The vestibulocochlear nerve (VCN) is part of the system of the organ of the same name, which is responsible for the functioning of the hearing aid. This is a fiber of special sensitivity, which includes several roots. The vestibular one is responsible for impulses from the static apparatus, and the cochlear one conducts signals from the organ spiral to the labyrinth. In medicine, there are several methods for testing the vestibulocochlear nerve in order to identify its pathologies. After all, they affect many unpleasant symptoms: from dizziness to severe weakness and headaches.
Anatomy and topography of the nerve ending
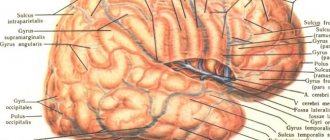
Anatomy of the vestibulocochlear nerve
Topography divides the fiber into two parts. The first is the cochlear part of the vestibular-cochlear nerve fiber, which is also called the vestibular. It integrates with afferent endings and transmits information from them. They are embedded in the semicircular channels of the elliptical and spherical sac. The second part is the cochlea, which transmits impulses from the spiral organ to the brain.
The anatomy of the parts of the vestibulocochlear nerve is as follows:
- The vestibule. The node of the same name is located here, deep in the auditory canal. It is also divided into 2 parts: the upper, directed to the receptive fields, and the lower, forming the spherical-saccular nerve. The ampullary nerve, which arises from the vestibulocochlear nerve, also originates here. The central roots of the cells of this node form the vestibular part, and in the cochlear zone they connect to the auditory canal. Inside, the nerve goes along with the intermediate endings and the branch of the facial nerve, and then diverges into the cranial cavity through the auditory canal. At the cerebellopontine angle the ending passes into the brain stem. The nuclei of the vestibular part of the vestibulocochlear nerve are also formed here. The vestibular part in the region of the vestibular field of the rhomboid fossa ends at the top in the ankylosing spondylitis nucleus, in the middle – in the Schwalbe nucleus, and at the back – in the Deiters nucleus.
- Cochlear zone. This part originates from the spiral ganglion formed by the neurons of the auditory pathway. Then it passes into the spiral canal of the cochlea rod. The peripheral roots end in the spiral organ. And the central ones run through the rod and the opening of the spiral path in the ear canal. The cochlear part of the apparatus is formed there. Then, together with the vestibular nerve ending, it passes into the cranial cavity through the auditory opening and goes to the brain stem. In the cerebellopontine part it enters the trunk and ends in the ventral and dorsal nuclei.
Topographically, the features of PUN do not differ from the characteristics of other sensitive fibers passing in this zone.
Physiological basis of maintaining balance
Return to section:
Dizziness Treatment Center
The cause of dizziness in most cases is a violation of the coordinated activity of various sensory systems - vestibular, visual, proprioceptive (information about the position of the body in space, received from receptors located mainly in muscles and tendons). In addition, an important and sometimes dominant cause of dizziness is dysfunction of the central structures involved in maintaining the balance of the body, mainly the cerebellar nuclei.
Vestibular system
The vestibular system consists of:
- maze,
- vestibular part of the vestibulocochlear nerve,
- vestibular nuclei in the brain stem, as well as their connections with other parts of the central nervous system (CNS).
The correct operation of the vestibular system allows a person to clearly navigate in three-dimensional space, namely:
- perceive the position of the body relative to the gravity vector (static component);
- feel the direction and speed of movement of the body during its angular and linear movements (dynamic component).
The labyrinth is located in the petrous part of the temporal bone and includes:
- otolithic apparatus, which is represented by two communicating chambers (sacculus and utriculus);
- a system of three semicircular canals located in mutually perpendicular planes.
Structure of the labyrinth
In each chamber of the otolithic apparatus and in each semicircular canal there is a cluster of receptor cells - the macula, which is covered with a gelatinous mass - the cupula. In the otolithic apparatus, the cupula covers the hair cells like a cushion and contains deposits of calcite crystals (otoliths), which give the cupula additional weight.
Otolith apparatus
In the semicircular canals, the gelatinous mass does not contain otoliths and completely covers the lumen of the canal.
The receptors of the vestibular system are represented by hair cells, which bear on the apical surface from 60 to 80 thin processes of cytoplasm (stereocilia) and one cilium (kinocilia).
