Brain structure
Everyone knows that if the brain stops functioning, then a person does not react to any external factors, does not show any activity, and turns into a “vegetable.” The structure of the brain is symmetrical and consists of the right and left hemispheres.
Disputes between scientists do not subside, but some facts have been proven and approved.
Important facts:
- The human brain consists of 25 billion neurons.
- The adult brain makes up about 2% of body weight.
- The organ consists of three membranes: hard, soft, arachnoid. The shells perform the main – protective function.
It is generally accepted that the left hemisphere is responsible for all mental processes, and the right hemisphere for the perception of the outside world. Roughly speaking, the left is the logical hemisphere, and the right is the creative hemisphere.
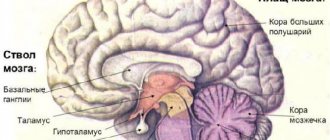
From an anatomical point of view, the brain consists of the following parts:
- Medulla. Responsible for vegetative functions.
- Midbrain. Controls reflexes to external stimuli.
- Hindbrain. Responsible for coordination of movements.
- Diencephalon. Includes sensory centers (hunger, thirst, satiety, sleep regulation).
- Forebrain. The largest part, which is covered with grooves (convolutions). Provides better brain function.
Anatomical and physiological mechanisms of speech
Knowledge of the anatomical and physiological mechanisms of speech, i.e. structure and functional organization of speech activity, allows us to imagine the complex mechanism of speech. The speech act is carried out by a complex system of organs, in which the main, leading role belongs to the activity of the brain.
The structure of the speech apparatus.
The speech apparatus consists of two closely interconnected parts: the central (regulating) speech apparatus and the peripheral (performing) speech apparatus.
1. The central speech apparatus is located in the brain. It consists of: - cerebral cortex (mainly the left hemisphere) - subcortical nodes - pathways - nuclei of the brainstem (primarily the medulla oblongata) - nerves going to the respiratory, vocal and articulatory muscles.
What is the function of the central speech apparatus and its departments??
Speech, like other manifestations of higher nervous activity, develops at the basis of reflexes. Speech reflexes are associated with the activity of various parts of the brain. However, some parts of the cerebral cortex are of primary importance in the formation of speech. These are the frontal, temporal, parietal and occipital lobes, predominantly of the left hemisphere of the brain (in left-handers, the right).
— The frontal gyri (inferior) are the motor area and are involved in the formation of one’s own oral speech (Broca’s area).
— The temporal gyri (superior) are the speech-auditory area where sound stimuli arrive (Wernicke's center). Thanks to this, the process of perceiving someone else’s speech is carried out.
The parietal lobe of the cerebral cortex is important for understanding speech .
— The occipital lobe is a visual area and ensures the assimilation of written speech (the perception of letter images when reading and writing).
— The subcortical nuclei control the rhythm, tempo and expressiveness of speech.
— The pathways connect the cerebral cortex with the muscles that regulate the activity of the speech apparatus - centrifugal (motor) nerve pathways . The centrifugal pathway begins in the cerebral cortex in Broca's center.
From the periphery to the center, i.e. from the area of the speech organs to the cerebral cortex, there are centripetal pathways . The centripetal pathway begins in the proprioceptors and baroreceptors.
Proprioceptors are found inside muscles, tendons and on the articular surfaces of moving organs. Proprioceptors are excited by muscle contractions. Thanks to proprioceptors, all our muscle activity is controlled.
Baroreceptors are excited by changes in pressure on them and are located in the pharynx. When we speak, proprio- and baroreceptors are irritated, which follows a centripetal path to the cerebral cortex.
The centripetal path plays the role of a general regulator of all activities of the speech organs.
The cranial nerves originate in the nuclei of the brainstem All organs of the peripheral speech apparatus are innervated (innervation is the provision of any organ or tissue with nerve fibers, cells) by cranial nerves . The main ones are: trigeminal, facial, glossopharyngeal, vagus, accessory and sublingual.
