A disorder acquired as a result of gradual progressive destruction in a patient of nerve cells that are responsible for coordination functions is known as Parkinson's disease. The initial symptoms of the disease are tremor (shivering) of muscle tissue, instability of some parts of the body at rest (hands, fingers, head). Such symptoms are most common among citizens aged 55-60 years, but there have also been cases when the disease began to manifest itself in citizens under 40 years of age. As the disease progresses, a person completely loses any physical activity and intellectual abilities, all this leads to the extinction of vital activity and death. This disease is one of the most difficult to treat. How long can a person with such a diagnosis live with modern medicine? Accommodation and care in specialized boarding houses for the elderly significantly increases life expectancy with this disease.
The emergence of Parkinson's disease
The entire system of coordination of human movements is controlled by his central nervous system, which includes the brain as well as the spinal cord. As soon as the patient thinks of making any movement, the cortex of his brain activates all parts of the nervous system responsible for physical activity. The basal ganglia is one such part. This is an auxiliary motor mechanism responsible for the speed of movement, quality and accuracy of execution.
Activity signals travel from the human cortex to the basal ganglia compartment. The ganglia are responsible for determining the specific muscles involved in the movement process, the work of each of them and the degree of their tension. All this happens so that the accuracy and purposefulness of movements corresponds to intentions.
Impulses from the basal ganglia are transmitted using neurotransmitters (special chemicals). The work of muscles depends on the amount of such substances and the process of their influence.
One of the most important neurotransmitters is dopamine, which helps inhibit nerve signals, controlling the accuracy and force of contraction of each muscle. In the most complex coordination of movements, part of the work is done by the “Nigral Substantia”, delivering dopamine to the striatum, thereby sending signals from the basal ganglia to the rest of the brain. “Substantia nigra” has this name because of the dark color of this brain structure, since the by-product of dopamine biosynthesis, melanin, is found there in large quantities. So, Parkinson’s disease is caused by insufficient levels of dopamine in the substantia nigra.
Causes of the disease, is there any reason to worry?
Clearly identified reasons for the development of the disease have not yet been established.
One of the main factors leading to Parkinson's disease is genetic predisposition. According to statistics, 15 patients out of 100 in their family had this disease. Articles on the topic
- Forms of autism in adults 09/25/2021
- Necessary help for teenagers with autism 09/21/2021
- Stages of alcoholism in women: main signs 06/24/2021
- Split personality: symptoms and signs of the disease in women 06.24.2021
In 20% of cases, parkinsonism is a complication of other diseases. In other cases, what exactly serves as an impetus cannot be determined.
It is believed that the development of the disease is influenced by the general environmental situation and living environment:
- quality of water and food consumed;
- air purity;
- poisoning with toxic gases and other circumstances.
The sooner the symptoms of Parkinson's disease in women are noticed and treatment is started, the better the condition can be stabilized and the progression of the disease can be slowed down.
What is Parkinson's disease
Parkinson's disease is a neurodegenerative brain disease that develops slowly in most cases. Over the course of many years, the symptoms of this pathology may progress unnoticed. Due to the death of a significant number of neuronal cells in areas of the basal ganglia and degradation of nerve fibers, this disease occurs. Symptoms of Parkinson's disease begin to actively manifest themselves when the functions of 80% of neural connections are impaired. In such cases, Parkinson's disease is incurable and develops over time, despite all the therapy taken.
Neurodegenerative diseases are a group of diseases that develop slowly and are characterized by hereditary or acquired lesions of the central nervous system.
Another specific feature of Parkinson's disease is a sharply reduced amount of dopamine. Its quantity is no longer sufficient for the necessary inhibition of nerve impulses flowing from the cerebral cortex. Thanks to this, nerve impulses go straight to muscle tissue, stimulating its tension. This is typical for the most striking manifestations of Parkinson's disease: muscle contractions (trembling and tremors), stiffness of muscle activity due to excessively high tone, manifestations of unintentional body movements.
The dangers of Parkinson's disease
The main danger of Parkinson's disease is that the patient can become completely incapacitated and bedridden.
As for disability, the first group is assigned to patients who have pronounced disabilities and have lost the ability to self-care. The second disability group is given to patients who have serious difficulties in moving. The third group is assigned in case of moderate difficulties in self-care and movement, when disability limitations are minimal.
Life expectancy with Parkinson's disease
Parkinson's disease is a chronic disease. It cannot be completely cured. The life expectancy of people diagnosed with pathology depends on timely diagnosis. If the disease is detected in the early stages and medical treatment is selected correctly, life expectancy remains almost unchanged. In this case, the patient must do gymnastics, massage, follow a diet, and follow all medical recommendations.
In the absence of adequate therapeutic therapy and the rapid progression of the disease, death can occur within 5-7 years.
Parkinson's disease and Parkinsonism
There are two types:
- "Primary parkinsonism" or Parkinson's disease. This is an irreversible, quite common case.
- "Secondary parkinsonism". Characterized by brain damage resulting from infectious or traumatic events. As a rule, it can be treated and restored. It can occur at any age under the influence of external factors.
The following can lead to secondary parkinsonism:
- Various brain injuries.
- Various toxic poisonings.
- Encephalitis.
- Vascular lesions in the brain (coronary artery disease, stroke or atherosclerosis, etc.).
Diagnosis of Parkinson's disease
Clinical diagnosis of the disease takes place in three stages.
Stage I
Parkinsonism syndrome is recognized and its symptoms are compared with other psychopathic and neurological pathologies that manifest themselves in a similar way. The main symptom of the disease is hypokinesia, combined with muscle rigidity, resting tremor or postural instability. However, it is not associated with visual, cerebellar and vestibular disorders.
