It is known that a person receives up to 85% of information about the environment through vision, and only the remaining 15% is hearing and other senses. The occipital lobe is the area responsible for the highest processing of visual signals. Thanks to it, healthy humanity is able not only to distinguish surrounding environmental objects by their visual characteristics, but also to contemplate the creations of artists, to create themselves. We can catch the mood of other people by observing the changes in their facial expressions, enjoy the beauty of the sunset, and, finally, choose food based on our favorite color.
- Location
- Functions
- What fields are included?
- Symptoms of the lesion
Interesting facts about the spinal cord and white matter
The white matter of the spinal cord contains a lot of interesting things and is the best conductor of nerve impulses, but the bone marrow itself is a very interesting structure that hides quite a large number of mysteries.
Here are the most interesting facts that scientists told the world about this system of the human body:
- The human spinal cord actively grows and develops from infancy to five years, after which it reaches a size of 45 centimeters.
- The older a person is, the more white matter is contained in the spinal cord, because it replaces dead nerve cells.
- The human spinal cord underwent evolutionary changes much earlier than the brain.
- The nerve centers responsible for sexual arousal are located exclusively in the spinal cord.
- Music is very beneficial for the spinal cord.
The most interesting thing is that the white matter of the spinal cord has a beige tint, and the name says something completely different. This component of the brain and spinal cord has approximately the same functions and undergoes the same morphological changes over the course of a person’s life.
- Location
- Assigned functions
- METHODS FOR STUDYING THE FUNCTIONS OF THE CEREBRAL CORTEX
- Assigned functions
- Dorsal and lateral routes
- Pathologies of the cerebral hemispheres
- Types and functions
The white matter contained in the bone marrow of animals has a completely different shape than in humans, and it also differs in different species of fauna. Scientists still have not figured out why everything turned out this way, but they can say with confidence that this structure is reliably protected from external influences by bone tissue.
The spinal cord, containing white and gray matter, is responsible for the sensuality of the entire body. If some of its parts are damaged, a person has to face various physical problems - loss of motor activity, speech, sensitivity, hair. This mechanism consists of many nerve endings, more than half of which are lost after the baby is born, and the rest can be destroyed due to the person’s lifestyle.
In the brain and spinal cord, white matter is located in certain areas, thanks to which it can transmit impulses to the central nervous system quickly and correctly. Even if you watch a person’s brain activity all day long, it is impossible to say exactly what the white matter does, because everything happens so quickly that the human eye cannot catch it.
The spinal cord, like the brain, contains white and gray matter and they are closely connected. Their work can be compared to the working mechanism of a Swiss watch and it will always be justified. The scientific facts about these structures are simply amazing. White matter consists of millions of small components that intertwine with each other, connecting into a complete, complex, functional structure. All this happens even before a person is born, and is consolidated in infancy. This structure is closely connected with the human nervous system, and if problems arise in this direction, then physical health will suffer. To prevent this from happening, a person needs to protect his back and nerves from the adverse effects of the outside world, and then he will be able to live a happy, long, healthy life.
The gray matter of the spinal cord and its white matter cannot exist separately and therefore a person must always monitor the condition of his body so that no malfunctions occur. If the diencephalon, medulla oblongata, or midbrain and white matter lose communication, the body will be at serious risk, and no one wants that.
Structure and functions of the hindbrain
The metencephalon (posterior part) develops at the stage of embryonic ontogenesis, originating from the anterior part of the rhomboid region. During development, the structure of the hindbrain is supplemented and gives rise to the pons and cerebellum. Thus, the rhomboid section becomes the myelencephalon (secondary medullary vesicle) from which the medulla oblongata of the CNS organ originates.
The anatomy of this structure is quite well studied and in evolutionary development it belongs to the most ancient area. The physiology of the hindbrain was studied using the ablative method (removing part of the organ and then observing changes in the body), which helped to deeply study the functioning.
Having studied the back of the brain in section, scientists were able to describe which cavity communicates it with the medulla oblongata of the central nervous system - the fourth ventricle. The cranial nerves pass through it; the medullary striae serve as the border.
The posterior (diamond-shaped) section of the central nervous system consists of:
- Oblong section;
- The hindbrain itself.
The second structure, in turn, is divided into the pons and the cerebellum. The rhomboid part of the central nervous system is involved in reflex activity, since it contains nerve bundles and cranial nerves that perform various functions.
Hindbrain - structure and functions of reflex activity:
- Gaulle's bundle - represented by axons, regulates muscle and joint sensitivity (from the lower extremities);
- Burdach's bundle - includes axons, regulates muscle and joint sensitivity of the entire upper body (from the neck).
These bundles form the path of proprioceptive sensitivity and allow you to recognize the position of body parts in space, perceive postures and feel both active and passive movements. If there are disturbances in the cortical direction, the coordination of movements is lost and they become disproportionate.
Reflex activity is also carried out with the help of innervation by cranial nerves (nuclei from 5 to 12 pairs), which form the classification of various reflexes in the corresponding structures of the central nervous system.