— The trigeminal nerve innervates the muscles that move the lower jaw;
- Facial nerve - facial muscles, including muscles that move the lips, puff out and retract the cheeks;
- Glossopharyngeal and vagus nerves - muscles of the larynx and vocal folds, pharynx and soft palate. In addition, the glossopharyngeal nerve is the sensory nerve of the tongue, and the vagus nerve innervates the muscles of the respiratory and cardiac organs.
— The accessory nerve innervates the muscles of the neck, and the hypoglossal nerve supplies the muscles of the tongue with motor nerves and gives it the possibility of a variety of movements.
Through this system of cranial nerves, nerve impulses are transmitted from the central speech apparatus to the peripheral one. Nerve impulses move the speech organs.
But this path from the central speech apparatus to the peripheral one constitutes only one part of the speech mechanism. Another part of it is feedback - from the periphery to the center.
2. The peripheral speech apparatus consists of three sections: 1. Respiratory 2. Vocal 3. Articulatory (sound-producing)
The respiratory section includes the chest with lungs, bronchi and trachea .
Producing speech is closely related to breathing. Speech is formed during the exhalation phase. During the process of exhalation, the air stream simultaneously performs voice-forming and articulatory functions (in addition to another, main one - gas exchange). Breathing during speech is significantly different from usual when a person is silent. Exhalation is much longer than inhalation (while outside of speech, the duration of inhalation is approximately the same). In addition, at the time of speech, the number of respiratory movements is half as much as during normal (without speech) breathing.
It is clear that for a longer exhalation a larger supply of air is needed. Therefore, at the moment of speaking, the volume of inhaled and exhaled air increases significantly (about 3 times). The inhalation during speech becomes shorter and deeper. Another feature of speech breathing is that exhalation at the moment of speech is carried out with the active participation of the exhaled muscles (the abdominal wall and internal intercostal muscles). This ensures its greatest duration and depth, and in addition, increases the pressure of the air stream, without which sonorous speech is impossible.
The vocal section consists of the larynx with the vocal folds located in it. The larynx is a wide, short tube consisting of cartilage and soft tissue. It is located in the front of the neck and can be felt through the skin from the front and sides, especially in thin people.
From above the larynx passes into the pharynx . From below it passes into the trachea . At the border of the larynx and pharynx is the epiglottis . It consists of cartilage tissue shaped like a tongue or petal. Its front surface faces the tongue, and its back surface faces the larynx. The epiglottis serves as a valve: descending during the swallowing movement, it closes the entrance to the larynx and protects its cavity from food and saliva.
In men, the larynx is larger, and the vocal folds are longer and thicker than in women. The length of the vocal folds in women is on average 18-20 mm, in men it ranges from 20 to 24 mm.
How is voice formation or phonation accomplished?
The mechanism of voice formation is as follows. During phonation, the vocal folds are in a closed state (Figure 2). A stream of exhaled air, breaking through the closed vocal folds, somewhat pushes them apart. Due to their elasticity, as well as under the action of the laryngeal muscles, which narrow the glottis, the vocal folds return to their original state, i.e. middle position, so that as a result of the continued pressure of the exhaled air stream, it moves apart again, etc. Closing and opening continues until the pressure of the voice-forming exhalatory stream stops. Thus, during phonation, vibrations of the vocal folds occur. These vibrations occur in the transverse and not the longitudinal direction, i.e. the vocal folds move inward and outward, rather than upward and downward. As a result of vibrations of the vocal folds, the movement of the stream of exhaled air turns over the vocal folds into vibrations of air particles. These vibrations are transmitted to the environment and are perceived by us as vocal sounds. When whispering, the vocal folds do not close along their entire length: in the back part between them there remains a gap in the shape of a small equilateral triangle, through which the exhaled stream of air passes. The vocal folds do not vibrate, but the friction of the air stream against the edges of the small triangular slit causes noise, which we perceive as a whisper. The voice has strength, height, timbre. The strength of the voice depends mainly on the amplitude (span) of vibrations of the vocal folds, which is determined by the amount of air pressure, i.e. exhalation force. The resonator cavities of the extension pipe (pharynx, oral cavity, nasal cavity), which are sound amplifiers, have a significant influence on the strength of the voice. The size and shape of the resonator cavities, as well as the structural features of the larynx, affect the individual “color” of the voice, or timbre . It is thanks to timbre that we distinguish people by their voices. The pitch of the voice depends on the frequency of vibration of the vocal folds, and this in turn depends on the length, thickness and degree of tension. The longer the vocal folds, the thicker they are and the less tense they are, the lower the sound of the voice. In addition, the pitch of the voice depends on the pressure of the air stream on the vocal folds and the degree of their tension.
