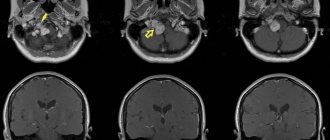
Find out more about nervous diseases starting with the letter “N”: Sleep disturbance; Narcolepsy; Hereditary cerebellar ataxia of Pierre-Marie; Spinal circulatory disorders; Trigeminal neuralgia; Neuralgia of the submandibular and sublingual nodes; Neuralgia of the glossopharyngeal node; Neuralgia of the ear ganglion; Neurasthenia; Neural amyotrophy of Charcot-Marie-Tooth; Acoustic neuroma; Neuroma; Optic neuritis; Pharyngeal neuritis; Neuritis of the facial nerve; Neuritis; Obsessive-compulsive neurosis; Pharyngeal neurosis; Neuroses; Neurosis-like stuttering; Femoral nerve neuropathy.
Femoral nerve neuropathy is an injury to the most powerful nerve in the lumbar region, has various origins, causing pathologies in the penetration of nerve signals. Symptoms depend on the type of injury, appearing in the form of pain, sensory disturbances in the lower extremity, mainly in the anteromedial areas of the thigh and lower leg. Gait disorders occur due to difficulties in knee extension.
The diagnosis is made based on ultrasound of the femoral nerve and EMG. The therapy is complex and is aimed at eliminating nerve compression and inflammation, relieving pain and swelling, restoring innervation and metabolism. A course of electrical stimulation therapy and physical therapy is required.
general information
In 1822, the disease was described for the first time as anterior crural neuritis. Inflammation of the femoral nerve has been studied for almost 200 years, but remains poorly understood. Among mononeurotic pathologies, femoral neuritis is more common than others. The lack of complete information on this type of neurological disorders leads to the fact that the disease cannot be differentiated from radicular syndrome or myelopathy. Difficulties arise due to the variability of clinical symptoms from sensory distortions to movement disorders, depending on etiological factors.
Epidemiology/Etiology
According to Boyajian-O'Neill LA et al. There are two types of piriformis syndrome - primary and secondary.
Primary SGM
Primary SHM has an anatomical cause, variations of which may include a divided piriformis muscle, a divided sciatic nerve, or an abnormal sciatic nerve pathway. Among patients with BMS, less than 15% of cases are due to primary causes. There are currently no accepted values for the prevalence of the abnormality and little evidence to support whether sciatic nerve abnormality results in FMS or other types of sciatica. These observations suggest that piriformis muscle and sciatic nerve abnormalities may not be as significant in shaping the pathophysiology of FMS as previously thought.
Secondary SGM
Secondary SHM occurs as a result of aggravating factors, including macro- or microtrauma, the effect of prolonged accumulation of ischemia, and the existence of local ischemia.
- FMS most commonly (50% of all cases) occurs due to macrotrauma to the buttocks, leading to soft tissue inflammation, muscle spasm, or a combination of these factors, ultimately resulting in nerve compression.
- Piriformis muscle spasms are most often caused by direct trauma, post-surgical injury, pathology, or excessive stress on the lumbar spine and/or sacroiliac joint.
- FMS can also be caused by shortening of muscles due to altered biomechanics of the lower extremity and lumbosacral region. This can cause compression or irritation of the sciatic nerve. When piriformis dysfunction exists, it can cause a variety of symptoms in the sciatic nerve, including pain in the gluteal region and/or the hamstring, calf, and lateral foot. Microtrauma can occur due to overuse of the piriformis muscle, such as long-distance walking or running or direct compression.