The hindbrain is involved in the implementation of the following reflexes:
- Responsible for tactile sensitivity - the function is provided by the trigeminal nerve (5th pair), located between the pons and the middle cerebellar peduncle. Supports unconscious reflexes in response to pain or touching a hot object. At the exit from the bridge it connects with the mandibular nerve and innervates the muscles of mastication. Damage to the fibers is accompanied by sharp pain and hyperemia of the skin on the face. If disturbances affect the motor nuclei, then atony of the masticatory and temporal muscles occurs.
- Responsible for the work of the oculomotor muscle (rectus) - the function is supported by the abducens nerve (6th pair), lies in the thickness of the bridge, exiting in the oblong part of the central nervous system and penetrates into the orbital area. Damage to the fibers leads to blurred vision (double vision) and the inability to direct gaze in any direction.
- Provides facial expressions - innervation of the facial nerve (7th pair). The roots extend from the bridge tire. After which a loop is formed and then the fibers run through the thickness of the bridge, exiting through the gap between the oblong structure of the central nervous system organ. Damage to the fiber (its branches) leads to a complete absence of facial expressions, the face becomes like a mask (all folds are smoothed out, blinking movements are impossible, eyelids do not droop).
- Responsible for hearing and vestibular regulation - the vestibular nerve (8th pair), is divided into two parts. The first (cochlea) conducts auditory impulses to the central nervous system, the second (vestibular) is located at the bottom of the auditory canal and regulates balance. From the first part, the nerve fibers end in the tegmentum of the bridge, from the second, in the cavity of the diamond-shaped structure - the diamond-shaped fossa. Damage to the nuclei leads to hearing loss and impaired balance (staggering gait).
- Responsible for swallowing movements - muscle contraction is provided by the glossopharyngeal nerve (9th pair), and in addition to the pharynx, it innervates the middle ear and tongue (posterior third). It comes out of the hole in the skull and runs to the cavity of the rhomboid region (4th ventricle). Damage to the fibers causes difficulty swallowing (or pain) and impaired taste sensitivity of the tongue.
- Responsible for the functioning of organs in the abdominal and thoracic cavities - the function is provided by the vagus nerve (10 pair), starting from the oblong part of the central nervous system organ, extending down through the neck to the cavities. Damage to the nuclei causes a malfunction of the internal organs, and paresis of the pharynx or larynx is possible.
- Controls contractions of the trapezius and large superficial muscles of the neck - the innervation comes from the accessory nerve (11th pair), the upper part of the fibers starts from the oblong structure, the lower part - from the anterior horns of the spinal part of the central nervous system (upper segments). At the exit from the cranium it intertwines with the vagus nerve. Damage to these fibers causes paresis or paralysis of the innervated muscles.
- Responsible for movements of the tongue - innervation is provided by the hypoglossal nerve (12 pair), located in the rhomboid fossa and has multiple branches, the final branch ends in the tongue. Damage to the fibers leads to impaired motor abilities in the tongue (muscle atrophy).
All parts of the diamond-shaped structure are connected to each other through neural connections that act as conductors.
Location
The temporal lobe is part of the telencephalon and is included in the structure of the cortex. It is located on both hemispheres of the brain on the sides below, in close contact with neighboring areas - the frontal and parietal lobes. This area of the cortex has the most pronounced boundary lines. The upper part of the temple is slightly convex, and the lower part is concave. The temporal lobe is separated from all the others by a groove called the lateral (lateral). The close location of the temporal and frontal lobes is not accidental: speech develops in parallel with thinking (frontal cortex), and these two functions are closely interconnected, since the ability to formulate and express oneself clearly (speech) is ensured by the degree of development of mental functions.
The convolutions of the temporal lobe are located parallel to the grooves that limit the area. Anatomically, there are 3 gyri: superior, middle and inferior. However, the superior cerebral fold includes 3 more small convolutions located in the sulcus itself. This group of small structures is called Heschl's convolutions. The inferior gyrus of the temple borders the transverse medullary fissure. On the lower part of the temporal lobe, in addition to the inferior gyrus, additional structures are also distinguished: the hippocampal peduncles, the lateral occipitotemporal gyrus.
Assigned functions
The functionality of the temporal cortex is insignificant, however, it is highly specialized. The functions of the temporal lobe of the brain are associated with the perception, analysis and synthesis of speech, the perception of auditory information, and partly gustatory and olfactory information. Also, the location of one part of the seahorse determines another function - memory, namely its mechanical component. One area has a special purpose: Wernicke's center (sensory speech area) - located on the back of the superior temporal gyrus. This zone is responsible for the perception and comprehension of oral and written speech.
What matters is the functional asymmetry of the brain, that is, the location of the dominant areas of the cortex on the surface of the brain. This specificity of the central nervous system did not bypass the temporal lobe.