Articulation department . The main organs of articulation are: - tongue - lips - jaws (upper and lower) - hard palate - soft palate - alveoli Of these, the tongue, lips, soft palate and lower jaw are movable, the rest are fixed (Fig. 3).
The main organ of articulation is the tongue.
The tongue is a massive muscular organ. When the jaws are closed, it fills almost the entire oral cavity. The front part of the tongue is mobile, the back part is fixed and is called the root of the tongue. The movable part of the tongue is divided into: tip, anterior edge (blade), lateral edges and back. The complex plexus of the muscles of the tongue and the variety of their attachment points provide the ability to change the shape, position and degree of position of the tongue within a wide range. This is very important because... the tongue is involved in the formation of vowels and almost all consonant sounds (except labials).
An important role in the formation of speech sounds also belongs to the lower jaw, lips, teeth, hard and soft palates, and alveoli. Articulation consists in the fact that the listed organs form slits, or closures, that occur when the tongue approaches or touches the palate, alveoli, teeth, as well as when the lips are compressed or pressed against the teeth. The volume and clarity of speech sounds are created thanks to resonators. Resonators are located throughout the extension pipe.
The extension tube is everything that is located above the larynx: the pharynx, oral cavity and nasal cavity.
In humans, the mouth and pharynx have one cavity. This creates the possibility of pronouncing a variety of sounds. In animals (for example, a monkey), the cavities of the pharynx and mouth are connected by a very narrow gap. In humans, the pharynx and mouth form a common tube - the extension tube. It performs the important function of a speech resonator. The extension pipe in humans was formed as a result of evolution.
Due to its structure, the extension pipe can change in shape and volume. For example, the pharynx can be elongated and compressed and, conversely, very stretched. Changes in the shape and volume of the extension pipe are of great importance for the formation of speech sounds. These changes in the shape and volume of the extension pipe create the phenomenon of resonance. As a result of resonance, some overtones of speech sounds are enhanced, while others are muffled. Thus, a specific speech timbre of sounds arises. For example, when the sound a occurs, the oral cavity expands, and the pharynx narrows and stretches. And when pronouncing a sound and vice versa, the oral cavity contracts and the pharynx expands.
The larynx alone does not create a specific speech sound; it is formed not only in the larynx, but also in resonators (pharyngeal, oral and nasal). When producing speech sounds, the extension pipe performs a dual function: a resonator and a noise vibrator (the function of a sound vibrator is performed by the vocal folds, which are located in the larynx). The noise vibrator is the gaps between the lips, between the tongue and teeth, between the tongue and the hard palate, between the tongue and the alveoli, between the lips and teeth, as well as the closures between these organs broken by a stream of air.
Using a noise vibrator, voiceless consonants are formed. When the tone vibrator is turned on simultaneously (vibration of the vocal folds), voiced and sonorant consonants are formed.
The oral cavity and pharynx take part in the pronunciation of all sounds of the Russian language. If a person has correct pronunciation, then the nasal resonator is involved only in pronouncing the sounds m and n and soft variants. When pronouncing other sounds, the velum palatine, formed by the soft palate and a small uvula, closes the entrance to the nasal cavity.
