What is cerebral edema
Physiologically, the maintenance of intracranial pressure is ensured by a constant volume of blood and cerebrospinal fluid. Changes in atmospheric pressure, compensation for different volumes of circulating blood are compensated by the inflow or outflow of cerebrospinal fluid. The appearance of additional formation inside the brain, hematoma, inflammatory processes, traumatic brain injury (TBI) leads to compression of cerebral structures. An increase in intracranial hypertension causes the death of parenchyma. Features of symptoms depend on the strength and location of the pathological focus.
Pathological cerebral edema leads to an increase in the size of brain tissue through excess accumulation of fluid. An increase in the amount of water is accompanied by death (if prompt decompression is not carried out in a timely manner). A gradual increase in the volume of brain tissue initially leads to neurological disorders. Psychoses and disturbances in the functioning of internal organs gradually develop.
Prevention
There is no specific prevention of cerebral edema, since it develops secondary. Among the general recommendations, we can only cite the need to follow some rules:
- Minimize the risk of head injury: use protective devices when moving (protective helmet when rollerblading/biking/skating, skiing; seat belts when driving in a car, do not jump your head into a body of water, etc.).
- Treat infectious/somatic diseases in a timely manner.
- Monitor your blood pressure .
- Lead a healthy lifestyle.
- When climbing to altitude (mountains), do not forget about the need to acclimatize to the altitude.
Classification of cerebral edema according to ICD 10
Clinical gradation of cerebral edema according to pathogenesis:
- Filtration;
- Interstitial;
- Cytotoxic;
- Vasogenic.
Depending on the location of fluid accumulation, symptoms are distinguished. Vasogenic lesions lead to disruption of the heart, vision pathology, and kidneys. Any organs that have an intensive blood supply are damaged.
The interstitial variety is characterized by compression of most structures of the central nervous system. The intervening fluid initially does not lead to tissue death, since it occupies free space. Lack of nutrients and oxygen leads to cell death. The speed of onset of the effect is determined by the degree of compression.
Classification of intracerebral edema by etiological factors:
- Postoperative;
- Traumatic;
- Malignant (tumor);
- Hypertensive;
- Ischemic;
- Inflammatory;
- Intoxicating.
Standardization of the disease according to ICD 10 allows you to correctly determine the nosological form:
- Nervous diseases – “G0-99”;
- Other nervous system disorders – “G90-99”;
- Various brain injuries – “G93”;
- Cerebral edema – “G93.6”;
- Unclassified cerebral edema – “R60”;
- Localized – “R60.0”;
- Generalized – “R60.1”;
- Unspecified - "R60.9".
Perifocal vasogenic appearance occurs due to increased permeability of the vascular wall. The penetration of blood through the wall leads to the destruction of the blood-brain barrier. The perifocal form occurs at the site of surgery, around the tumor, near the inflammatory focus.
The intoxicating cytotoxic variant develops mainly in the white matter during poisoning with carbon monoxide, cyanides, ischemic conditions, and viral infections. Viral infections provoke cytotoxic changes gradually, leading to the destruction of neurons.
The osmotic variety is formed when the osmolarity of tissues changes. Destruction of the blood-brain barrier is formed during hypoxia during childbirth, sweating through the destroyed walls of the cerebrospinal fluid. The condition is provoked by metabolic encephalopathies (for example, in diabetes mellitus).
Pathogenesis
Brain swelling is a stepwise process in which acute injury results in the formation of cytotoxic, ionic, or vasogenic edema. What is edema? This is a combination of pathogenetic mechanisms. Cytotoxic edema is characterized by depletion of intracellular adenosine triphosphate (ATP), which impairs the active transport of osmolytes across cell membranes. Sodium and water ions accumulate in cells.
On the surface of cell membranes, the pressure and ratio of ions are disrupted, which leads to the movement of fluid into the extracellular space of the brain parenchyma from the vessels. This mechanism is also called ionic. During brain contusions, the activity of the Sur1-Trpm4 ion channel in endothelial cells increases, which leads to fluid accumulation.