Stage II
Provides for the exclusion of the presence of other diseases manifested by parkinsonism syndrome. The doctor pays attention to a number of criteria:
- prolonged remission;
- oculogyric crises (gaze convulsions);
- use of antipsychotics before the onset of the first symptoms of the disease;
- clear manifestation of dementia;
- Babinski reflex;
- manifestation of autonomic failure;
- cerebellar symptoms;
- unilateral manifestation of pathology for more than 3 years;
- supranuclear gaze palsy;
- lack of effect from taking Levodopa;
- detected open hydrocephalus/brain tumor;
- a history of strokes with progression of symptoms of Parkinson's disease;
- repeated traumatic brain injuries.
Stage III
Symptoms are identified that allow an accurate diagnosis to be made. To do this, you must have at least three criteria from the list:
- presence of rest tremor;
- greater severity of symptoms on the side of the body on which the disease debuted;
- presence of a reaction to taking Levodopa;
- effectiveness of Levodopa for at least 5 years;
- duration of illness from 10 years;
- progressive course of the disease.
When evaluating patients with symptoms of Parkinson's disease, the following are used:
- Electroencephalography (EEG). Biological signals coming from brain cells are recorded. The functional activity of the brain is assessed, and pathological disorders present in it are diagnosed.
- MRI of the brain. It makes it possible to see brain structures and visualize the pathological formations present in them, evaluate the parameters of pulse blood flow in the capillary arteries, and identify functional areas of the brain.
- CT scan of the brain. During the examination, the structure of the brain tissue and the structure of the cerebrospinal fluid system are studied. The technique allows you to recognize abnormal processes occurring in the brain and carry out dynamic monitoring of the course of the disease and the effectiveness of the treatment.
- Rheoencephalography. The method is aimed at studying the blood supply to the veins of the neck and head. Makes it possible to study the parameters of pulse blood flow in the arteries of the brain, venous outflow from the cranial cavity.
Differentiation of diagnosis
It is very important during diagnostic measures to differentiate Parkinson's disease from other pathologies manifested by parkinsonism syndrome. This means:
- parkinsonism plus;
- secondary parkinsonism;
- pseudoparksinsonism.
Signs and symptoms
How to spot Parkinson's disease?
The manifestation of the disease is characterized by a persistent loss of control over one’s own physical activity:
- Tremor at rest.
- Lack of mobility and muscle stiffness (rigidity).
- Reduced speed and insufficient range of motion.
- Insufficient ability to maintain balance (instability).
Rest tremor is involuntary small movements that occur in the absence of motor activity. The most common are sudden shaking of the hands and tilted movements of the head.
Signs not related to movement and coordination:
- Excessive fatigue.
- Manifestations of depression.
- Smell disorders.
- Excessive salivation.
- Increased sweating.
- Metabolic disorders.
- Negative changes in the functioning of the stomach and intestines.
- Psychoses and other psychological disorders.
- Degeneration of cognitive functions.
The most noticeable deviations in cognitive functions in parkinsonism are:
- Memory problems.
- Slowness of thought processes.
- Problems with orientation in space.
Clinical picture
Motor symptoms
Hypokinesia
Includes:
- bradykinesia – slowness of movements, exhaustion of repetitive movements;
- oligokinesia - impoverishment of the movement pattern (lack of friendly hand movements when walking, acheirokinesis, hypomimia, microbasia, hypophonia, micrographia);
- akinesia - difficulty starting movements, freezing, difficulty getting up from a chair.
Rigidity
An increase in muscle tone of the plastic type, defined as resistance during passive movements.
Tremor
Rhythmic tremors with a frequency of 3–6 Hz, involving the distal parts of the extremities, decreasing or disappearing with movement.
Postural instability
Violation of reflex reactions to a shift in the center of gravity of the body, leading to an inability to maintain balance when changing posture.
Walking disorders
Slow, “shuffling” gait with a shortening of the step length, in the later stages - with “freezing” and involuntary runs forward - propulsions.
Non-motor symptoms
Constipation
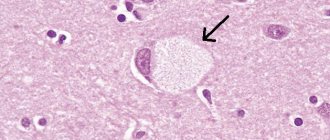
The formation of Lewy bodies in the structures of the peripheral part of the autonomic nervous system in PD also involves the intermuscular nerve plexus of the intestine with the development of sympathetic denervation of the colon. This is manifested clinically by a longer food transit time and the development of constipation.
Constipation, being one of the most common non-motor symptoms, occurs in patients with PD much more often than in the general population - in 50–80% of cases. In a quarter of patients, constipation occurs before the onset of motor disorders; patients often do not complain about them, not associating them with the disease. The presence of constipation should be actively questioned.
A statistical relationship was shown between the presence of constipation and the severity of the disease on the Hoehn-Yahr scale, depression, anxiety and autonomic disorders.
Constipation has a significant impact on the quality of life of patients with PD.
Studies use the Rome IV* criteria to define constipation in PD:
Rome criteria for constipation IV
- 2 or more conditions must be met**
- straining during more than ¼ of cases (25%) of bowel movements;
- lumpy or hard stools (Bristol Stool Shape Scale 1–2) in more than ¼ of bowel movements (25%);
- a feeling of blockage/obstruction of the anus in more than ¼ of cases (25%) of bowel movements;
- manual aids to facilitate defecation are used in more than ¼ of bowel movements (25%) (eg, digital evacuation, pelvic floor support);
- less than 3 spontaneous bowel movements per week.
- Defecation without the use of laxatives is rare.
- There is insufficient data to make a diagnosis of irritable bowel syndrome.
* Compliance with the criteria is noted for no more than 3 months, the development of symptoms before diagnosis is noted for no more than 6 months.
** In clinical trials, patients who meet diagnostic criteria for opioid-induced constipation should not be diagnosed with functional constipation because it is difficult to distinguish opioid side effects from other causes of constipation. However, clinicians recognize the possibility of a combination of these conditions in the same patient.