Important Mydocalm: instructions for use, price and reviews
The left temporal lobe is responsible for the following functions (it should be noted that the list of tasks is based on the fact that the left hemisphere is dominant):
- Understanding audio information (music, words and speech);
- Short-term memory;
- Choice of words during a conversation;
- Synthesis of visual information with auditory information;
There is an interesting phenomenon here - synesthesia. Only 0.05% of the population has this phenomenon. The essence of the phenomenon is the ability to see the qualitative parameters of sounds in a different color spectrum. Physiologically, this is explained by the process of irradiation (spread of action potential), when the excitation of an overly irritated area of the cortex passes to the neighboring part of the brain. As a rule, famous musicians (Rimsky-Korsakov, Franz Liszt) possessed and still possess this ability. - The connection between music and emotions;
The right temporal lobe of the brain is responsible for the following functions and abilities:
- Recognition of facial expressions;
- Identification of speech intonation;
- Musical tones and rhythm;
- Memorizing and fixing visual data.
In addition to recognizing speech intonation, the non-dominant lobe also analyzes it and subsequently integrates images into the general emotional attitude towards the interlocutor. It is this part of the brain that allows a person to know whether his conversation partner is happy with him or wants to get rid of him as soon as possible.
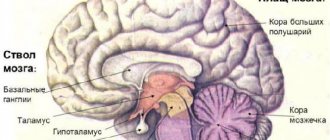
Anatomical features of the brain structure
The structure of the brain of the head is a complex structure consisting of approximately 25 billion neurons, localized in three important zones - anterior, middle and posterior.
In the human embryo, these zones are formed during the first month of intrauterine development and are clearly visible when examined after reaching four weeks. The gray mass of the brain is protected by three membranes - hard, soft and arachnoid. They protect the brain from external damage.
The most ancient parts of the hindbrain and midbrain are considered. Thanks to them, the most important functions are carried out. This is a normal process of blood circulation and respiration, without which the life of the human body is practically impossible. Carrying out communication interaction with the realities of the surrounding world, namely the ability to think, express emotions, the presence of memory, speech, hearing - is the prerogative of the front part of the brain.
In addition to identifying the three main zones of the most important human organ, the main principle of its organization is the division of functions into two hemispheres - left and right. They are connected by many nerve fibers and are practically indistinguishable from each other. However, in the absence of visible external differences and active joint activity, there is a significant difference in the functional asymmetry of their work. For example, one of the hemispheres (usually the right) performs dominant functional duties. This is where the correlation of one category of people with the so-called right-handed people, and the other with left-handed people, arose.
The brain structure of the head is a complex structure consisting of approximately 25 billion neurons
In addition to the distribution of the highest functions of the organ across different parts and hemispheres, ensuring consistency in its different zones is due to the performance of certain functions by the lobes of the brain located in the cerebral cortex. There are only four of them. These are the frontal, temporal, parietal and occipital lobes, each of which has its own species pair.
METHODS FOR STUDYING THE FUNCTIONS OF THE CEREBRAL CORTEX
A significant number of methods are used in physiology to study the activity of the cerebral cortex. Some methods can only be used in so-called acute experiments, when the animal is under anesthesia and dies after the experiments; other methods make it possible to study for a long time. To study the functions of such a complex organ as the cortex, the greatest results are obtained by methods that allow research to be carried out over several months and even years.
Rice. 2 DIAGRAM OF THE COURSE OF NERVE FIBERS IN THE LARGE HEMISPHERES OF THE BRAIN. 1 - short associative fibers; 2 - long associative fibers; 3 - commissural fibers that communicate between both hemispheres of the pulp; 4 - centrifugal fibers
Let's get acquainted with some methods for studying the activity of the cerebral cortex.
Removal of individual sections of bark.
The essence of the method is that certain areas of the animal’s cortex are surgically removed. After the wound heals, when the animal recovers, the changes that have occurred in the animal’s behavior are observed. Based on the resulting disturbances, conclusions are drawn about the functions of the remote area of the cortex.
Electrical stimulation method
This method makes it possible, after opening the skull of an experimental animal or a person during brain surgery, to apply electrical stimulation to various points of the cortex. Thus, it is possible to establish the motor zone of the cortex and study its individual areas, the irritation of which causes the contraction of certain specific muscle groups. When studying the functions of the human cortex, this method turned out to be productive, since a person, when the cortex is irritated, is able to respond and communicate to the researcher the sensations that he experiences.
Chemical irritation method
To cause chemical irritation to the cerebral cortex, some poisons are used, most often strychnine.
To study the cortex, the property of strychnine to sharply increase the excitability of the nervous system was used. A small piece of filter paper is moistened with a solution of strychnine and applied to the area of the bark being examined. The excitability of the area of the cortex to which strychnine is applied increases sharply, which is reflected in the animal’s reactions. By studying these changes and knowing where the piece of paper moistened with strychnine solution is attached, they get an idea of the functions of this area.
Study of brain currents
The study of electrical phenomena in the brain first began in our country.
Much earlier than foreign authors, these studies were carried out by V. Ya. Danilevsky, I. M. Sechenov, N. E. Vvedensky, B. F. Verigo, V. V. Pravdich-Neminsky. In 1877, V. Ya. Danilevsky first published his research, which showed the presence of rhythmic electrical oscillations in the brain. He established a connection between the activity of the brain and the electrical fluctuations it observed. Soon after the work of V. Ya. Danilevsky, I. M. Sechenov in 1882, while studying electrical phenomena in the medulla oblongata, established the rhythmic nature of these phenomena and made a number of other observations.