Perception of body position relative to gravity
When the head is vertical, the macula of the utriculus is located horizontally. When the head tilts to the side, the gelatinous membrane, weighted by otoliths, slides toward the tilt under the influence of gravity. This sliding causes the stereocilia of the hair cells to bend. The tilt of the stereocils is accompanied (depending on the direction) by an increase or decrease in the frequency of nerve impulses in the sensory neurons of the vestibular ganglion. The macula of the sacculus is positioned vertically and acts in the same way.
Perception of body position relative to gravity
Perception of linear accelerations
With sharp linear acceleration of the body, the cupula of the sacculus or utriculus, due to inertial forces, shifts in the direction opposite to the direction of movement, which also leads to a change in the electrical activity of the receptors.
Perception of angular acceleration
The three semicircular canals are located in three different planes. Each of the three channels acts as a closed tube filled with lymph. In the expanded part of the canal, its inner wall is lined with hair cells, and the cupula located above them completely covers the lumen of the canal. When the head turns, the semicircular canals turn with it, and the endolymph, due to its inertia, at the first moment remains in place. As a result, a pressure difference arises on both sides of the cupula, and it bends in the direction opposite to the movement. This causes deformation of the stereocilia and a subsequent change in neuronal activity.
Perception of angular acceleration
When the head rotates only in the horizontal, sagittal or frontal plane, the receptors of one of the corresponding channels are activated. During complex head rotation, the receptors of all three channels are activated. Information from them enters the brain and, based on its convergence and analysis, the true pattern of head movement is modulated.
Central division of the vestibular system
The axons of sensory neurons, the bodies of which are located in the vestibular ganglion, follow into the medulla oblongata and end in four paired vestibular nuclei. The impulses from the receptors arriving at these nuclei provide accurate information about the position in space of only the head (but not the entire body!), since it can be tilted or rotated relative to the body. To perceive the position of the body in space, it is also necessary to take into account the angle of inclination and rotation of the head relative to the body, therefore the vestibular nuclei receive additional stimuli from the proprioceptors of the neck muscles.
Nuclei of the vestibular nerve and their connections
Further from the vestibular nuclei, afferent impulses are sent to the neurons of the specific nuclei of the thalamus, and the processes of the latter reach the postcentral gyrus of the cerebral cortex
Proprioceptive system
Thanks to proprioception, we feel the position of the limbs, movement and the degree of muscle tension in them. This gives a person a feeling of “support”, i.e. awareness that the feet rest on some surface, supporting the weight of the body. The receptor apparatus of proprioceptive sensitivity is located in muscles, tendons, fascia, joint capsules, and also in the skin.
It should be noted that deep sensitivity receptors, located not only in the limbs, but also in the structures of the neck, mainly in the deep muscles, play an important role in maintaining body balance. The information received by the brain from these receptors is necessary for spatial orientation of a person, maintaining his posture, as well as coordinating the movement of the head and torso.
Visual system
Effective maintenance of balance requires precise control by the visual system (in accordance with the feedback principle). At the same time, control over the movements of the muscles of the eyeball is an extremely complex process. There are 3 main gaze control systems:
- System of saccadic movements of the eyeballs;
- System of smooth (following) movements of the eyeballs;
- Vestibulo-ocular system.
Within the brain, these systems are controlled by specific anatomical regions that are largely isolated and provide two main functions:
- fix the object of consideration in the periphery of the visual area, turning your eyes towards it;
- hold the image of the object being viewed stable on the retinal fovea.
System of saccadic movements of the eyeballs
When an object of interest appears in the periphery of the visual area, the eyeballs rapidly turn towards it, so that the image of the object is projected onto the retina in the macula area. The same motor response of the eyeballs can be triggered by a sudden sound or painful stimulus. This rapid eye movement is called saccadic, from the French word meaning the sudden movement of a sailboat in the wind, or the jerking of a horse's head when the reins are pulled. In general, the system of saccadic movements of the eyeballs ensures that a visual target is detected and brought to the most sensitive part of the retina. Saccades occur, for example, in the process of reading, with a person's eyes usually making several saccadic movements on each line. In addition, they appear when a person examines an object (painting, sculpture, etc.), but in this case, saccades are made in different directions (up, down, to the sides and at an angle) sequentially from one point of the object to another.