A separate form of cytotoxic edema is vasogenic. The pathology develops due to increased permeability of the blood-brain barrier of the brain after a bruise, the release of inflammatory substances during infection and an increase in free radicals. As a result, fluid is released outside the cell along with blood plasma proteins.
As brain contusion develops, these mechanisms replace and complement each other, leading to swelling. It is believed that edema is preceded by an increase in intracranial pressure due to the fixed volume of the closed cranial cavity. At the same time, capillary perfusion - blood pressure in the vessels of the brain - decreases. The tissues do not receive enough nutrients and oxygen, and hypoxemia develops.
Causes of cerebral edema
If a person’s brain swells, the etiology of the disease is first established. Main causes of the disease:
- Hemorrhage inside the skull during hypertensive crisis;
- Traumatic brain injury after a fall, traffic accident, blow from above;
- Malformations of the central nervous system in newborns;
- Inflammatory diseases - toxoplasmosis, meningitis, encephalitis, purulent limited destructive cavities (abscess);
- Change in atmospheric pressure (stay above sea level over one and a half kilometers);
- Carbon monoxide poisoning;
- Birth injury;
- Ischemic or hemorrhagic stroke.
Other etiological factors are less common, but are characterized by similar pathogenetic mechanisms.
Features of cerebral edema in newborns
The structure of the brain of a newborn and infant differs from the structure of the skull of an adult. The baby has instability of anatomical structures. Mechanisms for compensating for increased intracranial pressure have not been developed; there is no redistribution of cerebrospinal fluid and blood to level out hypertension. An increase in fluid inside the skull in an infant is accompanied by acute symptoms. An increase in intracranial hypertension leads to bulging of the cartilaginous tissue of the fontanelles and soft bones.
Immediately after birth, it is necessary to exclude risk factors in children to prevent nosology. Diseases can be identified after the first signs appear:
- Muscle cramps;
- Drowsiness and inhibition of brain activity;
- Restless behavior;
- Bulging of the fontanelle when the child is resting;
- Difficulty feeding from the breast;
- Frequent gag reflex.
Early detection is necessary, since late verification of cerebral edema in a child often ends in death.
Features of intracerebral edema in alcoholism
Metabolites of ethyl alcohol lead to the destruction of the vascular wall, increasing the permeability of the wall. Alcohol abuse in adults provokes chronic vasogenic edema. The condition leads to psychosis (delirium tremens, withdrawal symptoms). The longer the abuse of ethyl alcohol, the more irreversible the changes inside the brain.
Varieties, reasons
Brain edema occurs:
- vasogenic;
- cytotoxic;
- interstitial;
- osmotic.
The signs of cerebral edema depend on the type of developing pathology.
Causes of disease progression:
- Vasogenic edema occurs due to increased cerebral vascular permeability.
- Cytotoxic is the “swelling” of brain cells due to an increase in the amount of fluid inside them.
- Interstitial edema develops when there is increased pressure of the cerebrospinal fluid in the ventricles of the brain.
- Osmotic edema - with an increase in the osmolarity of brain tissue.
The most common reasons that cause brain swelling are: brain injury and disruption of its tissues in various pathologies.
Brain edema most often occurs in the following pathological conditions of a traumatic nature:
- brain contusion;
- fracture of the base of the skull;
- intracerebral hematoma;
- subdural hematoma. The prognosis of surgery for cerebral edema depends on its size.
The described pathology develops against the background of such organic brain lesions:
- ischemic and hemorrhagic stroke;
- hemorrhage under the arachnoid membrane;
- tumors;
- infectious diseases - encephalitis (inflammation of brain tissue) and meningitis (inflammation of the meninges).
Extracranial causes of cerebral edema can result from:
- Quincke's edema is a severe allergic reaction of the body;
- infectious diseases - scarlet fever, measles, mumps;
- diabetes;
- liver failure;
- alcoholism.
On our website Dobrobut.com you will find more information about the causes of cerebral edema in a newborn child, the development of pathology in the elderly and other facts.