Etiology of FMS
| Injury to the sacroiliac and/or gluteal region | Predisposing anatomical variants |
| Myofascial trigger points (read about MPTT here) | Hypertrophy and spasm of the piriformis muscle |
| Consequences of laminectomy | Abscess, hematoma, myositis |
| Piriformis bursitis | Neoplasms in the area of the infrapiriform foramen |
| Colorectal carcinoma | Neuroma of the sciatic nerve |
| Colon lipoma | Complications of intramuscular injections |
| Thigh nails | Myositis ossificans of the piriformis muscle |
| Klippel-Trenaunay syndrome |
Other causative factors include anatomical variations in the sciatic nerve, anatomical changes or hypertrophy of the piriformis muscle, repetitive trauma, sacroiliac arthritis, and hip replacement. Morton's finger may also predispose to the development of FMS.
Skiers, drivers, tennis players and bikers traveling long distances are most susceptible to the occurrence of SHM.
Tonley JC took a different view regarding the causes of SHM. He writes: “The piriformis muscle can function in an elongated position or under high eccentric loads during functional activities secondary to weak agonist muscles. For example, if the hip is excessively abducted and internally rotated during weight-bearing exercises, much of the eccentric load may be transferred to the piriformis muscle due to weakness of the gluteus maximus and/or gluteus medius. Constant stress on the piriformis muscle due to overextension and eccentric work can result in compression or irritation of the sciatic nerve.”
You can read about the gluteus maximus muscle here. Look here about the gluteus medius muscle.
Features of the anatomical structure of the femoral nerve
The lumbar processes of the spinal nerves arise at the level of L2, L3, L4 and merge into a single nerve trunk - the femoral nerve. N. femoralis passes between the iliacus and psoas major muscles, descends to the inguinal ligament and extends to the anterior thigh. Here there is a division into cutaneous, muscle branches and subdermal nerve. The femoral nerve innervates the muscle tissues through which it passes. Muscle functions include flexion and rotation of the hip, and with a stable hip, lumbar flexion and forward bending.
The processes coming from the femoral nerve under the inguinal ligament provide innervation to the hip flexor and knee extensor muscles. Dermal processes guarantee sensitivity of the frontal and part of the inner thigh. The subdermal nerve is the longest, exits in the area of the inguinal ligament, then along the anterior surface of the thigh enters the muscular canal and follows along the medial edge of the knee with the origin of the infrapatellar branch, with innervation of the anterior part of the patella.
Then the subcutaneous branch goes along the median surface area of the leg, foot - to the beginning of the big toe. It provides sensory sensation to the anterior and middle surfaces of the lower leg and the medial part of the foot.
Factors in the formation of the disease
Muscle spasms, injuries and hemorrhages in the psoas muscle lead to compression of the femoral nerve at the iliopsoas border. The cause of compression may be abdominal tumors or hematomas. Hematomas are the result of thrombocytopenia, hemophilia, complications during treatment with anticoagulants in patients with thrombosis, and abdominal aortic aneurysm. Femoral nerve neuropathy can result from damage to the nerve during operations for appendicitis, on the ureters and kidneys, with abscesses of the iliopsoas muscles, and bursitis.
Compression of the femoral nerve in the groin area is caused by femoral hernias, lymphogranulomatosis inguinal, or prolonged forced positioning of the hip. The condition of neuritis occurs as a complication after operations on the hip joint, surgical treatment of inguinal hernias.
In the area of Gunther's canal, femoral neuropathy occurs when the adductor muscles are tense during sports or professional work. Pathologies and instability of the knee joint can also cause muscle tension. The result of knee surgery is iatrogenic femoral neuropathy. Neuropathy of the infrapatellar part of the femoral nerve is associated with the development of thrombophlebitis, varicose veins, and knee injuries.
Ultrasound diagnosis of femoral and sciatic neuropathy in neurological practice
Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.
Introduction
Some of the most common types of pathologies of the nervous system are damage to peripheral nerves and tunnel neuropathies. The incidence of soft tissue injuries involving peripheral nerves, according to various authors, is 25-65% of all cases of injury, and the incidence of tunnel neuropathies is 30-40% of all diseases of the peripheral nervous system [1, 2]. The choice of the most rational methods for diagnosing damage and diseases of the peripheral nerves of the extremities is currently a difficult problem. Existing instrumental diagnostic methods either do not provide images of the nerve trunk (electromyography) or are labor-intensive, requiring complex, expensive equipment (magnetic resonance imaging - MPT). According to a number of foreign authors [3, 4], ultrasound scanning can be quite successfully used in the diagnosis of damage and diseases of peripheral nerves.
