What is syringomyelia?
The spinal cord is an organ of the nervous system; it runs inside the spinal column from the cranial foramen, which communicates with the spinal column, to the first lumbar vertebra. Along its entire length - from the base of the skull to the coccyx, which ends the spinal column - sensory and motor nerves branch off from it. The structure of the spinal cord is the same as that of the brain - its central part, shaped like a butterfly, consists of gray matter with a predominance of nerve cells and a shell of white matter with a predominance of nerve fibers. The disease, in which a cyst-like cavity forms in the spinal cord, affects mainly the gray matter and is called syringomyelia , because the hole in the central spinal canal gives the spinal cord a flute-like appearance (in Greek, “syrinx”). In most cases, the origin of syringomyelia is unknown.
At our Institute, thanks to more than 40 years of research into the cause of Syringomyelia, a minimally invasive surgical technique has been developed for the treatment of idiopathic Syringomyelia: dissection of the filum terminale at the level of the sacrum with the unique Filum System® method (More information can be read below).
Fig. 1. – A 26-year-old man complains of loss of temperature sensitivity in the left half of the body and head, especially noticeable when taking a shower. The disease appeared a year ago. After surgical intervention - dissection of the terminal filum of the spinal cord - sensitivity was restored immediately after the operation. For 5 years after surgery, syringomyelia is practically asymptomatic.
Lobes and segments of the lungs
Right lung
Upper lobe
Apical segment, S1 - located behind the second rib of the chest. Segment 1 of the lung includes airways with a total length of about 2 cm. The segment is connected by the airways to S2.
Posterior segment, S2 - in relation to the apical segment 2, it is located dorsally (lower, towards the back) at the level of 2-4 ribs. The segment is connected by the respiratory tract to S1, through the vascular branch to S3 and to the pulmonary artery.
Anterior segment, S3 - located frontally between the 2nd and 4th ribs. The 3rd segment of the lung includes the superior branch of the pulmonary artery.
It is with damage to the upper lobes of the lungs that most infectious and inflammatory diseases of the lungs begin, for example pneumonia, tuberculosis, granulomatosis. Since adjacent segments of the lungs, artery and bronchus are interconnected, it is important to promptly determine the type of infectious pathogen and begin treatment to prevent further spread of the disease.
Bullae (air cavities) in emphysema are also localized here.
Upper lobe
Lateral segment, S4 - located in the anterior part of the axilla between the 4th and 6th ribs.
Medial segment, S5 - located in the front of the chest at the level of the 4th and 6th ribs.
Thus, the 4th and 5th segments of the lung are located in the mid-frontal part of the lung at the same level, penetrated by tubular branches of the bronchi and vessels. At this level, neoplasms and metastases are found more often than in the upper lobes of the lungs.
Lower lobe
The upper segment, S6 - is projected onto the lower half of the scapula: from the center to the corner, at the level of 3-7 ribs. Blood supply in the 6th segment of the right lung is carried out through the artery - a continuation of the lower pulmonary.
The medial basal segment, S7, is also called the “cardiac” segment because it is located closer to the diaphragm on the inside, closer to the right atrium. A branch of the vena cava passes nearby. High-resolution computed tomography is the only research method in which the 7th segment of the lung is clearly visible.
Anterior basal segment, S8 - located at the level of the 6-8 rib in the projection from the middle of the axilla.
Lateral basal segment, S9 - located between the 7th and 9th ribs in projection to the posterior part of the axilla.
Posterior basal segment, S10 - located between the 7th and 10th ribs and adjacent to the spine.
Left lung
Upper lobe
The apical-posterior segment, S1-S2, is structurally and functionally practically no different from the 1st and 2nd segments of the right lung. The apical and posterior segments on the left side are often combined due to the common bronchus. Thus, this is the largest segment.
Anterior segment, S3 - located between the 2nd and 4th ribs closer to the sternum.
The upper lingular segment, S4, is located in the mid-anterior part of the chest at the level of 3-6 ribs in projection to the center of the armpit. This is also one of the largest segments.
The lower lingular segment, S5, is located under the 4th segment of the left lung. Separated from segment 4 by an interlobar fissure.
Lower lobe
The upper segment, S6 - in localization and structural and functional properties coincides with the 6th segment on the right.
Basal-medial, cardiac segment, S7 - in localization and structural and functional properties coincides with the 7th segment of the lung on the right.
Anterior basal segment, S8 - in localization and structural and functional properties coincides with the 8th segment of the lung on the right.