In 1884, N. E. Vvedensky, applying to the cerebral cortex the technique he developed of listening to electrical muscle currents through a telephone receiver, grasped the rhythmic nature of electrical phenomena.
The modern method of electroencephalography, i.e., recording the biocurrents of the brain, allows, by applying special electrodes to the cerebral cortex or scalp during the experiment, to divert the currents of the cortex and record them. A recording of brain currents is called an encephalogram. Recording action currents during work and at rest, during sleep and during various other types of activity, as well as their further comparison, make it possible to draw certain conclusions. In Fig. 125 shows the electroencephalogram of a person during rest and work.
Clinical method
It consists in studying changes in the normal activities of individual
organs and organ systems that are observed in people as a result of hemorrhages, injuries or brain tumors. If patients die, an autopsy is performed to determine which areas of the brain have undergone changes. Knowing the disturbances in the body's activity, it is possible to establish the function of the affected area of the cerebral hemispheres.
As already indicated, all these methods for studying the functions of the cerebral cortex make it possible to study only specific issues of the activity of the cerebral hemispheres. The study of the true physiology of the cerebral cortex became possible only in connection with the creation of the method of conditioned reflexes by I. P. Pavlov.
Important What is ventriculomegaly in the fetus
Article on the topic of the cerebral hemispheres
A large contingent at a children's outpatient clinic consists of patients with no signs of damage to the nervous system, but with a variety of health problems, which are manifested by complaints of headaches, sleep disorders, attention deficit, as well as mild signs of developmental delay, etc. In these cases, an electroencephalographic examination plays an important, sometimes decisive role. Even if changes in the EEG are not specific, they provide the doctor with additional diagnostic information about the functional state of a particular part of the cerebral cortex, and also make it possible to determine the nature of diagnostic tasks.
The literature often discusses the problems of functional disorders in various parts of the cerebral cortex. An analysis of relevant sources devoted to this problem was presented in the review article “Features of the formation and association of changes in the EEG in the occipital region in children with clinical manifestations”[].
The purpose of this study was: to identify the conditions most common in children with pathological changes on the EEG in the occipital region; establishing factors influencing the state of the cerebral cortex (its occipital region); assessment of treatment effectiveness.
Material and methods
The study was conducted on the basis of the city office of epilepsy and paroxysmal conditions at the Morozov Children's City Clinical Hospital, where 52 children were examined.
The majority of patients were 5 and 6 years old (6 and 10 people, respectively) and 11 and 12 years old (8 and 6 people, respectively). There were 2.5 times more boys among the observed children than girls (37 versus 15).
The reasons for patients to contact a neurologist and record an EEG were: routine examination of children in connection with somatic diseases (usually bronchial asthma, a history of traumatic brain injury (TBI), complaints of headache, attention deficit hyperactivity, delayed psycho-speech development, fainting); less often - parasomnias, tics, behavioral and learning disorders, fears, enuresis, dizziness, paroxysmal vomiting.
The main criteria for inclusion in the study were: the presence of pathological changes in the EEG in the occipital region using unified concepts and criteria in accordance with the classification of the International Federation of Electroencephalographic Societies and Clinical Physiology (IFSECN); no history of epileptic seizures or signs of epileptic encephalopathy.
Data from medical history, neurological examination, EEG and magnetic resonance imaging (MRI) were analyzed. Follow-up observation ranged from 1 year to 3 years.
results
In table Table 1 shows the EEG features in the studied cases.
These changes in 4 (7.6%) cases were combined with discharges of generalized epileptiform activity in the form of peak-slow wave complexes with a frequency of 2.5-3.2 Hz, lasting no more than 3 s in the background recording. In 4 (7.6%) patients, diffuse epileptiform activity appeared in response to hyperventilation (HV); in 4 (7.6%) children (according to an extract from the outpatient card), the phenomenon of secondary bilateral synchronization was previously noted; in 3 (5.7%) cases a photoparoxysmal response was recorded; Moreover, in 2 of these children, blocking of pathological activity when opening the eyes was noted.
Almost all (92%) patients were found to be burdened by certain harmful substances in the perinatal period. Every 5th child has suffered a TBI (concussion).
A survey of parents showed that most often in families of children there were patients with migraine (18%), headaches of various origins (15%), less often - diseases such as epilepsy and febrile convulsions in relatives (3.8% each), and in isolated cases - alcoholism, thyroid pathology, speech impairment in childhood, psychopathology.
In the neurological status, 46% of children showed diffuse microsymptoms (anisoreflexia, muscle tone disorders, motor clumsiness), 12% had autonomic dysfunction (marbling of the skin, hyperhidrosis, etc.).
According to the International Classification of Headache Pain (ICHD II), the headache that occurred in the examined patients corresponded to tension-type headache (TTH).
MRI of the brain (in some cases in vascular mode) revealed a number of changes. They are presented in table. 2.
From the data in table. 2 shows that certain changes on MRI were present in 17 (33%) children. These changes were varied, only in ⅓ of cases they can be classified as “conditionally epileptogenic” [1].