Electrophysiological methods, such as electromyography and neuromyography, are traditionally recognized as the “gold standard” for identifying pathology of the peripheral nervous system. However, it should be noted that the information obtained during the above examinations does not provide an idea of the state of the surrounding tissues, does not indicate the nature and cause of damage to the nerve trunk, and does not always accurately reflect the localization of changes. At the same time, it is this information that helps determine the tactics of conservative or surgical treatment. Ultrasound examination (ultrasound) of the peripheral nervous system was first used to diagnose diseases of the nerve trunks in the late 90s of the last century [5], and due to its undeniable advantages over other diagnostic methods, it developed rapidly.
However, despite the publications available in our country on this problem, it should be recognized that the possibilities of ultrasound diagnostics in the assessment of peripheral nerves in chronic pain in the lower extremities remain poorly studied [6].
The purpose of the work was to evaluate the capabilities of ultrasound of the sciatic and femoral nerves in the syndrome of chronic pain in the lower extremities.
Material and methods
This study is based on an analysis of the ultrasound results of 27 patients (18 women, 9 men) aged 30 to 65 years (mean age 47.2 ± 2.4 years) who suffered from chronic pain of the lower extremities.
All patients underwent a comprehensive clinical and instrumental examination, which included a thorough, scrupulous analysis of complaints and medical history, examination by a neurologist, rheumatologist, urologist and/or gynecologist, ultrasound of the femoral and sciatic nerves.
Patients complained of pain with all the features of neuropathic pain, which was often accompanied by the presence of concomitant phenomena such as paresthesia, dysesthesia, allodynia, hyperpathia, hyperesthesia and hypoesthesia. Patients characterized the pain as burning, shooting, stabbing, like an “electric shock”, burning, freezing, piercing with increasing intensity in the gluteal, groin and popliteal areas, limiting the range of movement of the leg. Along with changes in sensitivity, autonomic disorders in the corresponding area were often detected - changes in skin color (hyperemia or cyanosis), impaired tissue trophism, sweating, swelling. As a result, patients had disturbed sleep and had depressive and anxiety disorders. The average duration of pain and limitation of movement ranged from 1 to 3 months.
In terms of diagnostic search to identify possible causes of pain in the pelvic region, 17 patients underwent radiography of the hip joints (coxarthrosis was noted in 16 (94%) patients), and MRI of the lumbosacral spine was performed in 9 patients (degenerative symptoms were detected in 7 (78%) patients). -dystrophic processes). In 15 cases, an ultrasound scan of the pelvic organs was performed, and pathology was detected in 14, including uterine fibroids in 3, signs of external endometriosis in 4, which could be the cause of pain in the buttock and thigh, radiating to the foot, the severity of which depended on phases of the menstrual cycle [7]. 4 men showed signs of chronic prostatitis in combination with benign prostatic hyperplasia of varying degrees.
Ultrasound was performed using modern ultrasound machines with linear sensors with a frequency of 5-13 MHz. During the study, the thickness, structure, and echogenicity of the nerve were assessed. To determine the echogenicity of the nerve, it was compared with the healthy contralateral side and with the adjacent muscles.
It is known that the femoral nerve begins with three branches from the II-IV lumbar spinal nerves, which form a single trunk, descending down between the psoas major and iliacus muscles, and then along the lateral edge of the first (Fig. 1). There are several areas in which the anatomical and topographical features of the femoral nerve predispose to an increased risk of its compression or injury - in the area of the iliopsoas muscle, under the inguinal ligament, in the area of Gunther's canal and at its exit.
Rice. 1.
Anatomy of the femoral nerve, zone of innervation and the place of its most frequent damage ().
