Today, pudendal neuropathies (neuropathy of the pudendal nerve) are encountered quite often in the clinical practice of a urologist. They manifest themselves in the form of a syndrome with a general name - chronic pelvic pain.
Both women and men face this problem throughout their lives. So let's figure out what pudendal neuropathy is, why it occurs, how to diagnose it and how to treat it.
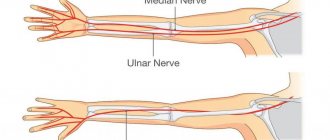
Let's start with the fact that complaints of pain in a sitting position, discomfort, numbness, burning in the pelvis can be explained by the anatomy of the pudendal nerve. This nerve leaves the spine at the level of 1-3 lumbar vertebrae and goes to the pelvis, passing between the muscles and ligaments. More precisely, between the piriformis muscle and the sacrospinous ligament. Note in Figure 1 where the pudendal nerve is labeled as. N.pudendus.
According to scientific research, most often the pudendal nerve is “pinched” either between two ligaments (sacrospinous and sacrotuberous), or between the piriformis muscle and the sacrospinous ligament. If this compression occurs, swelling will form around the nerve. This area begins to hurt, and the pain increases in a sitting position, actually due to the location of the area of nerve compression. After the nerve has passed these “dangerous zones”, it enters an equally dangerous canal - Alcock’s canal (the area of the ischial spine), however, based on literature data and our experience, compression in this canal occurs much less frequently.
Why is this happening?
There is evidence that risk factors for compression of the pudendal nerve are:
- Chronic microtraumas (non-systematic exercise according to the principle: “it’s better rarely, but wear it out.” This includes cycling, exercise in the gym, team sports).
- Hormonal disorders (diabetes mellitus, hypothyroidism, etc.)
- Systemic connective tissue diseases (collagenosis, etc.)
- Chronic intoxication (alcohol)
- Genetic predisposition
- Congenital anatomical features of the pelvis
Since there is no limit to indignation, or about neuropathy
In addition to neuralgia, the pudendal nerve can also become the scene of an inflammatory process, then they talk about neuropathy (neuropathy), or neuritis of the pudendal nerve (a term rarely used today).
Neuropathy differs from neuralgia in the presence of structural changes in the pudendal nerve, as well as movement disorders and the possibility of loss of sensitivity, which serves as a reason for indignation and upset of the patient, because we are talking about neither more nor less than the genitals.
What could be the reason?
The cause of the pathology (also called pudendoneuropathy) is the implementation of two mechanisms:
- compression-squeezing of the nerve trunk in the “scissors” of the sacrospinous ligament-piriformis muscle;
- traction due to overstretching of the nerve in the zone of its transfer over the ischial spine.
The first is illustrated by the consequences of long-term or unsuccessful horse riding or cycling (compression by a hard saddle), and the second by the consequences of surgical intervention - for example, when traction of the hip with the use of a perineal fixator, tension occurs on the nerve pressed to the pubic region.
Features of symptoms
The clinic may consist of lesions of the main nerve trunk or signs of involvement of various branches of the pudendal nerve.
When a surgical fixation is used in the perineal area, isolated damage to the dorsal nerve of the penis occurs with anesthesia of the penis and complete disruption of the previously normal erection.
Full restoration of sensitivity can occur within 6 to 18 months after surgery, but restoration of erection can be only partial.
When compressed by a hard saddle, the disorder is felt as transient numbness or the appearance of paresthesia in the genital area.
Both unilateral and bilateral loss of sensitivity may be observed, not limited to the penile area, but continuing to manifest itself also in the scrotum area.
Neuropathies of the pudendal nerve can signal themselves by pain in the lower buttock and in the anus, short-term urinary retention or a disorder of the imperatives to urinate, accompanied by sharp pain when palpated in the projection of the ischium.
In men, an inflamed pudendal nerve manifests itself with characteristic symptoms - paresthesia or hypoesthesia and pain in the peri-anal area, in the area of the penis and scrotum.
Diagnosis and treatment methods
The main diagnostic criterion is that the pull of the knee towards the opposite shoulder causes pain in the buttock (due to stretching of the sacrospinous ligament).
A simple diagnostic method is to pull the knee towards the shoulder
The clinic is confirmed by electromyography, noting the lengthening of the anal reflex, which closes on the pudendal nerve trunk, as well as a test blockade with the introduction of a novocaine solution into the area of the ischial spine.