So, the first section of the peripheral speech apparatus serves to supply air, the second - to form the voice, the third is a resonator that gives the sound strength and color and, thus, the characteristic sounds of our speech, arising as a result of the activity of individual active organs of the articulatory apparatus.
In order for words to be pronounced in accordance with the intended information, commands are selected in the cerebral cortex to organize speech movements. These commands are called articulation programs . The articulatory program is implemented in the executive part of the speech motor analyzer - in the respiratory, phonation and resonator systems.
Speech movements are carried out so precisely that as a result, certain speech sounds arise and oral (or expressive) speech is formed.
UNDERSTANDING ABOUT FEEDBACK COMMUNICATION . We said above that nerve impulses coming from the central speech apparatus set the organs of the peripheral speech apparatus in motion. But there is also feedback.
How is it carried out?
This connection functions in two directions: the kinesthetic pathway and the auditory pathway.
For the correct implementation of a speech act, control is necessary: 1. with the help of hearing; 2. through kinesthetic sensations.
In this case, a particularly important role belongs to kinesthetic sensations going to the cerebral cortex from the speech organs. It is kinesthetic control that allows you to prevent an error and make a correction before the sound is pronounced.
Auditory control operates only at the moment of pronouncing a sound. Thanks to sound monitoring, a person notices an error. To eliminate the error, you need to correct the articulation and control it.
Return impulses go from the speech organs to the center, where they control the position of the speech organs at which the error occurred. An impulse is then sent from the center, which causes precise articulation. And again the opposite impulse arises - about the achieved result. This continues until articulation and auditory control are matched. We can say that feedback functions as if in a ring - impulses go from the center to the periphery and then from the periphery to the center.
This is how feedback is provided and a second signaling system . An important role here belongs to systems of temporary neural connections - dynamic stereotypes that arise due to repeated perception of language elements (phonetic, lexical and grammatical) and pronunciation. The feedback system ensures automatic regulation of the functioning of the speech organs.
Brain functions
It is almost impossible to list all the functions. Areas of the brain are responsible for all human actions in everyday life.
Main functions:
- Reasonable function, or human thinking.
- Processing of external signals that coordinates taste, vision, hearing, and smell.
- Managing psychological state and emotions.
- Regulation of basic movements, reflex function.
In ordinary life, a person does not think about why he acts one way or another. The brain is responsible for all actions.
Departments
If you delve into the topic, in order to determine which part of the brain is responsible for speech, you need to know what main sections this human organ consists of. They are usually called shares. The structure and functions of the cerebral hemispheres play a vital role in the life of each of us.
The human brain has the following lobes:
- Frontal.
- Temporal.
- Parietal.
- Occipital.
Separate from the structure and functions of the cerebral hemispheres, the cerebellum, which is responsible for coordinating the body in space, and the pituitary gland, which regulates the production of hormones, are distinguished.
Not in all cases, scientists agree on which part is responsible for what. This speaks first of all about the great lack of knowledge about the areas of the brain and the imperfections of modern medicine.
Frontal lobe
Returning to the question of which part of the brain is responsible for speech, it is necessary to dwell on the study of the frontal lobe. First of all, there is a statement that the left hemisphere of the brain is responsible for the ability to speak. Speech centers are located here.
The frontal part of the cerebral hemispheres is of great importance in human daily life. She is responsible for:
- The nature of thinking.
- The process of urination.
- Maintaining the body in an upright position.
- Motivation and behavior control.
- Speech and handwriting.
The frontal lobe takes responsibility for the semantic construction of human speech.
Temporal lobe
The role of this part of the brain is not so extensive, but much more narrowly focused. The temporal lobes are located in both the left and right hemispheres of the brain, which affects their basic functions.
The left temporal lobe is responsible for:
- Perception of sound information.
- Short-term memory.