Depending on the level of damage, the clinical manifestations of femoral neuropathy vary significantly.
Ultrasound of the femoral nerve was performed with the patient in the supine position. The femoral nerve was visualized in the groin area lateral to the vascular bundle from the level of the inguinal ligament to the upper third of the thigh (Fig. 2, 3). The study was carried out in the transverse and longitudinal scanning planes (Fig. 2, 4).
Rice. 2.
B-mode. Study of the right femoral nerve in the transverse scanning plane at the level of the groin region: BN - femoral nerve, BA - femoral artery.
Rice. 3.
Color flow mode. Study of the right femoral nerve in the transverse scanning plane at the level of the groin region: BN - femoral nerve, BA - femoral artery.
Rice. 4.
B-mode. Examination of the right femoral nerve in the longitudinal scanning plane at the level of the groin region and the upper third of the thigh: arrows - femoral nerve.
The sciatic nerve is the largest peripheral nerve in the human body and exits the pelvic cavity through the greater sciatic foramen under the piriformis muscle (Figure 5). In the area of the gluteal fold, the sciatic nerve is located close to the fascia lata of the thigh, moves laterally and then lies under the long head of the biceps femoris muscle, located between it and the adductor magnus muscle. Depending on the level (height) of the lesion [8], the following types of sciatic nerve neuropathy are possible: very high level, piriformis syndrome (at the level of the infrapiriformis foramen), at the level of the thigh (above the division into the tibial and common peroneal nerves). The topical differential diagnosis of sciatic nerve syndrome often has to be made with discogenic compression radiculopathy LV-SII.
Rice. 5.
Anatomy of the sciatic nerve and innervation zone ().
Ultrasound of the sciatic nerve was performed with the patient lying on his stomach. The sciatic nerve was visualized distal to the ischial tuberosity in the space under the tendons of the semimembranosus and semitendinosus muscles and the long head of the biceps from the gluteal region to the site of division into the tibial and common peroneal nerves. The study was carried out in the transverse and longitudinal scanning plane (Fig. 6, 7).
Rice. 6.
B-mode. Examination of the left sciatic nerve in the transverse scanning plane in the upper third of the posterior surface of the thigh: SN - sciatic nerve.
Rice. 7.
B-mode. Examination of the left sciatic nerve in the longitudinal scanning plane in the upper third of the posterior surface of the thigh: arrows - sciatic nerve.
results
According to ultrasound data, signs of neuropathy were detected in 24 (88.9%) patients. The distribution of identified neuropathies by location and gender of patients based on ultrasound results is presented in Table 1.
Table 1
. Distribution of patients according to the nature of the identified neuropathies.
| Localization of neuropathy | Women | Men | Total | ||||
| abs. | % | abs. | % | abs. | % | ||
| Femoral nerve | Right | 5 | 31,25 | 2 | 25,00 | 7 | 29,20 |
| Left | 4 | 25,00 | 2 | 25,00 | 6 | 25,00 | |
| Sciatic nerve | Right | 2 | 12,50 | 3 | 37,50 | 5 | 20,80 |
| Left | 5 | 31,25 | 1 | 12,50 | 6 | 25,00 | |
| Total | 16 | 100,00 | 8 | 100,00 | 24 | 100,00 | |
In women, damage to the femoral nerve predominated on the right (31.2%), and the sciatic nerve on the left (31.2%); in men, lesions of the sciatic nerve on the right were more often observed, which is consistent with literature data [2].
Normally, the thickness of the femoral nerve at the level of the hip joint in men and women is 0.31 ± 0.08 cm, the thickness of the sciatic nerve in the upper and middle third of the posterior surface of the thigh is 0.4 ± 0.05 cm.