The condition of the vessels was assessed using duplex scanning. The following were identified: lability of vascular tone (20% of children), tortuosity of the internal carotid artery (ICA) (15%), venous dysfunction (7.5%), vertebrogenic effect on blood flow through the vertebral artery (VA) (4%) and vertebral hypoplasia arteries (2%).
All children were consulted by a psychologist, and the scope of psychological testing was determined during a conversation with the child and his parents (Table 3).
As for concomitant diseases, only one child was observed by an ophthalmologist from birth for optic nerve atrophy, pathology of other organs - bronchial asthma, tonsillitis, chronic gastroduodenitis, obesity, minor anomalies of heart development, etc. occurred with equal frequency (15% each). There were no severe cases of these diseases, because disabled people were not included in the sample.
During observation, 2 (3.8%) children developed epileptic seizures - one of them was diagnosed with idiopathic occipital epilepsy of the Panagiotopoulos type at the age of 5 years, and a single secondary generalized tonic-clonic seizure was diagnosed in the other at the age of 9 years.
In 5 (10%) cases, a diagnosis of migraine was made, and in 2 cases there were periodic childhood syndromes considered as precursors of migraine - paroxysmal dizziness and cyclic vomiting.
During the observation process, the EEG was studied over time: once every 3 and 6 months, depending on the severity of the changes and the dynamics of complaints (Table 4).
In addition to individual EEG views, in some cases a combination of various changes was noted in the same child.
Five children received anticonvulsant therapy, and in 3 cases treatment was prescribed by psychiatrists based on complaints of behavioral disturbances in the child and taking into account EEG data. Finlepsin was prescribed by a neurosurgeon in connection with a TBI; another was prescribed by a neurologist at a district clinic based on EEG data. None of these patients showed normalization on the EEG after 3 and 6 months of taking antiepileptic drugs and they were discontinued due to clinical ineffectiveness and side effects. In all 5 cases, treatment was also carried out with vascular, metabolic, nootropic drugs (pantogam, tanakan, neuromultivit, elkar, hypoxen, cogitum, fezam, etc.), which made it possible to state a subjective improvement in the condition of the children, although EEG changes, as mentioned above, were preserved.
Discussion
Thus, from the general group of children who had pathological changes on the EEG in the occipital region, only 15% during the observation process manifested paroxysmal conditions - epilepsy and migraine. This differs from the data of D. Talwar et al. [11], who, during a selective examination of adolescents with spike-wave paroxysms in the occipital region, found the manifestation of paroxysmal phenomena - epileptic manifestations and migraine in 80% of children, while the combination of migraine and epilepsy was 2 times more common than isolated migraine. Focal convulsive seizures predominated (75%), absence seizures were registered in ¼ of the examined patients. Migraine was in most cases associated with idiopathic partial forms of epilepsy. The authors noted the nonspecificity of epileptiform changes in the occipital leads, which can appear in both idiopathic partial and symptomatic partial, as well as absence forms of epilepsy and in patients who had no indication of a history of seizures.
Analyzing the identified local changes in the EEG in children without a history of epileptic seizures, P. Lerman, S. Kivity-Evhraim [8] found that they are more often recorded in the rolandic region and somewhat less frequently in the occipital region. These focal discharges are age-dependent and tend to disappear by adolescence. All the patients they examined complained of headaches, syncope, behavioral problems and learning difficulties. The main conclusion that the authors draw is that children with such EEG changes should not be regarded as having epilepsy and do not need to be prescribed anticonvulsants.
Among the patients we examined, we also noted an age-related relationship between changes in the EEG and the nonspecificity of the complaints presented.
Prescribing anticonvulsants to patients under our supervision did not lead to normalization of the EEG and the disappearance or reduction of complaints. Clinically, the prescription of syndromic therapy turned out to be more effective, which also confirms the nonspecificity of EEG changes in the occipital region in relation to epilepsy and their connection mainly with immaturity and developmental features of the cerebral cortex.
A. Fois et al. [5] studied clinical manifestations in patients with occipital paroxysms recorded on EEG and noted mental retardation, neurological symptoms, and visual symptoms; among them, 3% had idiopathic occipital epilepsy with visual seizure phenomena, and 20% had other types of seizures. In 8.5%, changes in the EEG disappeared during observation (children were observed from the moment of registration of pathological phenomena on the EEG until they were 15 years old), of which 5.5% also showed clinical normalization. This work indicates a fairly high frequency of epileptic seizures - 23%. Note that in our study, epilepsy developed only in 3.8% of cases, although EEG normalization was noted in a slightly larger percentage of cases.
Analyzing the reasons for contacting a neurologist and prescribing an EEG examination, it can be noted that this practice in pediatrics has justifiably become widespread for complaints of headaches. Among the patients we examined, children with similar complaints made up ¼ of all patients.
J. Valdozan et al. [12] as a result of an electroencephalographic examination of children with headaches (tension headache, migraine with aura, migraine without aura), found that the EEG of patients with tension headache and migraine without aura does not differ from the EEG of healthy children, while in in children with migraine with aura, theta activity increases in the occipitotemporal regions.
