours so that the doctor can monitor the occurrence of complications. It is recommended to limit heavy lifting for a while. It is not recommended to take baths. After carotid stenting surgery, it is necessary to take blood thinning medications (aspirin, clopidogrel). In addition, it is periodically necessary to monitor the condition of the carotid arteries using duplex ultrasound scanning.
The effectiveness of the operation
- significant reduction in the likelihood of restenosis
- rapid recovery of the body
- good long-term results
Stenting of the carotid arteries is indicated:
- Patients whose blood vessel narrowing exceeds 60%
- Persons who are contraindicated for open surgery on the carotid artery - endarterectomy
- Patients with restenosis after endartectomy
- Patients with stroke symptoms
- In case of intolerance to general anesthesia
- After neck irradiation
- After neck surgery
Carotid artery stenting is contraindicated in persons:
- Persons suffering from hepatic-renal failure
- Those who are allergic to medications and contrast agents used during surgery
- Those who have had cerebral hemorrhages in the previous 2 months
- Those with total occlusion of the carotid artery by a thrombus, as well as unstable plaques of the aortic arch
- Those with contraindications to taking anticoagulants and antiplatelet agents
Preparing for surgery
The operation of stenting the carotid arteries is carried out according to strict indications.
The need for surgical intervention is determined by the vascular surgeon in each specific case. The specialist asks the patient about the medications he is taking; if you are allergic to contrast agents, metals or plastics. The patient is prohibited from eating and drinking the evening before stenting.
5-7 days before the operation he is prescribed to take drugs from the group of antiplatelet agents.
Cerebral aneurysm - consequences after surgery
The consequences of the operation, as well as the natural course of the disease, very often is cerebral vasospasm, which leads to unsatisfactory treatment results - death or severe neurological deficit in the form of paresis and paralysis, aphasia, mental disorders (which is typical for aneurysms of the anterior communicating artery). Meningitis may be a complication of the operation itself, which is associated with the presence of blood - a rich nutrient medium in the subarachnoid space, in the basal cisterns, cerebral ischemia, and a rather long operation time.
Thus, the treatment of arterial aneurysms is a very urgent and difficult problem in neurosurgery, especially in the acute and acute periods of hemorrhage.
Author of the article: neurosurgeon Anton Viktorovich Vorobiev Frame around the text
Why choose us:
- we will offer the most optimal treatment method;
- we have extensive experience in treating major neurosurgical diseases;
- We have polite and attentive staff;
- Get qualified advice on your problem.
Multiple aneurysms
To date, the proportion of patients with multiple aneurysms is 20–25% of all patients with aneurysms operated on at the institute. In the vast majority of cases, no more than two aneurysms are found in a patient with multiple aneurysms, but there are patients with three or more aneurysms. Combinations of aneurysms in localization, size, number, and clinical manifestations are quite diverse. The primary task at the diagnostic stage is to determine the aneurysm that served as the source of hemorrhage. The main principle of treatment for AF is the initial exclusion of a ruptured aneurysm from the bloodstream using microsurgical or endovascular techniques, depending on the anatomical features of the aneurysm. Operations can be performed in one or several stages. In the treatment of multiple aneurysms of various vascular territories, especially in the acute period of SAH, as well as in complex aneurysms, two-stage or multi-stage interventions are preferable.