- Selection of words during a conversation (role in speech formation).
- Synthesis of visual and auditory information.
- Interaction of music and emotions.
The right temporal lobe is responsible for:
- Facial expression recognition.
- Perception of rhythm and musical tone.
- Perception of speech intonation.
- Recording visual facts.
This part of the brain allows a person to understand by the intonation of the interlocutor’s speech about his emotions and attitude to the issue under discussion.
The role of sensory integration in the speech development of a child
. Candidate of Medical Sciences.
Aladina E.A. What is speech? Speech is the highest mental function, which is provided by two centers located in different parts of the brain:
Wernicke Center.
Location: auditory cortex of the temporal lobe. Responsible for the perception of speech sounds.
Broca's Center.
Location: lower parts of the frontal lobe. Responsible for speech-motor function (reproduction of sounds, words and phrases).
Depending on the predominance of one or another center, speech is divided into impressive and expressive.
Impressive speech
is the process of perceiving words by ear, understanding their meaning, as well as the meaning of the statement as a whole.
Expressive
speech is the process of uttering words in a certain language. In left-handers, speech centers are located in the right hemisphere, in right-handers - in the left.
With the most serious speech disorders, not only the pronunciation of sounds suffers, but also the ability to distinguish sounds by ear. At the same time, the child’s active (used in speech) and passive (the one that the child perceives by ear) vocabulary is limited, and problems arise with the construction of sentences and phrases. All these violations, if not corrected in time, cause difficulties in communicating with others. In the future, they can lead to the development of complexes in the child, preventing him from learning and fully revealing his natural abilities and capabilities.
According to the severity, speech disorders can be divided into those that are not an obstacle to learning in a public school, and severe disorders that require special training. The most common severe speech disorders are alalia, various types of dysarthria, some forms of stuttering, etc.
Alalia
is a complete or partial absence of speech in children with good physical hearing, caused by underdevelopment or damage to the speech areas of the brain. With sensory alalia, the child does not understand someone else’s speech well, and does not recognize the sounds of speech: he hears that the person is saying something, but does not understand what exactly. This is similar to how we do not understand speakers of a foreign language unknown to us. Often children with sensory alalia are mixed with children who have a disorder of the auditory analyzer.
With motor alalia, the child cannot master the language (its sounds, words, grammar). Often children with motor alalia resemble children with mental retardation.
Causes of speech disorders.
From the point of view of exposure time, causes are divided into hereditary and acquired.
Hereditary: - late maturation of the speech zones of the cerebral cortex - left-handedness (causes stuttering, impaired reading and writing during relearning) - a certain ratio in the functioning of the right and left hemispheres (in girls - the left hemisphere develops faster, in boys speech disorders are more common) - genetic disorders, neuropsychiatric diseases of parents
Acquired: Prenatal and natal period (pregnancy and childbirth): 1) Hypoxic (impaired oxygen supply to the placenta, asphyxia during childbirth) 2) Infectious (influenza, rubella, measles, toxoplasmosis. Especially in the first half of pregnancy) 3) Toxic (causing damage brain structures: medications, Rh conflict, blood type incompatibility, maternal diseases (pyelonephritis, etc.), exposure to chemicals, radiation) 4) Mechanical (injuries during pregnancy, childbirth, the use of traumatic methods of obstetrics)
In the early postnatal (postpartum) period, the causes of speech impairment are divided into: 1) Biological (meningitis, encephalitis; chronic somatic diseases: infectious and other injuries to the head, organs of the speech apparatus). 2) Social (lack of attention to the child’s speech, mental trauma, bilingualism in the family, retraining for left-handedness).
However, speech disorders in children are not always associated with damage to speech centers in the brain. Until about 7 years of age, a child's brain functions as a processing device for sensory information received through the senses (taste, smell, touch, movement, gravity, and position in space). Children are busy perceiving things and moving their bodies according to their sensations. Therefore, the age up to 7 years of life is called the period of sensorimotor development.