As can be seen from the data in Table 2, with neuropathy there was a uniform increase in the thickness of the nerves: femoral - on average up to 0.56 ± 0.09 cm in women and 0.62 ± 0.20 cm in men; sciatic - on average up to 0.62 ± 0.06 cm in women and 0.66 ± 0.04 cm in men. Local thickening (suspicious of neuromas, schwannomas) or thinning (suspicious of trauma) of the nerve trunks was not detected in our study. In 50% of cases, the echogenicity of the nerve trunks decreased, in 37.5% it was not changed, and in 12.5% it was increased. When comparing the thickness values of the femoral and sciatic nerves obtained during the examination of healthy men and women, as well as when examining the right and left lower extremities, bilateral and gender differences in the parameters turned out to be insignificant.
table 2
. Ultrasound characteristics of neuropathies in gray scale.
| Index | Femoral nerve | Sciatic nerve | ||
| women | men | women | men | |
| Average nerve thickness, cm | 0,56 ± 0,09 (0,47-0,65) | 0,62 ± 0,20 (0,50-0,70) | 0,62 ± 0,06 (0,56-0,68) | 0,66 ± 0,04 (0,62-0,70) |
| Echogenicity, cases | ||||
| decreased normal increased | 5 3 1 | 2 2 0 | 3 3 1 | 2 1 1 |
All patients underwent pathogenetic therapy (muscle relaxants, non-steroidal anti-inflammatory drugs (NSAIDs), B vitamins, anticonvulsants, antidepressants, reflexology - acupuncture, laser puncture), as a result of which 22 showed improvement. During control ultrasound in patients with clinical improvement, a decrease in the thickness of the nerves was noted: femoral - on average to 0.39 ± 0.04 cm in women and 0.40 ± 0.04 cm in men; sciatic - on average up to 0.43 ± 0.02 cm in women and 0.45 ± 0.03 cm in men.
Discussion
Femoral and sciatic neuropathies are fairly common mononeuropathies of the lower extremities [9-11]. Symptoms of femoral neuropathy and other neuropathies are often mistakenly regarded as manifestations of vertebrogenic pathology. According to some studies, in approximately 9% of patients referred to the clinic with a diagnosis of radiculopathy, the cause of pain, sensory and motor disturbances in the lower extremities was actually traumatic and compression-ischemic neuropathies, a significant part of which (more than 10%) were various types of femoral neuropathy.
Diagnosis of lesions of the femoral nerve is primarily based on a thorough neurological examination and analysis of the distribution of sensory and/or motor disorders, identifying their correspondence to the area of innervation of the femoral nerve or its individual branches. At the same time, the topic of damage to the femoral nerve is determined, which, along with anamnestic data, allows us to suggest the etiology of the disease. In practice, femoral neuropathy most often has to be differentiated from vertebrogenic radiculopathies L2-L4. X-ray of the joints of the lower extremities is not of great importance for diagnosing the condition of the femoral and sciatic nerves due to the impossibility of their image. MRI allows you to clearly assess the condition of the corresponding part of the spine and suspect the presence of neuropathy, but does not provide images of the nerves along their length.
Incorrect diagnosis leads to partially or completely inadequate therapy, which, naturally, adversely affects the course of the disease and contributes to its chronicity. Meanwhile, the vast majority of cases of femoral neuropathy, subject to timely initiation and adequacy of treatment measures, are potentially curable. Elimination of the cause of damage to the femoral nerve and early pathogenetic therapy can avoid disabling outcomes, including intractable complex pain syndromes of the pelvic girdle and paresis of the anterior group of the thigh muscle with persistent impairment of walking function.
Pathological tension of the piriformis muscle due to compression of the L1 or S1 root, as well as due to injury, unsuccessful injection, prolonged lying on the back and side (during prolonged operations), posterior muscle compartment syndrome of the thigh can be a manifestation of sciatic nerve neuropathy [8]. The sciatic nerve may be compressed by a tumor or hematoma in the pelvic area, or an aneurysm of the iliac artery.
Therefore, the collaboration of neurologists, urologists, gynecologists, rheumatologists, and ultrasound doctors is so important for a more accurate and detailed differential diagnosis of neuropathies of the femoral and sciatic nerves.