Scheme 2. Bristol stool shape scale
Urinary disorders (incontinence, urinary incontinence, sensation of incomplete emptying of the bladder)
Urinary disorders occur in PD significantly more often than in age-matched control groups. Impaired urinary continence is observed in 57–83%, impaired evacuation function – in 17–27%. This ratio distinguishes patients with PD from patients with multiple system atrophy, in whom urinary retention is significantly more common.
The most common symptom in PD is nocturia (nocturnal urination), reported by >60% of patients.
An imperative urge to urinate is observed in 33-54%, frequent urination - in 16-36%.
Sexual dysfunctions
Sexual dysfunction in PD can be either primary, due to progressive damage to the autonomic ganglia, or secondary, due to motor and cognitive impairment, as well as depression and apathy.
57% report a decrease in interest in sex, and 66% have difficulty during sexual intercourse (Santos-García and de la Fuente-Fernández 2013). Erectile dysfunction and other erection-related problems are reported by 79% of patients. The patients' problems are associated with involuntary urination during sexual intercourse, decreased lubrication and vaginismus.
Some patients may experience hypersexuality as an undesirable effect of dopaminergic therapy (much more often when taking DA than levodopa).
Sexual dysfunction has a significant impact on the overall quality of life of patients with PD. An important problem is the low attention of clinicians to these disorders.
Orthostatic hypotension
Orthostatic hypotension (OH) is a decrease in blood pressure by more than 20 mmHg. Art. when moving from a lying position to a standing position.
OH can occur without symptoms, and also have clinical manifestations: increased fatigue, dizziness/a feeling of lightness in the head, pain in the cervical spine (sometimes radiating to the occipital region or shoulders), syncope.
A condition with functionally significant impairments develops in 20–30% of patients with PD. By this time, the disease usually lasts for 10 years or more, in contrast to multiple system atrophy (MSA), when OH occurs in most patients and develops 2–3 years from the onset of the disease.
The mechanisms of development of orthostatic hypotension in PD and MSA may differ: in MSA, the disorder is based on damage to the autonomic structures of the central nervous system; in PD, the main role is played by denervation of peripheral sympathetic structures in the later stages, which is confirmed by numerous studies using myocardial scintigraphy using MIBG (metaiodobenzylguanidine ) for both diseases.
Autonomic disorders, including OH, are more common in PD patients with dementia and dementia patients with Lewy bodies, which may indicate a connection with the formation of Lewy bodies in the structures of the neocortex and limbic system, as well as in parts of the peripheral autonomic nervous system.
In clinical settings, OH is detected using an orthostatic test. A more detailed study of the condition is possible by conducting a long-term passive orthostatic test (tilt test) on a special rotary (orthostatic) table. Having received a positive result, it is necessary to exclude causes other than autonomic dysfunction due to the disease:
- taking medications that lower blood pressure;
- hypovolemia (vomiting, diarrhea, fever, limited fluid intake);
- concomitant diseases (diabetes mellitus and adrenal insufficiency, alcoholism, heart failure).
Hypotension and tachycardia after eating
Postprandial hypotension develops 15–90 minutes after ingestion.
The nature of postprandial hypotension has not been definitively established. Patients do not experience adequate sympathetic compensation when blood flows into the digestive tract after ingestion, which leads to a decrease in cardiac output and peripheral vascular resistance. Another mechanism may be vasodilation in response to the release of insulin and vasoactive gastrointestinal peptide.
Orthostatic and postprandial hypotension often develop in older adults without PD.
Mild cognitive impairment and dementia
Cognitive disorders are more common in patients with PD than in the general population. Over time, dementia develops in 75% of patients with PD (a marker of the late stage of the disease), the prevalence of mild and moderate cognitive impairment (mild neurocognitive disorder according to DSM-5) in patients with PD is estimated at 27% (a large proportion of patients with early stages in the structure of patients explains relatively low prevalence of cognitive impairment).
Mild cognitive impairment may precede dementia or, more often, occur without significant deterioration for the rest of the patient's life.
The development of dementia has a significant impact on the course of PD: it is combined with a more rapid progression of functional impairments, an increased risk of the need for placement in a nursing hospital, and an increase in mortality.
The underlying pathological changes may include Alzheimer's-type changes and chronic vascular damage to subcortical structures, degenerative cortical damage with the formation of Lewy bodies, the latter being considered as the main driving factor. At the neurochemical level, the development of dementia is usually associated primarily with a deficiency of acetylcholine, rather than dopamine.
The clinical profile of dementia in PD includes psychomotor slowing, apathy and bradyphrenia, impaired retrieval, difficulty switching, impaired problem solving, visuospatial impairment, fluctuating attention and cognitive impairment, and significant personality and mood disorders. , hallucinations and psychotic disorders, with comparative preservation of speech functions and praxis.
The Montreal Cognitive Assessment Scale (MoCA) is used to screen for dementia in Parkinson's disease.
Diagnostic criteria for cognitive impairment in PD
A. Meets criteria for mild/moderate cognitive impairment and dementia.
B. Development of disorders in patients with a previously established diagnosis of Parkinson's disease.
C. Gradual onset and slow progression of disorders.
D. The neurocognitive disorder is not associated with another medical condition and is not better explained by a diagnosis of mental illness.
A diagnosis of probable cognitive disorder is established when a case meets all criteria; a diagnosis of possible cognitive disorder is established when one of criteria B or D is not met.
Dementia in PD has the following main features:
- impairments in more than one of the cognitive areas (attention, regulatory functions, visuospatial functions, memory);
- lower level of functioning compared to the state before the disease;
- the impairments are so severe that they cause difficulties in everyday life (social, professional and self-care skills are lost), regardless of motor and autonomic symptoms.
Behavioral disturbances such as apathy, personality or affective changes, hallucinations, delusions and increased daytime sleepiness confirm the diagnosis, but are not required for its formulation.
Apathy
Apathy is observed in 17–80% of patients with PD, much more often than in the general population. In most cases, apathy is combined with other neurocognitive disorders - depression and dementia.