Pathogenesis of cerebral edema
The initial stage of the pathology is accompanied by impaired microcirculation. Perifocal changes are located near the tumor, inflammatory focus, at the site of bone-destructive injuries to the skull.
A consistent increase in changes, the accumulation of copious amounts of fluid is accompanied by a disorder of vascular regulation, an increase in the size of the cerebral arteries, and subsequent intracranial hypertension.
Swelling of brain tissue, generalized swelling is characterized by circulatory and vascular edema. Multiple injuries cause massive death of neurons. The fluid squeezes out intracerebral structures, and the disposition of anatomical formations is formed. The situation increases the risk of death due to the likelihood of the brain being wedged into the foramen magnum. Death occurs due to damage to the center of thermoregulation, respiration, and cardiovascular activity.
Vascular dementia - symptoms and treatment
According to the International Classification of Diseases, 10th revision (ICD-10), there are the following types of vascular dementia:
- Acutely developed dementia. When a heart attack or hemorrhage is localized in a functionally significant area.
- Multi-infarct dementia.
- Subcortical dementia. The most characteristic of subcortical arteriosclerotic encephalopathy is Binswanger's disease (progressive damage to the white matter of the brain).
- Mixed subcortical-cortical dementia.
- Other forms of dementia, including dementia with hemorrhage, with global ischemia resulting from severe hypotension or cardiac arrest.
- Vascular dementia, unspecified [6].
Stages of development of vascular dementia:
Stage 1. There are no cognitive impairments. There is no apparent memory deficit on clinical interview, but very mild cognitive impairment develops.
Stage 2. Subjective complaints of memory loss arise, most often expressed as follows:
- Patients forget where they leave familiar objects.
- They forget the names of acquaintances whom they knew well in the past. However, there is no evidence of memory deficit at the clinical interview. There are no objective violations of social and professional adaptation. Criticism of one's condition is preserved.
3. stage. It is possible to see obvious cognitive impairment. Manifestations are observed in more than one of the following areas:
- The patient may get lost when traveling to an unfamiliar place.
- the patient may read a passage or book and remember nothing of what he read.
- The patient may show decreased ability to remember names after meeting new people.
- The patient may have lost or is losing motivation to perform activities.
- Concentration deficits will be noticeable on clinical testing. Objective evidence of memory deficits can only be obtained through intensive interviews. Decreased productivity at work and in social settings. Criticism of one’s condition begins to decline.
Stage 4. Accompanied by symptoms of mild cognitive decline (mild dementia): clear deficits on a thorough clinical interview that are evident in the following areas:
- Decreased knowledge of current and recent events.
- Deterioration of memory of one's past.
- Lack of concentration that occurs when reading text sequentially.
- Decreased ability to travel, manage finances, etc.
At the same time, there may not be a shortage in the following areas:
- Orientation in time and place.
- Recognizing familiar faces.
- Opportunity to travel to familiar places.
Patients at this stage are unable to perform complex tasks. Lack of criticism of one's condition is the dominant psychological defense mechanism for patients with vascular dementia.
Stage 5. Moderately severe cognitive impairment (moderate dementia): the patient already needs help for everyday life. The patient is unable, during a clinical interview, to recall any important aspect of his current life, such as an address or telephone number that he has known for many years, the names of close family members (for example, grandchildren), or the name of the school or college from which he graduated. There is often some disturbance in time orientation (date, day of the week, season, etc.).
An educated person may have difficulties with the “Counting according to Kraepelin” test (it is proposed to subtract 7 from 100 in sequence). But patients at this stage still retain knowledge of many important facts about themselves and others. They always know their names and, as a rule, the names of their spouses and children. They do not need assistance with grooming or nutrition, but may have some difficulty choosing appropriate clothing.
Stage 6. Severe cognitive decline (moderately severe dementia): Sometimes a patient at this stage may forget the name of the spouse on whom he is completely dependent as a caregiver. Patients, as a rule, do not remember many recent events and experiences in their lives. They retain some knowledge about their past life, but it is very superficial. Typically, patients do not know their exact location, year, season, etc. There may be difficulties in counting prime numbers up to 10 and back. Some assistance is required with activities of daily living. The daily rhythm is often disrupted. Patients almost always remember their name. They are often still able to differentiate between familiar and unfamiliar people in their environment.