F. De Romais et al. [4] in patients with basilar migraine during dynamic observation revealed periodically recorded spike-wave activity in the occipital leads, which disappeared with age, which confirms the connection of these diseases and the involvement of the occipital cortex. P. Camfield et al. [3] also observed adolescents with basilar migraine, in whom rhythmic discharges of acute-slow wave complexes were recorded in the temporo-occipital region, and less commonly, generalized spike-wave bursts that “responded” to treatment with anticonvulsants.
The appearance of migraine in patients during our observation confirms the role of the occipital cortex in this form of neurological pathology, which was noted earlier [4]. It was the EEG changes in our patients that made it possible to identify periodic childhood syndromes (precursors of migraine) in the anamnesis and to concentrate attention on the family history and complaints that parents either did not pay due attention to or misinterpreted.
M. Libenson et al. [9], having examined children with occipital epileptiform activity, noted that in 50% of cases there was symptomatic epilepsy (with cerebral palsy, brain dysgenesis, genetic disorders), in 34% - idiopathic epilepsy (of which 21% - benign occipital epilepsy) , in 1% - febrile seizures. Among the patients we examined, residual changes on brain MRI were recorded in every third child, but only one developed cryptogenic epilepsy; no febrile seizures were recorded.
In a study of children with attention deficit hyperactivity disorder conducted by J. Hughes et al. [6], ⅓ of them showed focal epileptiform activity, usually in the occipital or temporal localization, while slow-wave activity predominated in the anterior parts of the cortex - frontal and anterior temporal. Complaints about hyperactivity, attention deficit, learning difficulties among patients in our study were made by about 20% of children, but during psychological testing, attention deficit hyperactivity syndrome was not confirmed and a disharmonious type of mental development, impaired visual perception, limited productivity of memory, attention, increased exhaustion. R. Nass et al. [10] in 7 out of 42 examined children with autistic disorders, regression of speech and social skills and behavior on the EEG, spikes were found in the occipital region. Evaluating the results of the examination, the authors conclude that although nuchal commissures in young children can be considered as an age-related benign phenomenon, their high frequency in a population of patients with cognitive difficulties indicates a cause-and-effect relationship between clinical and neurophysiological phenomena.
Among the patients we examined, ¼ of the children had delayed psycho-speech development and autistic-like behavior, but they differed from the children described in the above works [6, 10], since they dealt with psychiatric patients. Our study included children who applied to a neurologist.
An observation of 200 children without epileptic seizures in a psychiatric hospital was presented by L.R. Zenkov [2]. In 7.5% of them, routine EEG revealed occipital, predominantly right-hemispheric spikes. The following types of disorders were found: general mental retardation - in 53% of cases, violation of spatial and visual gnosis - in 47%, behavioral disorder - in 53%, attention deficit and hyperactivity - in 46%, autism - in 2%, school impairment learning - in 87%, speech impairment - in 47%; in most children these disorders were combined. When assessing the results of this study, it is necessary to take into account that the examination was conducted in a psychiatric hospital.
A. Kozik [7], in a study of 511 children aged 1 to 18 years, showed that occipital, posterior parietal and posterior temporal EEG foci significantly predominated in the right hemisphere in young children. The author believes that epileptogenicity is associated with immaturity of the cortex, and the indicated age dynamics are due to the sequence of maturation of the right hemisphere and posterior parts of the brain first. In our study, only a slight predominance of changes in the right hemisphere was noted (27 right-sided versus 25 left-sided).
Summarizing the observations of children with EEG changes in the occipital areas of the cerebral cortex, who had no history of epileptic seizures and signs of epileptic encephalopathy, we can first of all note the variety of complaints when contacting a neurologist. A high incidence of perinatal complications and a history of traumatic brain injury was also noted, which cannot but affect the development of the cerebral cortex. In addition, a high frequency of migraine and headaches was registered in the families of the examined children, which indicates the existence of a connection between the occipital cortex and migraine. At the same time, there were 4 times fewer family cases of epilepsy than cases of migraine. In the observation we presented, the number of cases of epilepsy development was significantly less than in other studies [2, 4, 5, 8, 11]. During follow-up, migraine was diagnosed 2 times more often than epilepsy.
In ⅕ of the children we examined, stable normalization of the EEG occurred during the observation period, and this was more than in the works cited above [5, 8, 11]. However, in most other patients, cortical rhythm disturbances persisted, with generalized epileptiform activity joining the pre-existing changes and a photoparoxysmal response appearing.
There is reason to believe that the relatively high frequency of subclinical epileptiform changes on the EEG is associated with age-dependent hyperexcitability of the child’s cerebral cortex, its immaturity and reduced resistance to such unfavorable factors as perinatal burden, head injury, and somatic diseases. This is indirectly confirmed by the fact that among children who did not have an epileptic history, patients with signs of delayed mental development of varying degrees of severity predominated.
Also noteworthy was a wide range of somatic pathologies, which could also influence the development of the occipital cortex. However, in the literature there is almost no data on changes in the EEG in children with certain somatic diseases, which complicates this kind of interpretation, especially in terms of the predominant effect on the visual cortex.