Diagnostic criteria for apathy Starkstein et al. (2009)
A. Decreased motivation compared to the patient's previous level of functioning or normal level for his age or culture.
B. Along with decreased motivation, the presence of at least one of the symptoms belonging to each of the following three groups.
Reducing the activity of goal-directed behavior:
- Decreased effort or energy in performing daily activities.
- Dependence on reminders from third parties when planning daily activities.
Reduced activity of purposeful rational activity:
- Decreased interest in learning new things and gaining new experiences.
- Reduce preoccupation with your personal problems.
Reducing the emotions accompanying goal-directed behavior:
- Persistent or flattened affect.
- Decreased emotional response to positive or negative stimuli.
- Symptoms of apathy cause clinically significant distress or impairment in social, behavioral, or other important areas of functioning.
- The symptoms are not associated with depression of consciousness or the effects of psychotropic substances.
Depression
Clinically significant depressive symptoms occur in patients with PD with a frequency of 40–50%. Of these, less than half reach the level of “major depression.” According to a review by Slaughter JR Slaughter KA (2001), dysthymia (persistent neurotic disorder as defined by DSM-5), minor depression and major depression have a frequency distribution of 22.5%, 36.6%, and 24.8%, respectively.
A review by Williams JR, Hirsch ES (2012) indicated the superiority of the 30-item Geriatric Depression Scale over other instruments when used in patients with PD.
The “gold standard” for identifying depression is a clinical interview with active identification of criteria for this condition.
To reduce time costs, clinical scales are used. The greatest accuracy in the study Goodarzi Z, Mrklas K, 2021 was shown using the 15-item Geriatric Depression Scale.
Anxiety
Anxiety is one of the characteristic personality traits of patients with PD. The prevalence of anxiety and panic attacks in patients with PD is about 40%. The spectrum of anxiety disorders includes social phobia, panic disorder, and unspecified forms of anxiety disorder. In the later stages of PD, the development of panic attacks is combined with a period of shutdown.
Psychosis
Psychotic disorders develop in patients with PD at a higher frequency than in the general population. Their most common manifestation, visual hallucinations, can be experienced by 25–50% of patients at some point in time. Psychosis in PD is accompanied by visual hallucinations in 90% of cases. Auditory hallucinations are rare (8–13% of the number of patients with visual hallucinations), and even less often they are isolated. Hallucinations, usually short-lived, can occur several times a day, more often when the patient is not affected by stimuli - in the evening, in low light, in silence, alone.
There are no generally accepted criteria for diagnosing psychosis in Parkinson's disease; in practice, it is convenient to use the criteria for the preliminary diagnosis of psychosis in Parkinson's disease from the National Institute of Neurological Diseases and the National Institute of Mental Health (2007).
Criteria for the preliminary diagnosis of psychosis in PD
A. Characteristic symptoms . The patient has at least one of the following symptoms:
- hallucinations;
- illusions;
- the feeling that there is someone else in the room (“minor” hallucinations);
- crazy ideas.
B. Diagnosis of the underlying disease . Symptoms develop in patients diagnosed with PD according to UK Brain Bank criteria.
C. Sequence of development of symptoms of psychosis . Symptoms from group A occur in patients after the development of PD.
D. Duration of symptoms . Symptoms from point A recur or persist for ≥1 month.
E. Exclusion of other causes . The symptoms in this paragraph are not more likely to be explained by an alternative diagnosis to PD: dementia with Lewy bodies, mental illnesses such as schizophrenia, schizoaffective disorder, delusional disorder, affective disorders with psychotic symptoms, or general somatic illnesses, including those complicated by delirium.
Additional characteristics of psychosis (specify):
- with/without saving criticism;
- with/without dementia;
- with/without treatment for PD (specify drug, surgical, other treatment).
Risk factors for the development of psychosis in PD are older age, concomitant disorders (depression, rapid eye movement sleep behavior disorder, visual disturbances), taking dopaminergic drugs, high severity of symptoms and disease duration > 10 years, hospitalization.
Psychosis in PD patients with dementia develops with a frequency of up to 70%, and in the absence of dementia - only 10%. Nondemented patients with a history of psychosis have poorer immediate word production and language scores than nondemented patients without psychosis. These facts are explained by pathohistological data on the greater prevalence of Lewy bodies in the parahippocampal and inferotemporal cortex in patients with psychosis in PD.
Impulse control disorders
Disorders include gambling addiction, addiction to gambling, irresistible desire to eat, shop; Punding is the meaningless sorting or arranging of objects.
Sleep disorders
Sleep disturbances are one of the most common non-motor symptoms of PD, occurring with a frequency ranging from 41.1% in primary patients to 78.3% in patients at advanced stages of the disease.
The disturbances are caused by both symptoms of PD (hypokinesia, rigidity, pain) and primary degenerative damage to the structures involved in maintaining sleep (rapid eye movement sleep behavior disorder, restless legs syndrome). They include both nighttime (impaired satisfaction with night sleep, frequent awakenings at night) and daytime (increased sleepiness during the daytime).
Variants of the disease in young people.
There are cases when young people from 20 to 40 years of age develop Parkinson's disease - this is the so-called “early parkinsonism”. But there are not many such patients, according to statistics from 10% to 20%. People with this diagnosis have the same symptoms of the disease, but they are less pronounced and develop much more slowly than in the elderly.
How it manifests itself in young people:
- In many patients, the disease manifests itself as painful spasms of the muscles of the extremities of the body (feet, fingers, shoulders). This symptom can complicate the diagnosis of the disease, as it is very similar to the symptoms of arthritis.
- Undesirable motor activity of the body and limbs, often resulting from dopamine drug therapy.
Further symptoms characteristic of the normal progression of the disease develop.
Diagnostics.
At this time, there are no objective tests whose results may indicate the presence of Parkinson's disease.
Based on the manifestations of the disease, the findings of a physical examination and the results of certain tests, a diagnosis is made. The attending physician can refer you for certain diagnostics (including tests), which will help to recognize and exclude other diseases that cause similar manifestations.