The use of methods for radiological diagnosis of peripheral nerves of the lower limb is limited by the technical capabilities of the equipment and the anatomical features of the location of the nerves [6, 12, 13].
The decisive advantage of ultrasound of peripheral nerves is non-invasiveness, absence of radiation exposure to the patient, real-time examination, as well as minimal economic costs for the examination. Ultrasound allows not only to visualize the sciatic and femoral nerve along its entire length, but also to assess its location, thickness and structure, which in turn helps the neurologist to choose and promptly begin adequate treatment.
Conclusion
Thus, the use in the practice of a neurologist of the ultrasound method of studying nerves allows optimizing the differential diagnostic search for the causes of pain in the lower extremities, as well as minimizing the number of studies performed on a patient with neurological symptoms of peripheral origin, avoiding unnecessary manipulations and studies, reducing radiation exposure to the patient, reduce the cost of its examination and thereby increase the diagnostic efficiency of the studies.
Literature
- Popelyansky Ya.Yu. Orthopedic neurology (vertebroneurology). M.: MEDpress-inform, 2003.
- Popelyansky Ya.Yu. Diseases of the peripheral nervous system. M.: MEDpress-inform, 2005.
- Bianchi S., Martinoli C. Ultrasound of the Musculoskeletal System. Springer-Verlag Berlin Heidelberg New York 2007.
- Peer S., Bodner G. High-resolution ultrasound of the peripheral nervous system. Springer-Verlag Berlin Heidelberg 2008.
- Eskin N.A. Ultrasound diagnostics in traumatology and orthopedics // Ed. Mironova S.P. M.: Publishing house "Social and Political Thought", 2009.
- Saltykova V.G. Ultrasound examination technique and normal echographic picture of the sciatic nerve // Ultrasound and functional diagnostics. 2009. N 6. P. 75-81.
- Shtulman D.R., Levin O.S. Neurology: A Practitioner's Handbook. 5th ed., add. and processed M.: MEDpressinform, 2007. pp. 91-95.
- Samoilov V.I. Syndromological diagnosis of diseases of the nervous system. Volume 1, 2nd ed. St. Petersburg, “SpetsLit”, 2001.
- Khabirov F.A. Guide to clinical spinal neurology. Kazan: Medicine, 2006.
- Elman L., McCluskey L. Occupational and Sport Related Traumatic Neuropathy // The Neurologist. 2004. V. 10. P. 82-96.
- Durrant DH, True JM, Blum JW Myelopathy radiculopathy, and peripheral entrapment syndromes. CRC Press, 2002.
- Jacobson JA Fundamentals of musculoskeletal ultrasound, second edition 2013, 2007 by Saunders, an imprint of Elsevier Inc.
- McNally Eugene. Ultrasound studies of the musculoskeletal system: A practical guide // Transl. from English Khitrova A.N. / Ed. Nazarenko G.I., Geroeva I.B. M.: Vidar M Publishing House, 2007.
Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.
Clinical manifestations
Symptoms of the disease depend on the cause of the condition. If the process taking place in the iliopsoas region, motor, sensory and vegetative-dystrophic disorders develop throughout the entire innervation zone. Impairments may occur alone or as a combined combination of motor and sensory impairments.
Absolute neuropathy is accompanied by disruptions in the activity of the iliopsoas muscles due to the possibility of alternative innervation. The ability to rotate and flex the hip is maintained. The decrease in the potential of the quadriceps extensor muscle of the knee joint is significantly pronounced. The patient strives to keep his leg straight even while walking.
It is difficult to walk, especially up the stairs, as well as running. There is a change in gait. The lower limb on the corresponding side is stable in the hyperextension position. There is no knee reflex. Tactile and pain sensations are impaired in the anterior inner area of the thigh and lower leg, and the medial area of the foot.