The choice of treatment method depends on whether the process is advanced or in an acute stage.
Thus, all the symptoms disappeared in a group of cyclists on their own, after they agreed to refrain from cycling for a month. In case of chronic neuropathy, long-term restorative therapy is necessary.
In chronic cases, methods of drug therapy in combination with rational exercise therapy and physiotherapy are applicable.
Drug therapy includes the use of anti-inflammatory drugs (glucocorticoids Prednisolone, Triamcinolone, Hydrocortisone) in combination with anesthetics (Novocaine 0.5 or 1%) in the form of blockades. A case of relief of pain that had been observed for 14 years after a course of perineural administration of Triamcinolone is described.
Blockade is an effective method, the injection point is indicated with a finger
Pure novocaine blockades are usually less effective.
In order to relieve pain, suppositories of a combined formulation with anesthetics, sedatives and antispastic compounds, both rectal and vaginal, are used.
Vitamin therapy (administration of vitamin C and group B in adequate doses) is especially effective in combination with physiotherapy techniques (various methods of heat therapy), while exercise therapy allows you to increase the capabilities of muscles spasmed by pain and helps to increase the overall tone of the body.
Surgical intervention is applicable if there is no effect from treatment with therapeutic methods.
You should be extremely careful in the case of neuropathy of oncogenic etiology.
Diagnosis of pudendal nerve neuropathy
Today, there are clinical criteria that suggest pudendal neuropathy. We are talking about the Nantes criteria. Answer yourself the question whether you have these clinical symptoms.
- Pain in the area of innervation of the pudendal nerve: from the anus to the clitoris/head of the penis.
- The pain is felt worse when sitting.
- The pain does not cause awakenings at night.
- The pain is not accompanied by a decrease in tactile sensitivity.
Additional criteria:
- The pain is burning, shooting, stabbing, and may be accompanied by slight numbness.
- The pain worsens during the day and subsides after sleep.
- Mostly the pain appears on one side.
- Pain may be triggered by defecation.
If you notice that you have these symptoms, you should immediately consult a doctor.
Already at the initial appointment, the doctor will be able to conduct additional special manual tests.
Only a urologist specializing in the treatment of pelvic dysfunction should perform a manual examination (both in a gynecological chair and on a couch). This is due to the need to thoroughly and carefully examine the areas most susceptible to compression. An insufficiently complete examination is fraught with the loss of valuable diagnostic information, incorrect interpretation of symptoms and low effectiveness of treatment.
The next step is to conduct electrophysiological studies,
for example, assessing the bulbocavernosus reflex using electromyography.
All possible diagnostic methods are carried out at the Expert Urogynecology Clinic by highly qualified specialists in the field of pelvic floor pathology. Differential diagnosis is carried out with lesions of other pelvic nerves, as well as with myofascial syndrome. The latter is characterized by painful sensations when pressing on various trigger points in the muscles.
| anonymously to the doctor, through the feedback form, we will try to help you. | Ask a Question |
About the causes and symptoms of functional disorders
For the etiology of damage, the proximity to the ischium, which the nerve goes around entering the pelvic cavity, as well as the relatively shallow depth of the terminal branches under the surface of the skin and mucous membranes of the pelvic organs, are important. Therefore, dysfunction can occur as a result of:
- injuries to the perineal area;
Perineal trauma can lead to more serious consequences
Provoking factors may be:
- horse riding or cycling (frequently or professionally);
- prolonged labor;
- fracture of the pelvic bones (from a fall from a height, in a car or plane accident).
To understand that something is wrong with the genitofemoral nerve is made possible by dysfunctions of the organs located in the pelvis. These may be sensitivity disorders or autonomic disorders.
The first category includes both varying degrees of decrease in sensitivity (up to its complete loss) and an increase in pain to unbearable limits.
Deviations in autonomics are expressed by disturbances in the functioning of glands and other structures containing smooth muscle fibers, in particular, disorders of the mechanism of blood supply to the cavernous bodies of the penis or clitoris.
Trophic disorders of the skin of the perineum, scrotum and peri-anal area can also be a sign of disorders.
In addition to physical factors, the cause of pathology can also be general somatic diseases:
- tuberculosis;
- collagenoses;
- blood supply disorders due to endocrine disorders and vascular accidents or for any other reason.