The main sign of the presence of Parkinson's disease is positive changes and a noticeable decrease in symptoms of the disease after the prescription and administration of anti-Parkinsonian drugs.
Also in the modern world there is another diagnostic method - this is Positron Emission Tomography (PET). In a number of circumstances, when using PET, it is possible to identify insufficient levels of dopamine in certain areas of the brain, which is the root cause of Parkinson's disease. But this technique is very rarely used for diagnostic examination of Parkinson’s disease, since it is quite expensive and not many medical institutions are provided with such equipment.
Symptoms and signs of Parkinson's disease in women
The main symptom of the disease is slowness of movement and stiffness. As the disease progresses, the gait becomes disrupted—it becomes shuffling and the steps become small.
But the first signs of Parkinson's in adult women are usually different:
- the appearance of tremor in one of the hands, even at rest;
- decreased facial expression;
- deterioration in dexterity;
- difficulty performing many simple actions, such as getting up from a chair or turning over in bed.
Trembling of the upper extremities may increase when it is necessary to perform any actions:
- write;
- brush your teeth;
- typing text on a computer and so on.
Parkinson's disease symptoms and signs in women are initially mild, which can go unnoticed by others for a long time. Especially when poor coordination alternates with bursts of physical activity. In older women, such manifestations of a decline in dexterity can be attributed to age-related changes, which delays the start of treatment.
Muscle dysfunction also affects the larynx. In this case, even involuntary salivation may occur.
Parkinson's is diagnosed very rarely in young women, since in the vast majority of cases the disease affects people over 55-60 years of age.
At a young working age, symptoms will be noticed faster. But a diagnosis can only be made after an examination, which includes electromyography.
Only a doctor can make an accurate diagnosis of a patient, since the symptoms of the disease can be vague and characteristic of other pathological conditions, in addition to Parkinson’s disease.
Stages of development of Parkinson's disease
"1st stage"
Some disturbances in the movements of one of the hands. Nonspecific manifestations also occur: decreased sensitivity of smell, chronic fatigue, sleep disturbances and mood abnormalities. When nervous, tremors appear in the fingers. As the tremor progresses, it intensifies and tremor appears at rest.
"One and a half" or "intermediate stage"
Strong manifestations of signs of illness in one of the parts of the body or arm. Constant trembling, disappearing only in sleep. The quality of fine motor skills of the hands deteriorates, manifested in changes in handwriting. Stiffness in the neck and part of the upper back becomes noticeable, and the swinging movements of both arms when walking are limited.
"2nd stage"
Symptoms of deviations in the regulation of movements occur on both sides of the body. Trembling of the lower jaw and tongue is also possible. Disturbances in joint movement, noticeable changes in facial expressions and speech inhibition. Changes in sweating: skin is too oily or, conversely, too dry. Sometimes the patient has the ability to control involuntary movements. The patient can perform simple tasks and actions, but the speed of their execution slows down significantly.
"Zya stage"
Muscle stiffness (rigidity) and hypokinesia become much more noticeable. The gait changes noticeably, which has the appearance of a “puppet”, expressed in parallel feet and small steps. The facial expression takes on the appearance of a “mask”. Head shaking may appear as swaying movements (vertically or horizontally). The posture that often appears noticeably changes: half-bent legs, a semi-squat position of the pelvis, a hunched back with the head pressed and lowered forward, while the arms are slightly bent at the elbows and pressed against the body (the “beggar” pose). Characteristic movements in the joints are jerky. Deviations in speech develop - a person begins to fixate on the same words. The person is still able to take care of himself, but experiences enormous difficulties in doing so. It is difficult to fasten buttons and get your hands into the sleeves. Much more time is spent on simple hygiene procedures.
"Stage 4"
Postural instability begins to be noticeable - it is difficult for a person to balance when landing or getting out of bed (there is a high probability of falling forward). If you slightly push a patient who is standing at rest, he will move by inertia in the direction of the push until he hits an obstacle. There are falls that end in broken limbs. During sleep, changing the position of the body is especially difficult. The patient’s speech degrades – it becomes quieter and has a “blurred” character. Acute manifestations of depression, expressed in suicide attempts, are possible. There is a possibility of progression to dementia. Without outside help, a person can no longer cope with everyday worries and self-care activities.
"Stage 5"
This is the last stage of development of Parkinson's disease, and it is characterized by the development and intensification of all movement disorders. The person is no longer able to walk, sit or stand independently. Is not able to feed on his own - this happens not only due to trembling in the limbs and stiffness in the muscles, but also due to the inability to swallow food on his own. Loss of urinary control. His speech becomes extremely incomprehensible and the person begins to need constant care and help from others. Often these manifestations are accompanied by severe attacks of depression and dementia.
Dementia is a disease characterized by damage to cognitive functions to a much greater extent than occurs with aging. It manifests itself in the loss of the ability to learn and acquire new information with the loss of previously acquired knowledge.
Symptoms of Parkinson's disease
Symptoms of Parkinson's disease may not be noticeable in the early stages. First, the patient notices trembling or awkwardness in one arm or leg. General stiffness occurs and gait becomes difficult. The amplitude of tremor movements at the onset of the disease can change the degree of severity - intensify after emotional experiences, decrease after rest. Over time, there is limited mobility when moving the affected leg/arm. The back becomes more hunched. The stride length is shortened.
The first signs of Parkinson's disease in women and men also include:
- pain in the limbs, back;
- feeling of tightness in the calf muscle/shoulder area;
- muscle cramps;
- insomnia;
- increased fatigue;
- depression.
In addition, some autonomic disorders may occur: impotence, constipation, urination and sweating disorders, orthostatic hypotension, seborrheic dermatitis.