The frequency and severity of vascular disorders in our patients were small, which makes assessing their effect on cortical disorders in the occipital region difficult, especially since in pediatric practice there is no uniform approach to assessing blood flow.
Based on the data presented, in general, when examining children with headaches, we can recommend the widespread use of EEG.
Our experience in treating children with EEG changes in the occipital region in the absence of epileptic seizures and the exclusion of epileptic encephalopathy shows that the use of anticonvulsants in these cases is ineffective. Carrying out syndromic treatment using nootropics, metabolics, vitamins, herbal sedatives, antihypoxants, venotonics and anxiolytics can improve the well-being of children, and in some cases normalize the EEG.
Thus, analysis of literature data and our own results confirm the frequency of epileptiform changes on the EEG in children without an epileptic history as a manifestation of cortical immaturity and perinatal pathology. Chronic somatic diseases and a history of TBI are unfavorable environmental factors affecting the maturation of the cerebral cortex, which require electroencephalographic monitoring.
[] Journal of Neurology and Psychiatry 2011; 111:4:96-100.
Assigned functions
The functions of the occipital lobe of the brain are associated with the analysis, perception and containment (storage) of visual information. The visual tract consists of several points:
- An eye with its retina. This paired organ is only a mechanical component of vision, performing an optical function.
- Optic nerves, through which electrical impulses directly travel at a certain frequency and carry certain information.
- The primary centers are represented by the visual thalamus and quadrigeminal.
- Subcortical and cortical centers. All of the above structures act as points of elementary perception and delivery of information. The visual cortex, in contrast, plays the role of a higher analyzer, that is, it processes the received nerve impulses into mental visual images.
It is noteworthy that the retina of the eye perceives a set of light waves, each of which has a length and consists of quanta of electromagnetic radiation. But the cortex, evolving over millions of years, “learned” to work with such signals and turn them into something more than a set of energy and impulses. Thanks to this, people have a picture of the environment and the world. Thanks to this crust, we see the elements of the universe as they appear.
The visual cortex, located on both hemispheres of the occipital lobe, provides binocular vision - the world appears three-dimensional to the human eye.
The human brain is a multifunctional structure, like each area of its cortex - therefore, the occipital lobe of the brain in a standard functional state takes little part in processing auditory and tactile signals. Under conditions of damage to neighboring areas, the degree of participation in signal analysis increases.
The visual cortex, called the association area, constantly interacts with other brain structures, forming a complete picture of the world. The occipital lobe has strong connections with the limbic system (especially the hippocampus), parietal and temporal lobes. Thus, a particular visual image may be accompanied by negative emotions, or vice versa: a long-standing visual memory evokes positive feelings.
The occipital lobe, in addition to simultaneous analysis of signals, also plays the role of an information container. However, the amount of such information is small, and most environmental data is stored in the hippocampus.
The occipital cortex is strongly associated with theories of feature integration, the essence of which is that the cortical analytical centers process individual properties of an object (color) both separately, in isolation, and in parallel.
To summarize, we can answer the question of what the occipital lobe is responsible for:
- processing visual information and integrating it into a general attitude towards the world;
- storage of visual information;
- interaction with other areas of the telencephalon and partial succession of their functions;
- binocular perception of the environment.
https://youtube.com/watch?v=c-grDqnqQgM
https://youtube.com/watch?v=c-grDqnqQgM
Functions of the pons
The bridge is a small ridge with a depression (basilar groove), which contains a large amount of nerve fiber. The hindbrain is the pons located under the cerebellum. The main purpose of this structure is to transmit information from the back part to the largest part - the forebrain.
The functionality of the bridge is to support unconditioned reflexes (protective) in the body:
- Cough;
- Sneezing;
- Vomit;
- Blinking.
The pons Varoliev forms descending pathways through which impulses pass not only to the cortex of the central nervous system, but also in the opposite direction. Thus, the rhomboid region is connected with the spinal canal and with all the structures in its anatomical structure.
Dorsal and lateral routes
Once information has passed through the primary visual cortex into the occipital lobe, the data stream that this area emits bifurcates along two different routes: ventral and dorsal. As we will see, they propagate in parallel, interacting with parts of the brain that the other route does not directly access.
Through the abdominal
The ventral pathway starts from the primary visual cortex in the occipital lobe and goes to the frontal region of the brain through the lower part of the brain, which includes the visual cortices V2 and V4, which, as indicated by their number, are responsible for processing information already processed by v1.
It is believed that neurons involved in this "assembly line" of visual information are responsible for processing the characteristics of individual elements that are viewed at any time - that is, the content of the vision. Therefore, this route is also called the "what" route.
Dorsal path
This pathway runs from the occipital lobe to the frontal cortex through networks of neurons near the top of the skull. In it, information processed by the primary visual cortex reaches the parietal lobe through visual cortices v3 and v5. This visual processing area is thought to be responsible for establishing the location and motion characteristics of what is seen; This is why the spinal track is also called "where and how".
Along with the ventral pathway, this visual processing pathway, associated with the occipital lobe, tells us about how the brain works: sometimes mental processes that seem to form a single whole and come to our consciousness as a holistic experience are actually the product of several brain pathways that operate in parallel, each focusing on a different aspect.