Lateral basal segment, S9 - in localization and structural and functional properties coincides with the 9th segment of the lung on the right.
Posterior basal segment, S10 - in localization and structural and functional properties coincides with the 9th segment of the lung on the right.
The sizes and shapes of the pulmonary segments depend on the individual characteristics of the patient’s body and may vary.
Many lung diseases, such as pneumonia, tuberculosis, and abscesses, begin with a small lesion in one segment of the lungs. According to their localization and specific pattern of the disease, which is visualized on tomograms.
By studying images on cross-sectional scans and 3D reconstructions, a radiologist can give an initial conclusion on the changes identified on a CT scan. Differential CT diagnostics means that in most cases the doctor will be able to accurately distinguish tuberculosis from pulmonary granulomatosis, and “ground glass” in pneumonia from tumor infiltrate.
Are there any undesirable consequences of cutting this ligament?
The filum terminale is formed by the empty membranes of the spinal cord in its lowest section - the lumbosacral. In a human embryo, the vertebral column and spinal cord are the same length, and they are separated by membranes - hard, arachnoid and soft. During normal growth, the adult vertebral column is approximately 20 cm longer than the spinal cord. The membranes that separate the spinal cord from the spinal column in the sacrum and lumbar region, hard, arachnoid and soft, no longer contain the spinal cord and gather into something like a fibrous cord, forming the filum terminale; this end of the spinal cord resembles a sock that we pulled halfway onto our leg, and the empty part of this sock can be cut off without any harm to the leg. In the same way, the filum terminale of the spinal cord can be cut in any part without any consequences (1, 2).
What are the segments?
The sections of the spinal cord differ from those used to conventionally divide the areas of the spine. Their length varies; the fewest elements are found in the coccygeal part. The segments are connected to certain areas in the body by nerve conductors. In general, the brain is divided into the following segments:
Prognosis for spinal cord myelitis
- Neck – 8.
- Chest – 12.
- Sacral – 5.
- Lumbar – 5.
The main length falls on the thoracic segments of the spinal cord, after which 23.2% is allocated to the neck and only 7.3% to the lower back. They are posterior and anterior nerve roots that alternate regularly. They are located above the vertebrae with the same number. Their main task is to report movements and be responsible for muscle contractions. Therefore, the anterior nerve roots are also called motor, and the posterior - sensitive.
The intervertebral foramen contains the roots of each individual segment. Their direction is not the same, because the spinal column is filled with the brain. In the cervical region they lie horizontally, in the thoracic region they are directed diagonally, and in the lower part they are almost vertical.
The shortest segments are the neck segments, and the longest ones are in the lower back and sacrum. In the lower part they form the so-called “horse tail” - this is a bunch of roots located below the 2nd vertebra.
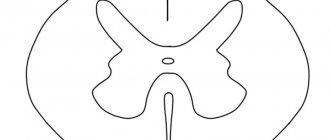
A visual representation of what a spinal cord segment looks like in cross section
No ads 1
Are there any other effects of spinal cord traction?
Tension of the filum terminale not only provokes syringomyelia , but also generates a flexion reflex in the spinal column, leading to scoliosis . To avoid strain on the spinal cord, it forces the lower part of the brain, the so-called tonsils of the cerebellum, to descend down the foramen magnum, through which the cranium communicates with the spinal column. This causes Arnold-Chiari malformation , a disease described 100 years ago, the cause of which remains unknown.
Concept of a spinal cord segment.
A spinal cord segment is a section of the spinal cord corresponding to two pairs, two anterior and two posterior, of the spinal nerve roots. The section of the spinal cord corresponding to two pairs of roots (two anterior and two posterior) is called a segment. In accordance with the thirty-one pairs of spinal nerves, the spinal cord is divided into 31 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral and 1-3 coccygeal segments. Each segment of the spinal cord corresponds to a specific area of the body that receives innervation from this segment of the spinal cord. The segments are named in Latin letters with indices indicated by Roman numerals. The letters correspond to the initial letters of the name of the region (part) of the spinal cord, and Roman numerals correspond to the serial number of the segment: – cervical segments, CI - CVIII (CI - CVIII); – thoracic segments, ThI - ThXII (ThI - ThXII); – lumbar segments, LI – LX (LI – LX); – sacral segments, SI - SV (SI - SV); – coccygeal segments, CoI - CoIII (CoI - CoIII). The length of the spinal cord is significantly less than the length of the spinal column in the canal of which it is located. Therefore, the serial number of any segment of the spinal cord and the level of its position do not always correspond to the serial number of the vertebra of the same name. The upper cervical segments are located at the level of the vertebral bodies corresponding to their serial number. There is no distal correspondence. The lower cervical and upper thoracic segments lie at the level of one overlying vertebra. In the middle thoracic region, this difference between the corresponding segment of the spinal cord and the vertebral body increases by 2 vertebrae, in the lower thoracic region - by 3. The lumbar segments of the spinal cord lie in the spinal canal at the level of the bodies of the X, XI thoracic vertebrae, the sacral and coccygeal segments - by level of the XII thoracic and I lumbar vertebrae.