The main signs of Parkinson's disease with an already developed clinical picture are:
- Rigidity. Muscle tone increases, and increased resistance to passive movements appears. It can be intermittent or monotonous (in the first case they talk about the “gear wheel” phenomenon, in the second – about the “wax doll” phenomenon).
- Hypokinesia. Initiation of voluntary movements becomes difficult, the patient becomes slow. He cannot generate muscle effort that is adequate in pace and strength. Symptoms of this condition include:
- quiet speech (hypophonia);
- poor facial expression reactions (hypomimia);
— very rare blinking;
- small handwriting (micrography);
- shortening of step length (brachybasia);
- difficulty getting up from a chair, walking, turning to the sides;
- decreased swinging of arms during movement (acheirokinesis).
- Postural instability. Normally, postural reflexes help maintain balance while walking and standing in place. If they weaken, a person cannot resist standing up, walking, or making turns. Because of this, he often falls. In an effort to get up and walk, he changes the direction of his movement. From the outside it looks like marking time in one place.
- Rest tremor. Limbs and head begin to tremble. Hand movements resemble “counting coins.” The pathology can be unilateral or asymmetric. It is observed in 80-85% of cases.
In addition to the symptoms mentioned above, Parkinson's disease may cause:
- salivation;
- dementia;
- restless leg syndrome;
- dysphagia (difficulty swallowing);
- dysarthria (impaired pronunciation).
If you experience similar symptoms, consult your doctor
. It is easier to prevent a disease than to deal with the consequences.
Causes of Parkinson's disease
Doctors and scientists are unable to recognize and identify specific root causes of the development of Parkinson's disease, however, there are several facts that may provoke the progression of this disease:
- One of the reasons may be aging . Since with aging, the number of nerve connections and cells sharply decreases, which, in turn, leads to a decrease in the required amount of dopamine in parts of the brain (in the basal ganglia).
- Hereditary factor . The genetic predisposition has not yet been proven, but 20% of people with this disease have relatives with manifestations of parkinsonism.
- Environment . It can lead to toxic brain poisoning due to the presence of toxic compounds, poisonous substances, pesticides and heavy metals in the air, water or food, which can lead to the death of a large number of nerve cells and lead to illness.
- Use of medications . Antidepressants and other antipsychotic medications that alter the metabolism and production of dopamine in the central nervous system can cause side effects very similar to the symptoms of parkinsonism.
- Diseases and brain injury . Concussions, various head contusions, viral or bacterial encephalitis - all this can lead to damage to parts of the basal ganglia and trigger the progression of Parkinson's disease.
- Lifestyle . Improper sleep patterns (lack of sleep), regular stress, unhealthy diet, lack of vitamins in the body and other factors can cause some pathologies.
- Other diseases . For example, atherosclerosis, various malignant tumors in the brain, and disorders of the endocrine gland can also provoke complications leading to Parkinson's disease.
Parkinsonism and its main nosological forms
Parkinson's disease (PD) is a chronic, steadily progressive disease of the central nervous system with degeneration of nigrostriatal neurons and dysfunction of the basal ganglia. It is one of the most common neurodegenerative diseases, which ranks third among the causes of death after cardiovascular diseases and cancer.
Parkinsonism has been known for a long time; the first reports of the treatment of similar disorders were made 1000-2500 BC.
The first clinical description belongs to the English physician James Parkinson, who published “An Essay on the Shaking Palsy” in 1817.
A detailed clinical analysis of the pathology complex was made in 1879 by the famous French neurologist Jean Martin Charcot.
Currently, the classification of parkinsonism includes: I. Parkinson's disease (it accounts for about 70-80% of all registered cases). II. Secondary (symptomatic) parkinsonism (about 15%) includes the following options: drug, toxic, post-hypoxic, encephalitic, traumatic, with volumetric processes, with hydrocephalus, vascular. III. Parkinsonism in various degenerative diseases with damage to the extrapyramidal system (“Parkinsonism-plus”, about 10%): multisystem atrophies (striatonigral degeneration, olivopontocerebellar degeneration), progressive supranuclear palsy (Steele-Richardson-Olszewski disease), corticobasal degeneration, dementia with Lewy bodies , parkinsonism-ALS-dementia, Wilson-Konovalov's disease, Huntington's disease (juvenile variant of Westphal), Fahr's disease (idiopathic calcification of the basal ganglia), Alzheimer's disease, others.
The main nosological form of parkinsonism is Parkinson's disease.
The worldwide prevalence of PD is approximately 1%.
The etiology of PD is unknown. Its pathogenesis is based on the degeneration of so-called dopaminergic neurons. PD is predominantly sporadic, but if close relatives have PD, the risk of developing it increases.
Clinical manifestations of PD occur when the amount of dopamine in the caudate nucleus and putamen decreases by at least 70%. Symptoms of PD develop gradually, initially affecting the limbs on one side. The clinical picture of PD is characterized by a combination of hypokinesia, rigidity, resting tremor, and postural disturbances.
Hypokinesia is manifested by a decrease in motor activity, slowness of movements, and a decrease in the amplitude of actions.
Rest tremor classically begins in the distal upper or lower extremity and resembles hand movements “counting coins or rolling pills.” Subsequently, the tremor involves the homolateral limb, lower jaw, and opposite limbs. Sometimes there is postural tremors of the hands.
Rigidity in PD is manifested by a plastic increase in muscle tone, often with a “cogwheel” phenomenon that increases during the study. Postural instability, which occurs in advanced stages of PD, is characterized by instability when turning, staggering when walking, and falls. In the future, patients are forced to use support devices.
In addition to motor disorders, non-motor manifestations develop in PD: neuropsychiatric disorders; sleep disorders; autonomic disorders; sensory disorders.
Depending on the predominance of a particular symptom in the clinical picture of PD, it is customary to distinguish the following clinical forms of the disease: trembling, akinetic, as well as mixed forms - akinetic-rigid and rigid-tremulous.