Classic image describing the saccadic movement of the eyeballs when viewing an object
System of smooth (tracking) movements of the eyeballs
When an object of view moves, the saccadic system may initially fixate on it, but soon loses it as the image moves out of the macula (reticular glide). Smooth (tracking) eye movements are necessary for long-term fixation of a moving object and tracking it. Once a visual target is selected, the system operates outside of volitional control.
Schematic representation of the functioning of the system of smooth (tracking) eye movements
Vestibulo-ocular system
While the tracking system of the eyeballs fixes the image of a moving object of viewing on the macula, there is another system that allows you to stabilize the image of a stationary object of viewing on the retina during head movement. This is the main function of the vestibulo-ocular system. Thanks to its presence, a person does not have problems clearly viewing a distant object while driving on an uneven road or walking. In the case when for some reason the vestibulo-ocular system does not work, a phenomenon called “oscillopsia” occurs - “twitching” of the visual image when moving.
Cerebellum
The main function of the cerebellum is to receive information about the position of the body in space from all sensory organs and, on its basis, to regulate muscle tone and movements to maintain balance and perform precise actions.
Patients with cerebellar damage are characterized by astasia-abasia - a violation of the ability to maintain body balance when standing and walking. Patients walk with their legs spread wide apart – the so-called trunk ataxia (“drunk gait”).
Walking on heels and toes is impossible. Ataxia in this case develops due to the inability of the brain to coordinate muscle activity in the process of overcoming gravity. Oculomotor disorders are also detected. They are manifested by a violation of gaze fixation on stationary or moving objects, resulting in jerky eye movements during tracking. Vertical nystagmus, beating up or down, is also characteristic.
Vertical nystagmus with cerebellar damage.
← Back
Functions of the nerve ending
There are several functions of the vestibulocochlear nerve. Violation of even a small segment in the structure of the ending can lead to significant changes in a person’s well-being:
- Auditory function. The human hearing system is a very complex organ consisting of the middle, inner and outer ears. The vestibulocochlear nerve is responsible for the innervation of the internal, most complex structure. First, the sound hits the membrane, and then is transmitted by its vibrations to the hammer. From there it moves to the stapes and anvil, combined with each other. Then it is transmitted to the oval window in front of the labyrinth. Intra-auricular fluid ensures prolongation of vibrational waves, which facilitates transmission through the lymphatic layers. The basilar plate receives sound from the spiral ganglion of the inner ear. And the processes of the nerve endings entering the node go through the opening of the ear canal and penetrate to the nerve. The nerve then sends a signal to the nucleus of the brain stem. This is how the brain receives a signal about incoming sound.
- Balance option. The hearing aid is closely related to the vestibular one. If disturbances occur in it, they also affect the coordination of movements. You may even experience symptoms such as nausea and fainting. The vestibulocochlear nerve provides innervation to important parts of the vestibular system. It allows the nervous system to analyze the position of the head and adjust the tone of the muscles of the whole body. And the organ responsible for balance is located right in the labyrinth of the middle ear and consists of 3 channels. They contain sensitive hairs. These hairs are equipped with neuronal processes that go to the vestibular canal of the bottom of the temporal bone. Further, passing into the medulla, the nerve enters the vestibular nuclei. They are responsible for the body's friendly reactions.
Any pathology of the vestibulocochlear nerve, disruption of its circuit, formation of tumors and rupture of innervation lead to problems with hearing and coordination. And damage to the vestibular apparatus can lead to other diseases.
Anatomy
The red nucleus (nucleus ruber) is a large collection of neurons along almost the entire length of the midbrain.