Forebrain
The functions of the forebrain are the most complex. It is responsible for mental activity, learning ability, emotional reactions and socialization. Thanks to this, it is possible to predetermine the characteristics of a person’s character and temperament. The anterior part is formed at 3-4 weeks of pregnancy.
To the question of which parts of the brain are responsible for memory, scientists have found the answer - the forebrain. His cortex is formed during the first two to three years of life, for this reason a person does not remember anything before this time. After three years, this part of the brain is able to retain any information.
A person's emotional state has a great influence on the front part of the brain. Negative emotions have been found to destroy it. Based on experiments, scientists answered the question of which part of the brain is responsible for emotions. They turned out to be the forebrain and cerebellum.
The front part is also responsible for the development of abstract thinking, computational abilities and speech. Regular mental training can reduce the risk of developing Alzheimer's disease.
Pathologies of the cerebral hemispheres
When the cortex of any lobe of the cerebral hemispheres is damaged, various neurological symptoms and syndromes occur.
The reasons for the development of such conditions are:
- head injuries;
- oncological diseases (benign and malignant brain tumors);
- atrophic diseases of the brain (Pick's disease, Alzheimer's disease);
- congenital disorders (insufficient development of nervous system structures);
- birth injuries of the skull;
- hydrocephalus;
- infectious and inflammatory processes in the membranes of the brain (meningitis, encephalitis);
- circulatory disorders in the vessels of the brain.
Disorders in the frontal cortex
When the frontal cortex is damaged, depending on the location, the following symptoms occur:
- frontal ataxia - imbalance, unsteadiness of gait;
- increased muscle tone in the limbs (passive movements are limited or difficult);
- paralysis of a limb/limbs on one side;
- tonic/clonic seizures;
- seizures (tonic-clonic or epileptic);
- speech difficulty (a person cannot find synonyms, case, time of action) - Broca's aphasia;
- symptoms of the frontal psyche (a person behaves foolishly, relaxed, rage may appear for no reason);
- “frontal signs” (the appearance of primitive reflexes, such as in a baby - proboscis, grasping, etc.);
- loss of smell on one side.
Important Nervousness
In addition to the pronounced symptoms of the frontal psyche, the patient may behave apathetically, indifferently, and not come into contact with others. In severe cases, there may be a tendency to immoral social actions: fights, rowdyism, arson.
Pathological disorders in the parietal lobe cortex
When the cortex of the parietal lobe is damaged, disturbances in sensitivity and surrounding perception occur. The following symptoms are characteristic:
- disorders of skin sensitivity;
- posturality (changes in position in space, passive movements that the patient feels, but this does not happen to him);
- lack of perception of parts of your body;
- inability or refusal to respond to stimuli in areas of superficial and deep sensitivity;
- loss of reading, writing, and counting skills;
- inability to find familiar places;
- when examining objects with closed eyes, the patient cannot recognize a familiar thing.
Pathological disorders in the temporal lobe cortex
The main manifestations of damage to the temporal lobe are:
- cortical deafness (hearing loss without injury to the ear);
- Wernicke's aphasia – loss of the ability to perceive speech, music, etc.;
- noise in ears;
- dream-like states (the patient remembers something that he has not seen or heard before, but claims that it happened to him in reality, and not in a dream);
- the occurrence of auditory hallucinations;
- short- or long-term memory loss (amnesia);
- the occurrence of moments of déjà vu;
- combined hallucinations (auditory + visual, auditory + olfactory);
- temporal lobe seizures.
Pathological disorders in the occipital lobe cortex
Damage to the cortex of this area is accompanied by problems with the visual analyzer. Conditions such as:
- cortical blindness (complete loss of vision without damage to the visual analyzer);
- loss of vision, in which the patient claims that he has not lost his sight;
- hemianopsia – loss of visual fields on one side;
- inability to remember an object, color, or person's face;
- changes in surrounding objects that seem small - visual illusions;
- visual hallucinations – flashes of light, zigzags, individual for each eye.
When the limbic system is damaged, memory loss or confusion of memories occurs, there is an inability to create and remember bright moments in life, low emotional lability, lack of smell, loss of the ability to analyze and make decisions, as well as master new skills.
The cerebral hemispheres play a huge functional role in the human body. The ability to write, read, analyze information, perceive and navigate in space, feel, hear, see, smell help the body adapt to the world around it. When certain areas of the cortex are damaged, pathological syndromes and symptoms arise, which can be used to indicate the location of the affected area.
Interaction of brain parts
Each section of the complex structure that is the human brain performs certain functions. At the same time, the holistic activity of the most important organ of the nervous system is aimed at determining consciousness, forming character, temperament and important psychological aspects of behavior.
A feature of the interaction of all brain structures is the fact that despite the clear distribution of the functional load between its lobes, there is a possibility of redistribution of these functions. For example, when an injury or disease develops in one of the lobes, its function is performed by another part of the brain.
The coordinated activity of all brain structures becomes a prerequisite for the performance of its functions and the harmonious maintenance of balance throughout the human body.