There are five degrees of severity of PD (stages of the disease according to Hoehn and Yahr): stage 1 - unilateral symptoms of parkinsonism; Stage 2 - bilateral symptoms of parkinsonism without postural disturbances; Stage 3 - moderate postural instability occurs; Stage 4 - significant limitation of motor activity, falls, but the ability to move independently is still retained; Stage 5 - the patient is bedridden or wheelchair-bound.
In the later stages of PD, the clinical picture changes; additional motor (motor fluctuations, drug-induced dyskinesias, walking disorders, falls, freezing and akinetic crises) and non-motor (vegetative, cognitive, neuropsychiatric) syndromes appear.
Patients may experience long periods of decompensation - from several days to several weeks, as well as akinetic crises - severe episodes of akinesia, accompanied by dysphagia, autonomic disorders, hyperthermia, oliguria, and confusion. The reasons for this may be: violation of the regimen for taking antiparkinsonian drugs, their complete o); taking drugs that block DA receptors (primarily antipsychotics); exacerbation of concomitant somatic diseases, stress; operations, injuries, dehydration of the body.
PD can be diagnosed with certainty only through autopsy. Clinical diagnosis of parkinsonism syndrome requires the presence of hypokinesia and at least one of the three main symptoms of parkinsonism: resting tremor, rigidity and postural instability.
An MRI of the brain is mandatory if the patient has parkinsonism syndrome. This study is primarily necessary to differentiate idiopathic Parkinson's disease and secondary parkinsonism, as well as “parkinsonism-plus”.
The main directions of treatment for PD are: 1. Pharmacotherapy. 2. Medical and social rehabilitation. 3. Therapeutic physical education (PT). 4. Neurosurgical treatment.
Pharmacotherapy for PD is aimed at normalizing the biochemical imbalance and requires constant use of medications, since when treatment is stopped, the symptoms of PD return to their original level.
At an early stage, treatment of PD consists of prescribing monotherapy followed by a transition to combination treatment.
In the early stages of the disease, it is generally accepted to prescribe DA receptor agonists and MAO-B inhibitors in the form of monotherapy or combination to patients under the age of 70 years.
In patients over 70 years of age, when the patient's life expectancy is shorter, and there are cognitive impairments, therapy can be started immediately with DOPA-containing drugs in the minimum effective dose, which is adjusted gradually.
Anticholinergics (Cyclodol, Akineton) are prescribed mainly at the early stage of PD - as monotherapy or in combination with other antiparkinsonian drugs; they predominantly affect resting tremor.
Currently, they are prescribed only to young patients with severe rest tremor and intact cognitive functions. The high incidence of side effects and low effectiveness compared to other groups significantly limit their use. Amantadine preparations (Midantan, PC-Merz).
Amantadines can be prescribed both at the initial stage as monotherapy and in combination with other antiparkinsonian drugs in the later stages of PD. The drugs are also effective in reducing the severity of dyskinesia caused by taking levodopa. The infusion form of amantadine sulfate (PC-Merz) is used in the treatment of decompensations and akinetic crises in PD.
Dopamine receptor agonists have the ability to directly stimulate DA receptors in the brain. Non-ergoline DA receptor agonists (Pronoran, Mirapex, Requip Modutab, Newpro) are widely used at all stages of PD. In addition to controlling movement disorders, they showed an antidepressant effect, which is very important, since the frequency of depressive syndrome in PD is quite high.
ADAR monotherapy in the early stages of the disease makes it possible to delay the prescription of levodopa drugs, as well as the development of motor fluctuations and drug-induced dyskinesias.
MAO type B inhibitors (Rasagiline). The administration of drugs in this group leads to an increase in the amount of dopamine in neurons. They are also believed to have a neuroprotective effect. They can be prescribed in the early stages as monotherapy, as well as in combination with levodopa.
COMT inhibitors. COMT inhibitors increase the bioavailability of levodopa by reducing the level of its inactive metabolites.
Peripherally acting COMT inhibitors do not cross the BBB and interfere with methylation of levodopa in the gastrointestinal tract and bloodstream. Thanks to this, they maintain the concentration of levodopa at a certain level. These drugs include entacapone.
The combination of entacapone with levodopa drugs can reduce the daily dose of DOPA-containing drug by 15–30%.
It is prescribed only in combination with levodopa drugs (Stalevo), since when prescribed as monotherapy it does not have an independent antiparkinsonian effect.
Levodopa preparations (Madopar, Nacom, Tremonorm, Tidomet-forte, Duellin, Sindopa). Dopamine does not cross the BBB, so a metabolic precursor of dopamine, levodopa, has been proposed as a drug, which crosses the BBB and is metabolized into dopamine in the brain. Today, levodopa drugs are the most effective drugs, the “gold standard”, used for the treatment of PD. However, they do not stop the progression of PD. Moreover, after an average of 5 years of using DOPA-containing drugs in patients with PD, their effect decreases, motor fluctuations and drug-induced dyskinesias appear.
The timing of treatment with levodopa depends on the severity and rate of progression of the disease, the professional activity of the patient, and family and household status. In general, it is necessary to prescribe drugs from this group when there are severe motor disorders that cannot be relieved by other antiparkinsonian drugs.
Neurosurgical treatment.
A decrease in the effectiveness of pharmacotherapy, the appearance of motor fluctuations and drug-induced dyskinesias are indications for the use of neurosurgical treatment, which over the past two decades has firmly taken its place in the algorithm for the management of patients with PD. Currently, three types of neurosurgical interventions are used for PD: stereotactic destructive methods (ventrolateral thalamotomy, pallidotomy, subthalamotomy and their combination), stimulation methods (implantation of electrodes into subcortical structures followed by chronic electrical stimulation) and intracerebral transplantation of dopaminergic neurons of the mesencephalon of the human embryo, effectiveness which continues to be studied.