Its color is explained by the large number of capillaries or the presence of iron-containing pigment in neurons. The structure is divided into an anterior small cell (parvocellular) and a posterior (magnocellular) large cell part.
| Part of the red core | Parvocellular nucleus ruber | Magnocellular nucleus ruber |
| Neurotransmitters | GABA, glutamate | Glutamate |
| Meaning | Connected to the cerebellum Gives rise to the red nuclear olivary tract | Gives rise to the rubrospinal tract |
| Evolution | Associated with motor learning processes, developed in humans | Ancient motor center |
There are several pathways connecting the structure with other parts of the brain. The main ones:
- The corticorubral tract (corticorubral tract, tractus corticorubralis) stretches from the cortex to the nucleus. It runs parallel to the corticospinal tract of the pyramidal system. This shows parallels between the pyramidal and extrapyramidal systems.
- The cerebellorubrospinalis tract (tractus cerebellorubrospinalis) follows the motor neurons of the spinal cord, but before that it passes through the red nucleus. Connections with the cerebellum provide correction of movements.
- The neurons of the magnocellular part give rise to the rubrospinal tract (red nuclear spinal tract, tractus rubrospinalis, rubrospinal tract). Its fibers immediately pass to the opposite side of the midbrain and then descend to the motor neurons of the spinal cord. In humans, the rubrospinal tract largely determines the movements of the limbs.
- Rubroolivary tract.
The structure also receives signals from the basal ganglia and sends impulses to the cortex.
The function of the red nuclei is to integrate information from the cortex and cerebellum and control underlying structures.
Red cores provide:
- Exit of the extrapyramidal system to the spinal cord.
- Determination of the tone of all skeletal muscles of the body.
- Coordination of posture together with the cerebellum.
- Regulation of unconscious automatic movements, such as changing body position.
Possible diseases
Symptoms of damage to the vestibular-cochlear nerve
Damage to the vestibular-cochlear nerve is accompanied by several symptoms. They are closely related to the part in which the violation is localized:
- If the vestibule is damaged, a person experiences dizziness, problems with stability, nausea, and vomiting. The pulse and breathing rhythm change, and blood pressure fluctuations are possible.
- If the cochlear part is damaged, the patient experiences severe tinnitus and hearing loss. Complete deafness is possible.
If both parts are damaged, all symptoms appear simultaneously and can be either severe or mild.
Causes of nerve damage
The most common diseases leading to pathologies of PUN include:
- Infections and viruses. Symptoms can be caused by influenza, colds, as well as measles, scarlet fever, syphilis, mumps and tuberculosis.
- Diseases of the heart and blood vessels. Strokes, heart attacks, atherosclerosis and myocarditis can also cause poor health.
- Intoxication. Symptoms appear when treated with antibiotics and other medications.
There are other diseases that are specific only to the ears, such as labyrinthitis. With this pathology, the inner ear is affected.
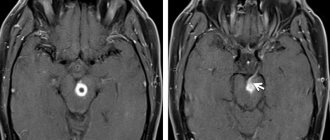
Rarely occurs acoustic neuroma involving PUN. It develops very slowly and provokes the gradual onset of all symptoms. Meniere's syndrome is also possible. It is associated with a disease of the same name, in which the production and outflow of fluid in the inner ear changes. From the side of the affected nerve, noise in the ear and a feeling of fullness appear. The person may suffer from attacks of dizziness and hearing loss.
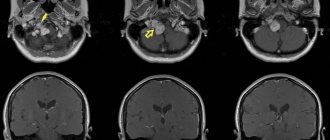
To identify the exact cause, a full diagnosis is required. The patient is prescribed electroencephalography and examination by an ENT specialist or a neurologist. A CT and MRI of the ear area may be required.
Features of the treatment of pathologies
Methods for treating pathology of the vestibulocochlear nerve
Some diseases of this structure require only surgical intervention. Neuroma is considered especially dangerous. It is removed during surgery, since as it develops, especially in the brain part of the PUN, it leads to pressure on the vascular and respiratory centers. After removal, rehabilitation therapy is carried out.
For other disorders, symptomatic treatment is used:
- the patient is provided with complete rest during attacks of dizziness and hearing loss;
- prescribe B vitamins to improve well-being and fiber nutrition;
- take medications to normalize fluid levels in the inner ear;
- perform light gymnastics for the cervical spine;
- massage the head and area;
- use means to improve microcirculation.
Treatment is carried out by a neurologist in combination with the help of an otolaryngologist, neurosurgeon and other specialists.