Treatment of pudendal nerve neuropathies
Therapeutic and diagnostic blockades
Conservative treatment is aimed primarily at removing tension (decompression) of the nerve in “critical zones” and restoring normal trophism.
The first stage is recommended to carry out therapeutic and diagnostic blockades of these very problem areas, which we talked about at the very beginning (areas of ligaments and muscles).
The most common are blockades with local anesthetic (lidocaine, bupivacaine) and glucocorticoid (betamethasone).
Transvertebral magnetic neuromodulation
Within the walls of our center, a unique method of treating neuropathic pain has been developed and adapted. It is highly effective for true pudendal nerve neuropathy and is used in parallel with blockades. The deep impact of a directed magnetic pulse with a certain frequency on the area where the pudendal nerve exits the spine (level S2-S3) allows you to “reset” the innervation and break the vicious circle of pain. The course of treatment with magnetic neuromodulation ranges from 10 to 15 sessions, depending on the severity of the disease.
Botulinum therapy.
Indicated in the presence of muscular-tonic syndrome, when the muscle needs to be relaxed. Botulinum toxin type A is successfully used specifically to target this pathological component.
When used correctly (according to indications and with good navigation via ultrasound), the risks of complications are minimal.
Transcranial magnetic neuromodulation
The newest method of influencing brain structures.
In Russia, we are leaders in the use of neuromodulation of the central and peripheral nervous system for the treatment of pelvic floor dysfunction and chronic pelvic pain syndrome. This technique is aimed at eliminating central sensitization - a condition that develops during a long course of the disease, when the patient did not receive adequate treatment in time.
Remember, even with a prolonged course of the disease there is a way out!
Manual therapy.
The main goal of treatment by an osteopathic neurologist is to eliminate biomechanical disorders and pathological changes in soft tissue structures.
When a person has a sore muscle, he tries to reflexively “save” it by changing his position, sitting or walking. This leads to the fact that these structures, which bear an additional “volume of work,” begin to experience additional stress and get sick. And this only strengthens the vicious circle of disease development. With the help of manual techniques, it is possible to return to its place what has been displaced and is involved in the pathological process.
Pudendal nerve neuropathy: a patient’s history of recovery
Pudendal nerve: symptoms of neuropathy
As with any other pinching, symptoms include pain, sensory disturbances, muscle weakness and disorders of the autonomic system.
When the pudendal nerve is pinched, the symptoms in women and men are similar:
When the pudendal nerve is pinched, symptoms in women whose treatment should not be delayed are observed in the lower part of the vagina. This causes great discomfort.
Severe pain may be felt during sexual intercourse and walking - these are the symptoms in men if the pudendal nerve is pinched. Treatment is required immediately, as the pain becomes burning, and touching the skin becomes painfully unpleasant. The sensations can be described as the presence of a cold or hot foreign object or electric shock. In general, a pinched pudendal nerve entails a large number of unpleasant symptoms.
Diagnostics
If you have these symptoms, you should consult a neurologist. Identification of the disease begins with a thorough history taking. The presence of a triad in the system of complaints - pain, burning and sensory disturbances - makes it possible to make a preliminary diagnosis and determine the range of additional studies.
An ultrasound Doppler scan is required, which helps to identify a slowdown in the speed of blood flow in the pudendal artery. The presence of such a pathology indirectly indicates a possible pinching of the vessel, and therefore the nerve located along its course.
During the examination, the branches of the pudendal trunk are blocked. If it helps to completely relieve pain, the diagnosis is confirmed.
Long-term treatment
It must be remembered that treatment of neuropathy of the pudendal nerve is a very long process, during which all recommendations of the attending physician should be followed. The recovery period takes at least six months.
Treatment of the disease should be carried out only in a hospital setting, as this will allow doctors to take control of the healing process, as well as successfully select a set of means that will be used for proper treatment. After all, a person may be allergic to some medications, which will only worsen the situation.
Treatment of pudendal nerve neuropathy
As in other situations, treatment of this disease must be comprehensive.
What are the basic principles of treating neuropathy?
- Influencing the characteristic pain pattern of pinching with the help of gabapentin, which is part of the medicine.
- Regular nerve blocks using hormones and anesthetics.
- The use of centrally acting muscle relaxants, which allow the muscles to relax, resulting in a decrease in the tone of the piriformis muscle.
- The use of physiotherapeutic effects, which include electrophoresis and phonophoresis.
- Taking B vitamins, which are part of the blockade, as well as in tablet form.