The most modern method of surgical treatment of PD is deep electrical stimulation of the brain. The DBS procedure consists of implanting electrodes with 4 contacts into target areas within the subcortical formations of the brain; The electrodes are connected to a stimulator implanted under the skin, which delivers high-frequency electrical impulses to the stimulated nucleus.
Medical and social rehabilitation.
The high degree of disability with steadily progressing PD, the socio-economic losses suffered by society necessitate the creation of a system of medical and social rehabilitation, which should include dispensary observation of patients; creating schools for patients and their relatives, conducting training programs and psychotherapeutic classes, creating public organizations and support groups. Exercise therapy is of great importance, which can be selected individually depending on the severity of the disease in a particular patient, exercise therapy classes in groups, dance therapy, as well as occupational therapy and physiotherapy.
Literature: 1. Shtok V.N., Diagnosis and treatment of extrapyramidal disorders. - M., 2000. - P. 138. 2. Shtok V. N., Fedorova N. V. Treatment of parkinsonism. - M., 1997. - 194 p. 3. Yakhno N. N. Modern approaches to drug treatment of Parkinson’s disease // Clinical pharmacology and therapy. - 1994. - No. 3-4. - P. 92 - 97. 4. Levin O.S., Fedorova N.V., Parkinson’s disease. - M., - 2012. 5. N.V. Fedorova, I.P. Chigir, Parkinson's disease - Attending physician - 2005. -№8.- p.26-28.
How is Parkinson's disease treated?
- In the early stages of Parkinson's disease, it is treated with medications, introducing substances that are lacking into the body. The main target of drug (chemical) therapy is the “substantia nigra”. When using this method of treatment, almost all patients experience a noticeable reduction in symptoms and they have a lost opportunity to live a normal life.
- But there are cases when patients do not improve, even after taking medications for a long time and increasing their dosages. In such cases, brain surgery is used to implant a stimulator into the brain.
This operation takes the form of high-frequency stimulation of the basal ganglia with electric current through an electrode connected to an electrical stimulator:
- When using local anesthesia, two electrodes are sequentially introduced into the patient’s brain (along a path determined in advance by a computer), producing deep stimulation of parts of the brain.
- Under anesthesia, an electrical stimulator connected to electrodes is implanted into the chest area under the skin.
Drugs used for treatment:
"Amantadine" or "Midantan". These are the drugs used to start the treatment of Parkinson's disease. This medication stimulates the release of dopamine, helps reduce its reuptake by blocking glutamate receptors, protects the “substantia nigra,” and also has other positive properties. Amantadine significantly reduces the manifestations of hypokinesia and rigidity (stiffness and limited movement), however, it almost does not reduce tremor and trembling. These medications are well tolerated and have almost no side effects.
Rotigotine or Newpro. It is an agonist of the dopamine receptor group. Available in the form of a patch that is applied to the skin. This patch is a transdermal therapeutic system with dimensions of 10-40 cm², used once a day. Such medications are sold exclusively by prescription and are used for independent (without combination with other drugs) treatment of Parkinson's disease in the early stages.
The use of this form of drugs has significant advantages: the dosage is smaller, but more effective, and the side effects are less pronounced.
"Leftfall." It has long been considered one of the best medical drugs for the treatment of Parkinsonism. This compound is a chemical precursor to dopamine. But it is worth remembering that this substance has a significant number of side effects, such as psychological disorders. It is prescribed, as a rule, in combination with “carbidopa” or “benserazide”. They lead to better absorption of “levodopa” and reach areas of the brain and help reduce side effects.
"Modopar". It is a combination drug containing both “leovdopa” and “benserazide”. Produced in various forms. "Madopar GSS" is produced in special capsules, the shell density of which is significantly less than that of gastric juice. This ensures that the substance enters the body slowly and evenly, because such a capsule dissolves in the stomach from 5 to 12 hours. “Dispersible Madopar” is also available, which has a liquid form, thanks to which it acts much faster. This option is more suitable for patients with limited swallowing function.
"Miralex". This drug is produced as tablets, which are used both as a stand-alone drug in the early stages of the disease, and as a combination therapy with levodopa in the later development of Parkinson's disease. Miralex has fewer side effects than non-selective agonists, but at the same time more than amantadine. Such side effects can manifest themselves as nausea, pressure surges, excessive drowsiness, changes in the balance of enzymes secreted by the liver, and swelling of the lower extremities. Hallucinations are also possible in patients diagnosed with dementia.
"MAO inhibitors." They significantly slow down the oxidation of dopamine, located in the “striatum” of the brain, due to this its concentration in synapses increases. The most common use in the treatment of the disease is Selegiline. In the first stages of Parkinson's disease, Selegiline is used as an independent therapy (without the use of other combination drugs). Many patients report significant improvements when using these products. Undesirable effects from the use of Selegiline are rare and mild.
Treatment with Selegiline can delay the prescription of lepodopa for a period of 9 to 12 months. In the last stages of the disease, Selegiline is used as an addition to Levodopa, which allows the latter to increase its effectiveness by a third.
"Mydocalm." This drug greatly reduces the abnormally large tone of muscle tissue. This property is used in Parkinson's disease as an auxiliary. "Mydocalm" is available in tablets, for oral use and ampoules, for intravenous and intramuscular use.
"B vitamins." This group of vitamins is often used to treat diseases of the central nervous system. In order for L-Dopa to be safely converted into dopamine, nicotinic acid and vitamin B6 are needed. Also, “Thiamin” (vitamin “B1”) is used to increase the content of dopamine in parts of the brain.
Diet for Parkinson's disease
If you have Parkinson's disease, you need to eat in small portions 5-6 times a day. The bulk of hearty meals should be consumed before lunch. It is advisable to leave easily digestible food for the evening.
If you suffer from constant bouts of nausea, it is recommended to eat very slowly. Drink only half an hour after finishing the meal.
It is important that the diet for Parkinson's disease is well balanced. If you have no appetite, you should still eat.
To avoid constipation, you need to enrich your diet with fiber, grains and dairy products.