The process is expressed in the form of trophic and vegetative disorders, pain of an irrigation nature. The Wasserman symptom is pronounced - lying on the stomach, the patient experiences pain in the anterior part of the thigh when trying to raise the straightened leg to the maximum height, as well as the Mickiewicz symptom - the inability to bend the leg at the knee joint.
If the process takes place in the inguinal ligament area, the symptoms are similar to those described above. The most common motor disorders are those accompanied by pain when pressing on the inguinal ligament. Compression of the femoral nerve shaft in Gunther's canal is accompanied by pain and numbness of the skin of the central part of the knee joint, the anterior inner surface of the leg and the inner part of the foot.
Spontaneously occurring pain and paresthesia intensify with extension of the leg. The patient keeps his legs bent in a standing position and when walking. The knee reflex is preserved. Tinel's symptom is clearly expressed - when tapped with a hammer, paresthesia passes along the saphenous nerve, significant pain is detected at the site where the nerve exits the conductive canal.
Symptoms
Doctors divide the chronic, acute and subacute course of axonal polyneuropathy. The disease is divided into two types: primary axonal and demyelinating. During the course of the disease, demyelination is added to it, and then a secondary axonal component.
The main manifestations of the disease include:
- weakness in the muscles of the legs or arms;
- spastic paralysis of the limbs;
- feeling of twitching in muscle fibers;
- dizziness with a sudden change in body position;
- swelling of the limbs;
- burning;
- tingling;
- crawling sensation;
- decreased sensitivity of the skin to high or low temperature, pain and touch;
- impaired speech clarity;
- problems with coordination.
The following symptoms are considered vegetative signs of sensorimotor polyneuropathy of the asconal type:
- rapid or, on the contrary, slow heart rate;
- excessive sweating;
- excessive dry skin;
- change in skin color;
- ejaculation disorder;
- erectile disfunction;
- problems with urination;
- failure of motor functions of the gastrointestinal tract;
- increased salivation or, conversely, dry mouth;
- eye accommodation disorder.
The disease manifests itself in dysfunction of damaged nerves. It is the peripheral nerve fibers that are responsible for the motor functions of muscle tissue, sensitivity, and also have a vegetative effect, that is, they regulate vascular tone.
Disorders of nerve conduction function are characterized by sensitivity disorders, for example:
- crawling sensation;
- hyperesthesia, that is, increased sensitivity of the skin to external irritants;
- hypoesthesia, that is, decreased sensitivity;
- lack of sensation of one's own limbs.
When autonomic fibers are affected, the regulation of vascular tone goes out of control. With axonal demyelinating polyneuropathy, compression of the capillaries occurs, causing the tissue to swell. The lower and then the upper limbs, due to the accumulation of fluid in them, significantly increase in size. Since with polyneuropathy of the lower extremities the main amount of blood accumulates in the affected areas of the body, the patient experiences persistent dizziness when taking an upright position. Due to the loss of trophic function, erosive and ulcerative lesions of the lower extremities may occur.
Axonal motor polyneuropathy manifests itself in motor disorders of the upper and lower extremities. When the motor fibers responsible for the movements of the arms and legs are damaged, complete or partial muscle paralysis occurs. Immobilization can manifest itself in a completely atypical manner - you can feel both stiffness of the muscle fibers and their excessive relaxation. With a moderate degree of damage, muscle tone is weakened.
During the course of the disease, tendon and periosteal reflexes may be strengthened or weakened. In rare cases, a neurologist does not observe them. The disease can often affect the cranial nerves, which are manifested by the following disorders:
- deafness;
- numbness of the sublingual muscles and tongue muscles;
- inability to swallow food or liquid due to problems with the swallowing reflex.
When the trigeminal, facial or oculomotor nerve is affected, the sensitivity of the skin changes, paralysis develops, facial asymmetry and muscle twitching occur. Sometimes, when axonal demyelinating polyneuropathy is diagnosed, the lesions of the upper or lower extremities may be asymmetrical. This happens with multiple mononeuropathy, when the knee, Achilles and carporadial reflexes are asymmetrical.