Organizing sensations about the physical state of our body or environment is called sensory integration. Thanks to it, the brain provides effective body reactions and perceptions, forms emotions and thoughts.
Some people have problems with their auditory or visual systems, and the vestibular system can have exactly the same problems.
In a child with delayed speech development, a competent specialist in sensory integration disorders will note a violation of the vestibular system. How might they manifest themselves?
Nonverbal children make more sounds than usual and engage in active play that stimulates the vestibular system. Children with reduced activity of the vestibular system are able to ride roller coasters or merry-go-rounds longer than others. In addition, they do not feel either weakness or nausea even after heavy and prolonged physical activity. They may also exhibit vestibular-bilateral disorders: clumsiness, difficulty riding a bicycle. Such children often fall without even noticing the fall and make no attempt to restore their balance.
The cause of these disorders is a violation of the development of sensory systems, which develop interdependently. Thus, speech communication depends not only on hearing, but also on touch, vision, and interaction with many sensory and motor functions associated with learning and behavior.
The brain does not process and organize the flow of sensory impulses, and as a result, the child does not receive accurate information about himself and the world around him. Many children whose sensory systems are malfunctioning have average or above average intelligence. If multiple areas of the brain have problems processing signals, then forming generalizations, ideas, and other intellectual problems may be difficult for the child, which at first glance appears to be a developmental disorder.
The auditory system also works closely with the vestibular system. Children with auditory processing disorder may try to listen to the teacher in class, but the sounds from the playground under the windows, the noise of cars and the whispers of classmates make it very difficult for them to understand the explanations. Such children often look around at other children, looking for visual cues in the lesson.
Studies of children with learning difficulties caused by hearing or speech impairments have shown that improvements in reading tests were noted after activities that stimulate the vestibular and proprioceptive senses, but not after language training.
How can you notice a child's auditory processing disorder: Checklist “Processing of Sound Stimuli” from the book “The Child and Sensory Integration” by E. Jean Ayres:
Do you notice that your child: - does not always respond when you contact him? — misunderstands the words addressed to him? - confuses similar words (“bring the cat” instead of “bring the spoon”) - partially understands, but misses details of clearly spoken instructions or stories - hears well in quiet, but gets confused in a noisy environment? - can’t correctly indicate the direction where the sound is coming from? — can’t watch and listen at the same time? — speaks monotonously or very loudly? - demonstrates high sensitivity to noise, sometimes hears what others do not hear? - looks confused if people around are laughing, making noise and talking at the same time.
In conclusion, it should be noted: children who have not developed speech by the age of 2.5-3 years should be examined comprehensively. This includes an examination by a speech therapist, a psychiatrist, an electroencephalographic study, and an examination by a neurologist or other sensory integration specialist. This will make it possible to carry out a differentiated approach to diagnosis and determine an individual rehabilitation plan for the child, taking into account such an interdisciplinary problem as impaired speech development in children.
Speech centers of the brain
Various human speech disorders have motivated scientists to study how this fact is affected by the functioning of the brain. It has been determined that there are several speech centers that are located predominantly in the left hemisphere. In joint interaction, they maintain a person’s speech at the proper level. If any part is injured, this will certainly affect the quality and ability to speak.
There are two main speech areas of the brain:
- Motor zone.
- Sensory area.
- Association Center.
Each of them is responsible for clearly defined functions.
Human speech involves neurons from both hemispheres of the brain
Until recently, it was generally accepted that the speech center, that is, the areas of the brain that allow us to perceive and pronounce sounds, is located primarily in the left hemisphere. New York University specialists
and
Langone University Medical Center
have proven that both hemispheres are equally involved in speech.
Dyslexia due to poor connections
Scientists have found that disruption of connections between the frontal and temporal lobes of the brain causes dyslexia...
06 December 15:49
These results, published in the journal Nature
, change established ideas about the neural activity of the brain.