Personal and emotional changes occur. These changes are quite varied and include:
- Psychotic symptoms. For example, patients may complain about a spouse who is allegedly an impostor, talk to imaginary figures, or refer to their own reflection in the mirror.
- Obsessive, repetitive actions.
- Symptoms of anxiety, agitation, and even previously unusual aggressive behavior may occur.
- Decreased volitional sphere. A person cannot think long enough to make a purposeful decision to take an action.
Stage 7. Very severe cognitive decline (severe dementia): all verbal abilities are lost. Often there is no speech at all, only incomprehensible statements and the rare appearance of seemingly forgotten words and phrases (incoherent thinking). Patients require assistance with personal care and feeding. Basic psychomotor skills, such as the ability to walk, are lost as this stage progresses. The brain can no longer tell the body what to do. An increase in muscle tone is often present and pathological neurological reflexes develop, for example the Babinski reflex (pathological extension of the big toe when the edge of the sole is irritated)[10].
The first signs of cerebral edema
Symptoms are determined by general and local disorders. It is impossible to determine what is primary, therefore an analysis of the initial signs of pathology is required:
- Severe pain or increasing chronic pain in the head;
- Cloudiness of consciousness;
- Fainting;
- Meningeal syndromes are disorders of conscious activity;
- Paresis and paralysis of half the body;
- Visual pathology;
- Coordination disorders;
- Reduced blood pressure;
- Constant muscle contractions (convulsive);
- Strabismus.
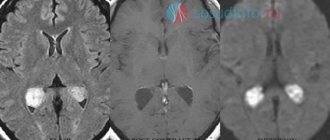
Mortality due to intracerebral edema is often observed, so it is important to identify at least one sign to prescribe additional diagnostic methods - neuroimaging (MRI and SCT of the head).
How do I know if I have scalp swelling?
A healthy scalp is normally moderately elastic. This means that the skin on it should move freely when pulled in different directions, without pain or difficulty in this process.
Check the condition of your scalp yourself. Place your finger on the temple area and pull up to the top of the head. If you feel as if the skin doesn't want to move, there's very little tension, or it's painful, it could be swelling. Repeat the same movement on the top of your head.
Do this check periodically, because it is much better to prevent pathology than to treat the consequences.
Consequences of cerebral edema
Dangerous complications of pathology are determined by a number of pathogenetic changes:
- An increase in the amount of fluid with an increase in the degree of compression of the cerebral parenchyma, the disposition of brain tissue. Mortality occurs when available space for water storage runs out;
- Early detection, drug elimination of the pathology with subsequent resorption of free fluid is a favorable prognosis. Timely delivery of people to the intensive care unit or toxicology department allows to remove toxins and eliminate other etiological factors;
- Removal of edema after disability occurs. Meningitis, meningoencephalitis due to traumatic brain injury lead to irreversible neurological disorders.
Even after timely surgery, complete relief from the consequences of the disease cannot be guaranteed.
Neurogenic consequences of cerebral edema:
- Memory disorders;
- Strabismus divergent;
- Severe headaches;
- Motor disorders;
- Depressive state;
- Epileptic seizures;
- Pathology of speech and attention;
- Facial asymmetry.
The consequence of the condition can be constant anxiety and chronic fatigue.
Symptoms
Brain edema: symptoms - bursting headache, which is detected almost equally in the occipital, parietal, temporal and frontal parts. Vomiting or nausea also occurs, which does not improve. Vision decreases, the person becomes weak and drowsy. Some are plagued by convulsive seizures - involuntary contractions of the muscles of the arms and legs, sometimes accompanied by loss of consciousness or biting the tongue. A disturbance of consciousness occurs or it completely disappears, then the person does not answer questions immediately or ignores them. Signs of cerebral edema can also be observed in breathing problems due to compression of the chest.