Reflex arc.
Reflex arc (nerve arc) is the path traversed by nerve impulses during the implementation of a reflex.
The reflex arc consists of:
· receptor - a nerve link that perceives irritation;
· afferent link - centripetal nerve fiber - processes of receptor neurons that transmit impulses from sensory nerve endings to the central nervous system;
· central link - nerve center (optional element, for example for the axon reflex);
· efferent link - carries out transmission from the nerve center to the effector.
· effector - an executive organ whose activity changes as a result of a reflex.
· executive organ - puts the body into action.
There are:
· monosynaptic, two-neuron reflex arcs;
· polysynaptic reflex arcs (include three or more neurons).
Divisions of the brain.
The brain is the most important organ of the human body. The parts of the human brain are presented in the form of 5 functional areas (divisions). Each department has its own structure and functionality. The brain is protected by the bones of the skull. The average weight of an adult's brain is 1.3 kg, and that of an infant is 0.4 kg.
Brain department
| Department function | |
| Average | This is a continuation of the brain of the vertebral region of the back. It performs conductive and reflex functions. Processes information received through visual and auditory receptors. |
| Intermediate | Exercises general control over the activities of the central nervous system and autonomic nervous system, the endocrine system, regulates general metabolism, and coordinates sleep. Monitors the working condition of the organs of vision and hearing. |
| Rear | Exercises control over unconditioned reflexes. |
| Oblong | Controls the functioning of the heart, respiratory organs, and vasomotor system. Controls the unconditioned reflexes of the digestive system and protective reflexes. |
| Front | Controls the activities of the entire organism as a whole. Responsible for the mental activity of the human body and the state of the individual’s psyche. |
What happens to a syringomyelic cyst?
In syringomyelia , dissection of the filum terminale of the spinal cord delays the development of the disease. A cyst formed as a result of cell death may remain unchanged, but it may disappear with the spontaneous opening of the space surrounding the spinal cord, or it may move into its central canal, where there is an ependymal canal, through which the central canal of the spinal cord communicates with the cavities of the brain . Syringomyelia symptoms are caused by cell death and the toxic tumor effect of the cyst. Cutting the filum terminale of the spinal cord has two beneficial effects: it delays cell death that was caused by the tension on the spinal cord, and it reduces the toxic tumor effect of the cyst on the spinal cord.
Bibliography
- Dr. Miguel B. Royo Salvador (1996), Siringomielia , escoliosis y malformación de Arnold-Chiari idiopáticas, etiología común (PDF). REV NEUROL (Barc); 24 (132): 937-959.
- Dr. Miguel B. Royo Salvador (1996), Platibasia , impresión basilar, retroceso odontoideo y kinking del tronco cerebral, etiología común con la siringomielia , escoliosis y malformación de Arnold-Chiari idiopáticas (PDF). REV NEUROL (Barc); 24 (134): 1241-1250
- Dr. Miguel B. Royo Salvador (1997), Nuevo tratamiento quirúrgico para la siringomielia , la escoliosis , la malformación de Arnold-Chiari , el kinking del tronco cerebral, el retroceso odontoideo, la impresión basilar y la platibasia idiopáticas (PDF). REV NEUROL; 25 (140): 523-530
- M. B. Royo-Salvador, J. Solé-Llenas, J. M. Doménech, and R. González-Adrio, (2005) “Results of the section of the filum terminale in 20 patients with syringomyelia , scoliosis and Chiari malformation .” (PDF). Acta Neurochir (Wien) 147:515–523.
- M. B. Royo-Salvador (1992), “Aportación a la etiología de la siringomielia ,” Tesis doctoral (PDF). Universidad Autónoma de Barcelona.
- M. B. Royo-Salvador (2014), “Filum System® Bibliography” (PDF).
- M. B. Royo-Salvador (2014), “Filum System® Guía Breve.”