According to classical concepts, the perception and processing of sounds occurs in Wernicke's sensory area
(in the posterior part of the superior temporal gyrus), and their pronunciation is controlled by
Broca's motor area
(in the posterior lower part of the third frontal gyrus). Both are located in the left hemisphere. These zones are connected and form the sensorimotor system of speech. However, these data are based on indirect studies of brain activity in stroke patients with speech difficulties. Studies have also been conducted on healthy volunteers, but the main method used is functional magnetic resonance imaging, which is based on measuring cerebral blood flow while the subject performs various tasks.
American scientists were able to conduct a direct study of the participation of brain neurons in the speech process.
In the rhythm of words
The sense of rhythm and the ability to follow it are directly related to the ability to perceive information, it has been established...
18 September 13:17
They used a method called electrocorticography, in which neural activity is recorded using electrodes placed directly on the surface of the cortex. The method allows one to obtain high spatial and temporal resolution. Naturally, no one will drill into the patient’s skull for experimental purposes—such electrodes are implanted for the purpose of treating some neurological disease.
The study involved patients undergoing pharmacological treatment for epilepsy. Six patients had electrodes inserted into the left hemisphere, seven into the right, and three into both hemispheres of the brain. The subjects performed three types of tasks: simply listening to syllables, repeating the heard syllables out loud, and repeating them silently, that is, moving their lips, tongue, and jaws. In some experiments, patients listened to and repeated the monosyllabic words heat, hit, hat, hoot, het, hot, hut; in others, the nonsense syllables “kig” and “pob” . The use of insignificant syllables made it possible to separate speech ability, that is, the ability to hear and pronounce sounds, from language activity - the ability to form phrases and understand their meaning.
Scientists have identified the areas of the brain that are most involved in performing all types of tasks.
Singing hamsters will help stutterers
If we understand which genes unique South American rodents use in their trills, we may be able to...
08 September 11:26
It turned out that while listening and repeating syllables, neurons located in both hemispheres are activated.
These are neurons in the supramarginal, middle temporal and superior temporal gyri, somatosensory and motor cortex, premotor cortex and inferior frontal gyrus. They provide the perception and pronunciation of sounds, the connection between what a person hears and what he says (repeats).
The language center differs from the speech center; it is a center of a higher level of information processing, it provides an understanding of the meaning of words.
And it is the language center that is located in the left hemisphere.
close
100%
According to the classical model (bottom), speech production (blue frame), sensory-motor interaction (red frame) and the language center (yellow frame) are in the left hemisphere, and only speech perception (green frame) is in both hemispheres; According to the new model ( above) only the language center is located in the left hemisphere, and the remaining functions are in both.
Greg Cogan, Bijan Pesaran
When the mechanisms of speech generation are known, speech disorder problems can be more successfully addressed. Researchers hope to develop more effective methods of rehabilitation for patients suffering from speech disorders after a stroke.
Functions
The motor area is located in the front part of the frontal lobe of the left hemisphere, next to the motor center, which is responsible for muscle activity. Main function of the motor area (Broca's area):
- Responsible for the motor ability of the tongue. In case of any violations in this department, the person continues to understand speech, but is not able to respond.
The sensory area is located in the posterior part of the temporal lobe of the brain. The main task of this center (Wernicke Center) is:
- Perception and storage of oral speech, both one’s own and those of others. If disturbances occur in this area, then the person ceases to perceive the speech of others, although he himself retains the ability to speak, albeit with defects.
If for some reason the sensory speech zone has to be removed, then the person completely loses the ability to perceive and produce speech.
Speech localization. Broca's area and Wernicke's area
Brock and Wernicke studied patients whose difficulties in producing and understanding speech could be linked to damage in various areas of the brain.