Diagnostics
For an accurate diagnosis, it is important to determine the cause of neuropathy. The conclusion is made by a neurologist after carefully collecting anamnesis and studying the results of instrumental research methods. X-ray of the spinal column is not a reliable diagnostic method, since identified spinal defects do not exclude the manifestation of neuropathy. EMG allows you to resolve controversial issues in making a diagnosis.
Neuropathy corresponds to the slow passage of impulses along the femoral nerve column, a decrease in the amplitude of the M-response, symptoms of impaired innervation in the corresponding muscles, as well as the muscles of the L2-L4 segments. Using ultrasound diagnostics, the integrity of the femoral nerve is traced, pathological neoplasms, swelling, adhesive-scar changes and degenerative phenomena are determined. The level of nerve mobility in the adductor canal is confirmed by ultrasound with dynamic tests.
Differential diagnosis is aimed at excluding radiculopathies of the lumbar vertebrae of vertebrogenic origin, lumbosacral plexopathy caused by diabetes mellitus, injuries and gonarthrosis of the knee joint. To differentiate diseases of the abdominal cavity, ultrasound, MRI or CT are performed.
Treatment
If the femoral column is compressed by abdominal tumors, surgical intervention is performed urgently. If a traumatic violation of the integrity of the nerve with interruption of its fibers is confirmed, surgical treatment is also performed. For other established causes of the pathology, conservative treatment is carried out aimed at eliminating swelling, restoring blood supply, metabolism of the femoral nerve, and eliminating pain.
Glucocorticoid drugs are prescribed for decongestant and anti-inflammatory purposes when the nerve fiber is compressed under the inguinal ligament or in the muscle canals. Blockades are performed in the compression zone with solutions of glucocorticoid drugs (hydrocortisone, diprospan) in a cocktail with local anesthetics (solutions of lidocaine, novocaine).
If nonsteroidal anti-inflammatory drugs in combination with analgesics do not relieve intense pain, treatment is supplemented with antidepressants (amitriptyline) and anticonvulsants (pregabalin, topiramate, gabapentin). To restore the normal functioning of the femoral nerve, it is advisable to prescribe medications to improve blood supply to nerve cells (nicotinic acid, pentoxifylline) and drugs that improve tissue metabolism (combined forms of vitamins B6, B1).
To prevent muscle contractures and atrophies in cases of detected paresis of the quadriceps muscle and lumbosacral muscles, it is advisable to prescribe a complex of exercise therapy, electrical stimulation physiotherapy, and prescribe medications that restore the transmission of neuromuscular impulses (ipidacrine, neostigmine).
Methods and goals of therapy
Regardless of the cause of the disease, therapy includes the use of medications:
- Anti-inflammatory tablets, ointments, injections - relieve pain and reduce inflammation.
- Diuretics – to eliminate swelling.
- Medicines to improve blood circulation.
- Antispasmodics – to relieve tension in muscles and blood vessels.
- B vitamins.
Depending on the causes of the disease, treatment may be supplemented with:
- antibiotics - when an infectious process is attached;
- antiviral – for viral nerve damage;
- sedatives - with increased emotional stress.
Therapy for neuritis should be comprehensive and include physiotherapeutic procedures:
- UHF – relieves inflammation.
- Pulsed currents have an analgesic effect.
- Acupuncture – relieves swelling, restores sensitivity to nerve cells, improves blood circulation.
- Massage : acupressure, cupping.
- Magnetic therapy – improves blood circulation, reduces sensitivity, accelerates regeneration.
- Ultrasound therapy – restores sensitivity.
- Laser therapy – increases blood flow, promotes better penetration of nutrients and medications to their destination.
- Therapeutic gymnastics – used in the rehabilitation process, restores mobility and sensitivity of the damaged area.
If the above methods are ineffective, the doctor may prescribe surgical treatment. Surgically, the affected nerve is freed from the influence of surrounding tissues and its damaged fibers are sutured.