In 1861, French neurologist Paul Pierre Broca (1824–1880) proposed that there was an area in the frontal lobe that specialized in speech production. Broca based this idea on his study of stroke patients who spoke words slowly and with difficulty, often with jumbled sentence structure. Below is an example of speech from a modern patient with similar symptoms. This man is trying to describe when he had a stroke that occurred while he was in a hot bath.
Fine. . . Uh. . . stroke and... I... yes tavanna gar... G... g... hot bath and... And... two days when uh... pain... uh... hospital and uh... soon... ambulance for... help. (Dick et al., 2001, p. 760)
Although Broca's patients had difficulty expressing themselves, they easily understood what other people were saying. When the patients died, Paul Broca performed autopsies and determined (1865) that one specific area of the brain had been damaged (Figure 2.12). This area in the frontal lobe - the motor speech center - is called Broca's area (or Broca's area). This is a section of the cerebral cortex in the posterior inferior part of the third frontal gyrus of the left hemisphere, which provides the motor organization of speech.
A speech disorder (aphasia) caused by damage to Broca's center is called Broca's aphasia. This anarthric syndrome is characterized by the inability to combine individual speech movements into a single speech act.
Rice. 2.12. Broca's and Wernicke's areas were identified in early studies as specialized for speech production and comprehension.
In 1879, German neuropsychiatrist Carl Wernicke (1848–1905) studied another group of patients who had damage to an area of the temporal lobe that would become known as Wernicke's sensory speech area, or Wernicke's area. The patients' speech is fluent and grammatically correct, but usually incoherent. The following is a modern example of patient speech similar to those studied by Wernicke:
A difficulty just suddenly arose and all the effort disappeared with it. He even stepped on my ledge. You know, they took them from the earth. They made my beloved nine broken, and now I am gripped by the persistence of my abolition, which is now forever. (Dick et al., 2001, p. 761)
Such patients not only utter meaningless phrases, they also cannot understand the speech of others or printed text. This condition is called Wernicke's aphasia.
Unlike Broca's area, which is responsible for speech production, Wernicke's speech area is involved in the process of assimilation and understanding of written and oral speech.
The direct connection between word production and Broca's area, and speech comprehension and Wernicke's area, has been an accepted model of language processing for many years.
But generally accepted models are often revised in response to new data, and the Broca/Wernicke model is no exception.
Beginning in the 1970s, researchers began to obtain new data on language processing in the brain. One line of evidence shows how important it is to pay close attention to how the behavior of brain-damaged patients is tested.
The idea that patients with Broca's aphasia can understand language but have problems producing it (impaired at the syntactic level) has been challenged by research showing that these patients do have problems understanding language. Consider, for example, the following two sentences:
1. The girl ate the apple. (The apple was eaten by the girl).2. The boy was pushed by the girl. (The boy was pushed by the girl).
Patients with Broca's aphasia understand the first sentence easily but have difficulty with the second. The problem they have with the second proposal is deciding who was pushing and who was being pushed. Did the girl push the boy or did the boy push the girl? Although it may seem obvious to you that a girl pushed a boy, patients with Broca's aphasia have difficulty processing connecting words such as was and by, making it difficult to determine who was pushed.
On the contrary, the first sentence cannot be interpreted in two ways. It is clear that the girl ate the apple because the converse is not possible, except in the unlikely science fiction scenario of the apple eating the girl (Dick et al., 2001; Novick et al., 2005).
The fact that Broca's patients have real problems understanding language indicates that Broca's aphasia is not just a problem with language production.
The results of many behavioral and physiological experiments have led some researchers to distinguish not between problems of reproduction and comprehension, but into problems with form and meaning.
Problems with form are associated with difficulties in determining the relationship between words in a sentence (for example, the problem of patients with Broca's aphasia with sentence 2.
Problems with meaning include wider differences in comprehension, as in patients with Wernicke's aphasia who will also have difficulty with sentence 1.
A method of recording rapid electrical responses in the brain, called event-related potential (ERP), has provided additional capabilities for distinguishing form and meaning.